Introduction and Historical Context
Before the seminal descriptions of talocalcaneal coalitions by Harris and Beath, the clinical entity of rigid pes planus—with or without accompanying peroneal spasm—had not been definitively attributed to a structural anomaly between the talus and the calcaneus. Harris and Beath revolutionized the understanding of hindfoot pathology by reporting a “talocalcaneal bridge” of bone spanning the sustentaculum tali and the talus in 12 of 17 feet presenting with “peroneal spastic pes planus.” Since their initial report, extensive clinical series and advanced imaging modalities have unequivocally confirmed their findings, establishing talocalcaneal coalition as a primary etiology of rigid flatfoot in the adolescent and young adult populations.
Talocalcaneal coalitions represent a failure of mesenchymal segmentation during embryonic development, resulting in an abnormal connection (bony, cartilaginous, or fibrous) between the talus and calcaneus. This condition profoundly alters hindfoot kinematics, leading to adaptive changes, pain, and progressive arthrosis if left untreated.
Pathoanatomy and Biomechanics
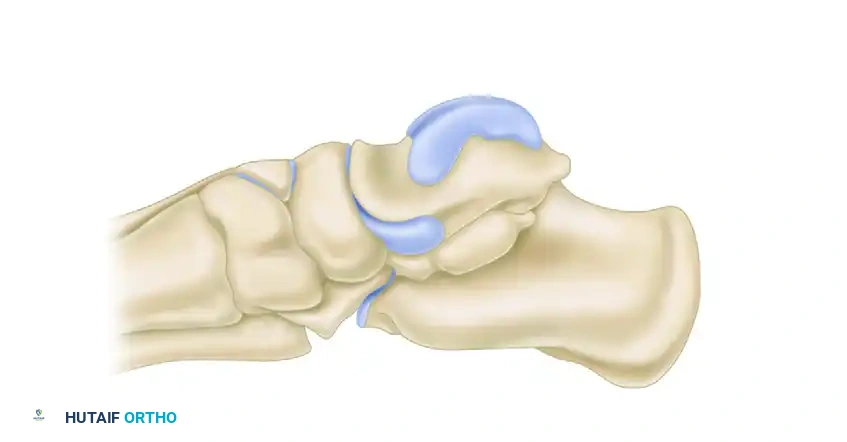
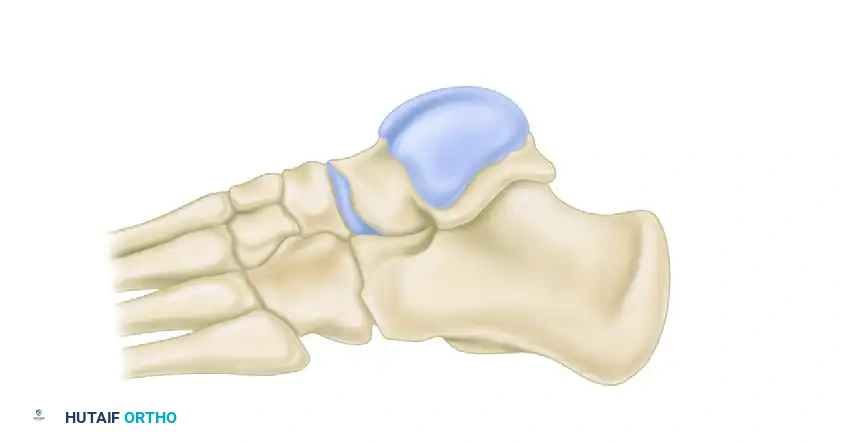
The subtalar joint functions as a complex, multi-axial "mitered hinge" that translates tibial rotation into foot pronation and supination. A talocalcaneal coalition, which most frequently involves the middle facet, rigidly locks this articulation.
Clinical Pearl: The loss of subtalar motion forces the transverse tarsal joint (talonavicular and calcaneocuboid joints) to absorb the torsional stresses of gait. This abnormal stress transfer is the primary driver of the classic "talar beak" seen on lateral radiographs, which is a traction osteophyte at the insertion of the talonavicular capsule, rather than a true degenerative osteophyte.
