Introduction to Talar Fractures
The role of the talus in lower extremity function, the sheer complexity of its anatomy, and the high variability of fracture patterns frequently complicate the treatment of talar fractures, presenting a formidable challenge to orthopedic surgeons. Functioning as the critical intercalated segment between the leg and the foot, the talus transmits the entire weight of the body across the ankle, subtalar, and talonavicular joints. Because approximately 60% of its surface area is covered by articular cartilage and it lacks any direct muscular or tendinous attachments, the talus relies entirely on a tenuous extraosseous vascular sling and ligamentous soft-tissue envelope.
To gain full confidence in the treatment of these injuries, the orthopedic surgeon must possess a thorough, three-dimensional knowledge of the osseous and vascular anatomy, extensive experience with modern methods of rigid internal fixation, and the clinical acumen to anticipate and manage the severe complications—such as avascular necrosis (AVN) and post-traumatic arthrosis—that frequently accompany talar trauma.
Osseous and Vascular Anatomy
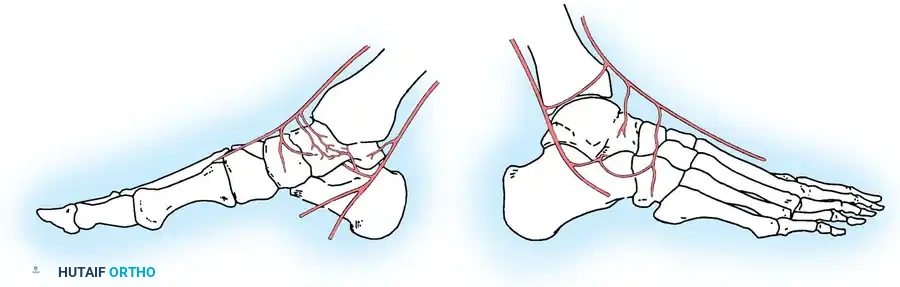