Ossification Timeline
The talocalcaneal bridge ossifies either completely or incompletely when an individual is between 12 and 16 years of age. This is notably later than the ossification of a calcaneonavicular bar (which typically ossifies between 8 and 12 years of age). Consequently, talocalcaneal coalitions are usually diagnosed in older adolescents or adults, coinciding with the onset of ossification which drastically reduces the compliance of the coalition and precipitates symptoms.
Clinical Presentation
The clinical presentation of a talocalcaneal coalition is hallmark, though it requires a high index of suspicion, particularly in the adolescent athlete presenting with recurrent "ankle sprains" or vague hindfoot pain.
Symptoms
- Insidious Hindfoot Pain: Patients typically report deep, aching pain around the hindfoot and sinus tarsi that exacerbates with weight-bearing activities, prolonged standing, or walking on uneven terrain.
- Foot Fatigue: A generalized sense of early foot fatigue is common.
- Arch Collapse: While a loss of the longitudinal arch is frequently present, it is rarely the patient's primary complaint.
Physical Examination Signs
- Absent Subtalar Motion: The cardinal sign on physical examination is a marked reduction or complete absence of subtalar motion. This contrasts with a calcaneonavicular bar, which may still allow varying degrees of subtalar mobility.
- Peroneal Spasm: Often termed "peroneal spastic flatfoot," this is not a true upper motor neuron spasticity but rather an adaptive, protective muscle spasm of the peroneal musculature attempting to splint the painful subtalar joint.
- Rigid Pes Planus: Heel valgus and loss of the normal longitudinal arch occur in varying severity. Crucially, the arch does not reconstitute upon toe-standing (Jack's test is negative), indicating a rigid deformity.
- Localized Tenderness: Palpation often elicits tenderness in the sinus tarsi, over the talonavicular joint, along the peroneal tendon sheath, and most specifically, medially over the sustentaculum tali.
Radiographic Evaluation
Standardizing radiographic diagnosis for talocalcaneal coalition is notoriously difficult due to normal variations in the osseous anatomy of the hindfoot.
Plain Radiography
The standard radiographic series should include weight-bearing anteroposterior, lateral, and oblique views of the foot.

Standing lateral radiograph of the right foot. Note the middle facet tarsal coalition with prominent talar beaking.
Helpful Radiographic Signs on Lateral View:
1. Talar Beaking: Beaking of the anterior aspect of the head/neck of the talus at the dorsal articular margin.
2. Broadening of the Lateral Process: Rounding or broadening of the lateral process of the talus as it impinges on the calcaneal sulcus.
3. C-Sign of Lateur: A continuous C-shaped line formed by the medial outline of the talar dome and the posteroinferior outline of the sustentaculum tali.
4. Joint Space Narrowing: Narrowing of the posterior talocalcaneal joint space and loss of the middle subtalar joint visibility.
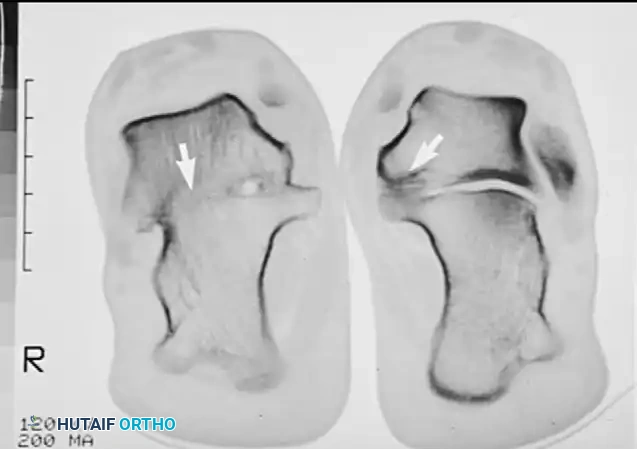
The Harris and Beath View (Coalition View):
This posterosuperior oblique projection is designed to pass between the sustentaculum tali and the neck of the talus.
* Technique: The patient stands on the cassette with knees flexed sufficiently to remove the calf shadow from the beam. The cone is angled toward the heel.
* Optimal Angulation: Because the medial and posterior subtalar joint facets normally lie in highly variable planes (35° to 45° and 45° to 60° to the long axis of the calcaneus, respectively), multiple views are often required. Angles of 35, 40, and 45 degrees to the long axis of the calcaneus are the most common angles utilized to demonstrate the coalition.

Angles of middle and posterior subtalar facets demonstrating the high variability in normal hindfoot anatomy.
Diagrammatic representation of the posterior facet orientation.
Further diagrammatic representation of the posterior facet.
In a positive talocalcaneal coalition, the joint space on the Harris-Beath view is replaced by a solid bony bridge, or the distinct articular margins are lost, implying a fibrous or cartilaginous bridge.
Advanced Imaging: Computed Tomography (CT)
CT is the undisputed gold standard for the diagnosis and surgical planning of talocalcaneal coalitions.
Surgical Warning: Instructions to the radiography technician must be explicit. The primary cuts of the CT must be perpendicular to the posterior and middle facets of the subtalar joint (the semicoronal plane) at 3-mm increments. Standard axial or sagittal cuts may miss a subtle middle facet coalition.

Semicoronal CT scan clearly demonstrating a middle facet talocalcaneal coalition.
CT not only confirms the diagnosis but defines the exact location, size, and margins of the coalition. It is critical for assessing the condition of the remaining subtalar articulations at the posterior facet.

Semicoronal CT scan demonstrating bilateral middle facet coalitions. Bilateral involvement is common and must always be ruled out.
Magnetic Resonance Imaging (MRI)
While CT sets the standard for bony architecture, MRI is highly sensitive and may be helpful in depicting fibrous or cartilaginous coalitions before they ossify, presenting as bone marrow edema across the suspected coalition site.
Non-Operative Management
A trial of conservative treatment is universally recommended as the first-line approach, particularly for newly diagnosed, symptomatic patients without severe degenerative changes.
Conservative Modalities:
1. Immobilization: 4 to 6 weeks in a short-leg walking cast or controlled ankle motion (CAM) boot to completely rest the subtalar joint and break the cycle of peroneal spasm.
2. Orthotics: Following cast removal, transition to firm, custom-molded medial longitudinal arch supports or a University of California Biomechanics Laboratory (UCBL) orthosis to control hindfoot valgus.
3. Pharmacotherapy: NSAIDs for inflammatory control.
4. Corticosteroid Injection: An image-guided injection into the sinus tarsi or the subtalar joint can provide significant diagnostic information and therapeutic relief.
If this comprehensive conservative regimen fails to provide durable relief, operative intervention is indicated.
Surgical Management
Surgical decision-making is dictated by the patient's age, the size of the coalition, and the presence of secondary degenerative arthrosis in the hindfoot.
1. Resection of the Talocalcaneal Coalition
In younger patients (typically 9 to 15 years old) with a symptomatic middle facet tarsal coalition and no degenerative changes, resection of the bar with interpositional arthroplasty is the treatment of choice.
Indications for Resection:
* Patient age typically < 16 years (though successful resections in patients in their 20s and 30s are reported).
* Coalition size < 50% of the total subtalar joint surface area.
* The bar measures no more than 2 to 3 cm in length on 3-mm CT cuts.
* Absence of advanced talonavicular or posterior facet arthrosis.
Surgical Technique: Medial Approach
1. Positioning: The patient is placed supine with a bump under the contralateral hip to externally rotate the operative leg, providing excellent access to the medial hindfoot. A thigh tourniquet is applied.
2. Incision: A longitudinal medial incision is made centered over the sustentaculum tali, extending from the medial malleolus toward the navicular tuberosity.