The vascular anatomy of the talus has been extensively mapped by pioneers such as McKeever (1943), Wildenauer (1950), Haliburton et al. (1958), Mulfinger and Trueta (1970), and Gelberman and Mortensen (1983). The three major arteries of the lower leg—the posterior tibial, anterior tibial (dorsalis pedis), and peroneal arteries—contribute to a rich, extraosseous anastomotic plexus that supplies blood to the head, neck, and body of the talus.
The Extraosseous Arterial Plexus
The head and neck regions are richly supplied by the superior neck vessels, which branch off the dorsalis pedis artery and the artery of the sinus tarsi. Because of this robust collateral network, osteonecrosis of the talar head and neck is extremely rare.
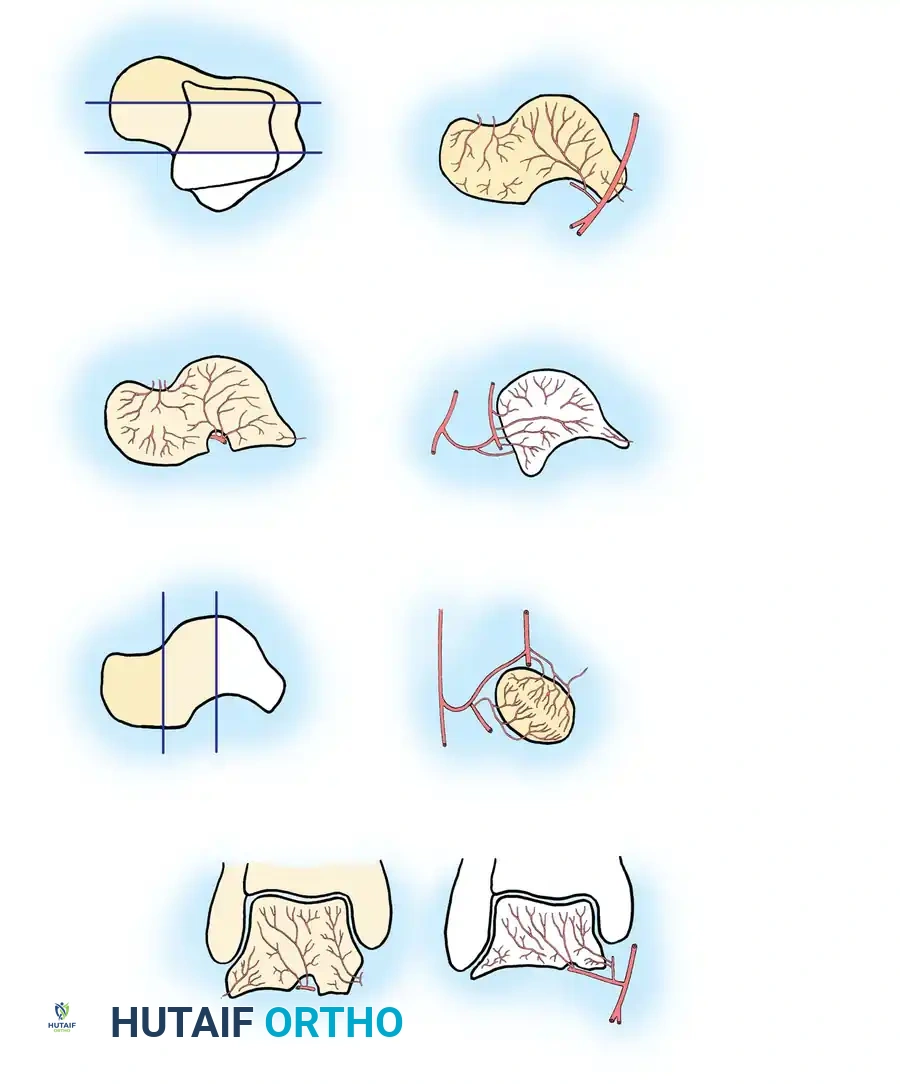
The vascular supply to the highly vulnerable talar body is summarized as follows:
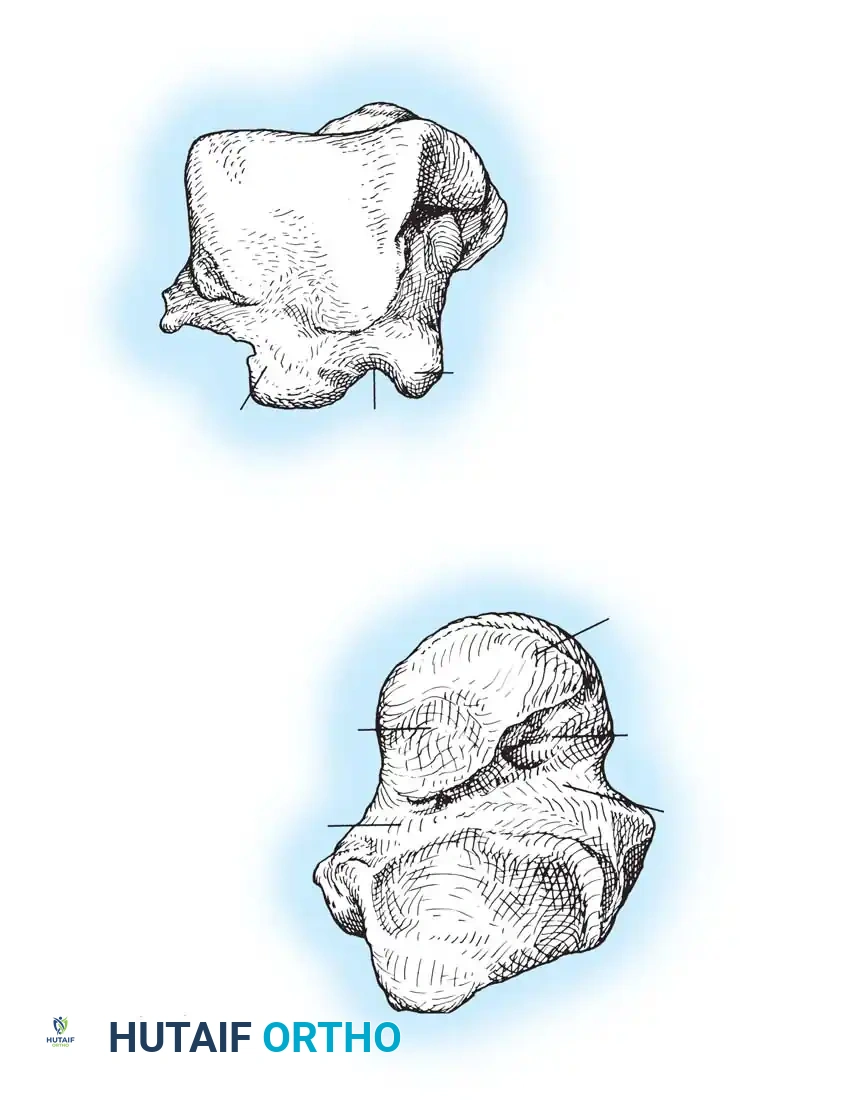
- Artery of the Tarsal Canal: This is the most consistent and major supplier of blood to the talar body. It branches off the posterior tibial artery approximately 1 cm proximal to its bifurcation into the medial and lateral plantar arteries. It courses through the tarsal canal (formed by the inferior sulcus of the talus and the superior sulcus of the calcaneus) from posteromedial to anterolateral. Within the canal, it sends four to six direct perforating vessels into the body of the talus.