3. Dissection: The flexor retinaculum is incised. The posterior tibial tendon (PTT) is retracted dorsally, and the flexor digitorum longus (FDL) is retracted plantarward. The neurovascular bundle and the flexor hallucis longus (FHL) must be meticulously identified and protected plantarly.
4. Exposure of the Coalition: The periosteum over the sustentaculum tali is elevated. The coalition is usually immediately apparent as a continuous bridge of bone lacking a normal joint line.
5. Resection: Using a combination of osteotomes, rongeurs, and a high-speed burr, the coalition is resected. Resection must proceed laterally until normal, healthy articular cartilage of the posterior facet is visualized, and a clear space is established between the talus and calcaneus.
6. Interposition: To prevent recurrence (re-ossification), an interpositional material must be placed into the defect. Options include:
* Bone wax applied to the raw cancellous surfaces.
* A pedicled graft of the local medial adipose tissue.
* A split portion of the FHL tendon.
7. Closure: The retinaculum and skin are closed in layers.
Postoperative Protocol for Resection:
* 0-2 weeks: Non-weight-bearing in a splint.
* 2-6 weeks: Transition to a CAM boot. Initiate early, aggressive active and passive subtalar range of motion exercises to prevent scarring and maintain the newly created joint space.
* 6+ weeks: Progressive weight-bearing and physical therapy focusing on peroneal strengthening and proprioception.
2. Subtalar Arthrodesis
In older adolescents or adults where the coalition is large (>50% of the joint), or if isolated subtalar arthrosis is present without midtarsal involvement, an isolated subtalar arthrodesis is highly effective.
Surgical Technique:
* The subtalar joint is approached laterally.
* The remaining cartilage is denuded from the posterior facet.
* The rigid, bony, or fibrous talocalcaneal bar is resected sufficiently to allow correction of the heel valgus.
* The joint is rigidly fixed using one or two large-diameter (6.5 mm or 7.3 mm) cannulated screws placed from the calcaneal tuberosity into the talar dome.
* Clinically, the patient’s pain and tenderness around the medial and lateral margins of the subtalar joint usually improve dramatically following solid fusion.
3. Triple Arthrodesis
In older patients, particularly those in whom long-standing altered biomechanics have led to advanced degenerative changes at the talonavicular joint, calcaneocuboid joint, or both, a triple arthrodesis is the definitive procedure.
Indications:
* Failed prior resection.
* Advanced patient age with rigid deformity.
* Significant transverse tarsal arthrosis (talonavicular and calcaneocuboid joints).
Surgical Technique:
1. Approaches: The procedure is typically performed through a standard anterolateral (Ollier) approach to access the posterior facet of the subtalar joint and the calcaneocuboid joint. This is supplemented by a medial utility incision to expose the medial aspect of the talonavicular joint and the coalition at the sustentaculum tali.
2. Joint Preparation: The articular cartilage of the subtalar, talonavicular, and calcaneocuboid joints is meticulously debrided down to bleeding subchondral bone.
3. Deformity Correction: The talocalcaneal coalition is resected via the medial approach to mobilize the hindfoot, allowing correction of the fixed valgus and restoration of the longitudinal arch.
4. Fixation: Rigid internal fixation is achieved. Typically, large cannulated screws are used for the subtalar and talonavicular joints, while screws or staples may be used for the calcaneocuboid joint.

Lateral radiograph several years after a successful triple arthrodesis. Note the solid fusion mass and restoration of hindfoot alignment.
Coronal CT scans after triple arthrodesis of the right foot, demonstrating complete bony consolidation across the subtalar joint. The left foot remains untreated.
Postoperative Protocol for Arthrodesis:
* 0-6 weeks: Strict non-weight-bearing in a short-leg cast.
* 6-12 weeks: Progressive weight-bearing in a CAM boot, pending radiographic evidence of consolidation.
* 12+ weeks: Transition to regular footwear, often with a supportive orthotic.
Complications and Outcomes
Following Resection:
* Recurrence: Re-ossification of the bar is the most common complication, minimizing this requires adequate initial resection (until normal cartilage is seen) and meticulous interposition.
* Nerve Injury: The medial calcaneal branches or the main posterior tibial nerve can be injured during the medial approach.
* Persistent Pain: Often due to unrecognized pre-existing arthrosis or incomplete resection.
Following Arthrodesis:
* Nonunion: Particularly at the talonavicular joint, which has the highest nonunion rate in a triple arthrodesis.
* Adjacent Segment Disease: Long-term follow-up of triple arthrodesis often reveals progressive arthrosis of the ankle joint or midfoot due to the transfer of mechanical stress.
Conclusion
Talocalcaneal coalition is a complex structural anomaly that demands a thorough clinical evaluation and precise radiographic workup, heavily reliant on semicoronal CT imaging. While conservative measures play a role in initial management, surgical intervention is frequently required. The paradigm of treatment relies on joint-preserving resection in the young patient with a localized middle facet bar, shifting toward definitive arthrodesis in the older patient or in the presence of degenerative joint disease. Mastery of the complex medial hindfoot anatomy and rigorous adherence to surgical indications are paramount for achieving excellent, pain-free functional outcomes.
📚 Medical References
- Talocalcaneal coalition treated with resection, J Pediatr Orthop 7:513, 1987.
- Gonzalez P, Kumar SJ: Calcaneonavicular coalition treated by resection and interposition of the extensor digitorum brevis muscle, J Bone Joint Surg 72A:71, 1990.
- Harris RI: Rigid valgus foot due to talocalcaneal bridge, J Bone Joint Surg 37A:169, 1955.
- Harris RI, Beath T: Etiology of peroneal spastic fl atfoot, J Bone Joint Surg 30B:624, 1948.
- Herzenberg JE, Goldner JL, Martinez S, et al: Computerized tomography of talocalcaneal tarsal coalition: a clinical and anatomic study, Foot Ankle 6:273, 1986.
- Kumar SJ, Cowell HR, Ramsey PL: Foot problems in children, I: vertical and oblique talus, Instr Course Lect 31:235, 1982.
- Kumar SJ, Guille JT, Lee MS, et al: Osseous and nonosseous coalition of the middle facet of the talocalcaneal joint, J Bone Joint Surg 74A:519, 1992.
- Mazzocca AD, Thompson JD, Deluca PA, et al: Comparison of the posterior approach versus the dorsal approach in the treatment of congenital vertical talus, J Pediatr Orthop 21:202, 2001.
- Swiontkowski MF, Scranton PE, Hansen S: Tarsal coalitions: long-term results of surgical treatment, J Pediatr Orthop 3:287, 1983.
- Takakura Y, Sugimoto K, Tanaka Y, et al: Symptomatic talocalcaneal coalition: its clinical signifi cance and treatment, Clin Orthop Relat Res 269:249, 1991.
- Warren MJ, Jeffree MA, Wilson DJ, et al: Computed tomography in suspected tarsal coalition: examination of 26 cases, Acta Orthop Scand 61:554, 1990.
- Congenital Angular Deformities of the Leg and Congenital Pseudarthrosis Adamsbaum C, Kalifa G, Seringe R, Bonnet JC: Minor tibial duplication: a new cause of congenital bowing of the tibia, Pediatr Radiol 21:185, 1991.
- Aegerter EE: The possible relationship of neurofi bromatosis, congenital pseudarthrosis, and fi brous dysplasia, J Bone Joint Surg 32A:618, 1950.
- Andersen KS: Congenital angulation of the lower leg and congenital pseudarthrosis of the tibia in Denmark, Acta Orthop Scand 43:539, 1972.
- Anderson DJ, Schoenecker PL, Sheridan JJ, et al: Use of an intramedullary rod for the treatment of congenital pseudarthrosis of the tibia, J Bone Joint Surg 74A:161, 1992.
- Badgley CE, O’Connor SJ, Kudner DF: Congenital kyphoscoliotic tibia, J Bone Joint Surg 34A:349, 1952.
- Baker JK, Cain TE, Tullos HS: Intramedullary fi xation for congenital pseudarthrosis of the tibia, J Bone Joint Surg 74A:169, 1992.
- Boyd HB: Congenital pseudarthrosis: treatment by dual bone grafts, J Bone Joint Surg 23:497, 1941.
- Boyd HB: Pathology and natural history of congenital pseudarthrosis of the tibia, Clin Orthop Relat Res 166:5, 1982.
- Boyd HB, Fox KW: Congenital pseudarthrosis: follow-up study after massive bone-grafting, J Bone Joint Surg 30A:274, 1948.
- Boyd HB, Sage FP: Congenital pseudarthrosis of the tibia, J Bone Joint Surg 40A:1245, 1958.
- Charnley J: Congenital pseudarthrosis of the tibia treated by the intramedullary nail, J Bone Joint Surg 38A:283, 1956.
- Crossett LS, Beaty JH, Betz RR, et al: Congenital pseudarthrosis of the tibia: long-term follow-up study, Clin Orthop Relat Res 245:16, 1989.
- Dal Monte A, Donzelli O, Sudanese A, et al: Congenital pseudarthrosis of the fi bula, J Pediatr Orthop 7:14, 1987.
- Dooley BJ, Menelaus MB, Paterson DC: Congenital pseudarthrosis and bowing of the fi bula, J Bone Joint Surg 56B:739, 1974.
- Dormans JP, Krajbich JI, Zuker RM, et al: Congenital pseudarthrosis of the tibia: treatment with free vascularized fi bular grafts, J Pediatr Orthop 10:623, 1990.
- Gilbert A, Brockman R: Congenital pseudarthrosis of the tibia: long-term follow-up of 29 cases treated by microvascular bone transfer, Clin Orthop Relat Res 314:37, 1995.
- Goldberg I, Maor P, Yosipovitch Z: Congenital pseudarthrosis of the tibia treated by a pedicled vascularized graft of the ipsilateral fi bula: a case report, J Bone Joint Surg 70A:1396, 1988.
- Gordon L, Weulker N, Jergensen H: Vascularized fi bular grafting for the treatment of congenital pseudarthrosis of the tibia, Orthopedics 9:825, 1986.
- Grill F, Bollini G, Dungl P, et al: Treatment approaches for congenital pseudarthrosis of tibia: results of the EPOS multicenter study. European Paediatric Orthopaedic Society (EPOS), J Pediatr Orthop 9B:75, 2000.
- Grogan DP, Love SM, Ogden JA: Congenital malformations of the lower extremities, Orthop Clin North Am 18:537, 1987.
- Hefti F, Bollini G, Dungl P, et al: Congenital pseudarthrosis of the tibia: history, etiology, classifi cation, and epidemiologic data, J Pediatr Orthop B 9:11, 2000.
- Heikkinen ES, Poyhonen MH, Kinnunen PK, et al: Congenital pseudarthrosis of the tibia: treatment and outcome at skeletal maturity in 10 children, Acta Orthop Scand 70:275, 1999.
- Heyman CH, Herndon CH, Heiple KG: Congenital posterior angulation of the tibia with talipes calcaneus: a long-term report of eleven patients, J Bone Joint Surg 41A:476, 1959.
- Hsu LCS, O’Brien JP, Yau ACMC, et al: Valgus deformity of the ankle in children with fi bular pseudarthrosis: results of treatment by bone-grafting of the fi bula, J Bone Joint Surg 56A:503, 1974.
- Ilizarov GA: The principles of the Ilizarov method, Bull Hosp Jt Dis 48:1, 1988.
- Johnstone CE 2nd: Congenital pseudarthrosis of the tibia: results of technical variations in the Charnley-Williams procedure, J Bone Joint Surg 84A:176, 2002.
- Inan M, ElRassi G, Riddle EC, Kumar SJ: Residual deformities following successful initial bone union in congenital pseudoarthrosis of the tibia, J Pediatr Orthop 26:393, 2006.
- Joseph B, Mathew G: Management of congenital pseudarthrosis of the tibia by excision of the pseudarthrosis, onlay grafting, and