- Deltoid Artery: Branching directly off the artery of the tarsal canal, the deltoid artery supplies the medial one-fourth to one-half of the talar body. Through extensive intraosseous anastomoses, it has the potential to supply a much greater area. In severe fracture-dislocations, the deltoid branch may be the only remaining blood supply to the extruded talar body.
- Artery of the Sinus Tarsi: Highly variable in size and origin, this artery supplies the lateral one-eighth to one-fourth of the talar body. It is formed by branches of the perforating peroneal artery, the dorsalis pedis (or anterior tibial) artery, or an anastomosis between the two. It anastomoses with the artery of the tarsal canal to form a vascular sling under the talar neck.
- Posterior Tubercle Vessels: The posterior tubercle is supplied by direct branches from the posterior tibial artery or the peroneal artery. Though small, intraosseous anastomoses allow this region to contribute to the body's perfusion.
Surgical Warning: The talar body is exceptionally vulnerable to ischemia. Osteonecrosis rates approach 100% in completely extruded talar body fractures due to the catastrophic disruption of the artery of the tarsal canal, the artery of the sinus tarsi, and the deltoid branches. Surgical approaches must meticulously preserve the medial soft tissues to protect the deltoid artery.
Talar Head Fractures
Fractures of the head of the talus constitute approximately 5% to 10% of all talar injuries. They are critical injuries because the talar head forms the keystone of the medial longitudinal arch and articulates with the navicular to facilitate essential hindfoot inversion and eversion.
Mechanism of Injury and Diagnosis
Two primary mechanisms of injury are recognized:
1. Axially directed loading and compression of the talar head against the navicular.
2. A dorsal compression fracture resulting from impingement against the anterior tibial plafond during extreme dorsiflexion.
A high index of suspicion must be maintained for any patient presenting with post-traumatic tenderness in the anterior ankle or midfoot region, as these fractures are notoriously difficult to identify on standard radiographs. While plain films may suggest the injury, a fine-cut Computed Tomography (CT) scan is mandatory for definitive diagnosis, evaluation of articular comminution, and surgical planning.

Surgical Management of Talar Head Fractures
Displaced fractures of the talar head require Open Reduction and Internal Fixation (ORIF) to restore the congruity of the talonavicular joint and the stability of the triple joint complex.
Surgical Approach:
An anteromedial approach is utilized, making the incision medial to the anterior tibial tendon.
* Soft Tissue Handling: Extreme care must be taken not to strip the dorsal capsular attachments, which carry the remaining vascular supply to the head fragment.
* Fixation: Stable fixation is achieved using countersunk, partially threaded cancellous lag screws (typically 3.5 mm or 4.0 mm) or headless, fully threaded compression screws to avoid impingement within the talonavicular joint.
Postoperative Protocol:
If rigid fixation is achieved, early range of motion (ROM) of the ankle and subtalar joints can be initiated at 2 weeks postoperatively. Weight-bearing is strictly delayed for a minimum of 6 to 8 weeks. If fixation is marginal due to comminution, the patient is placed in a non-weight-bearing short leg cast for 6 weeks.
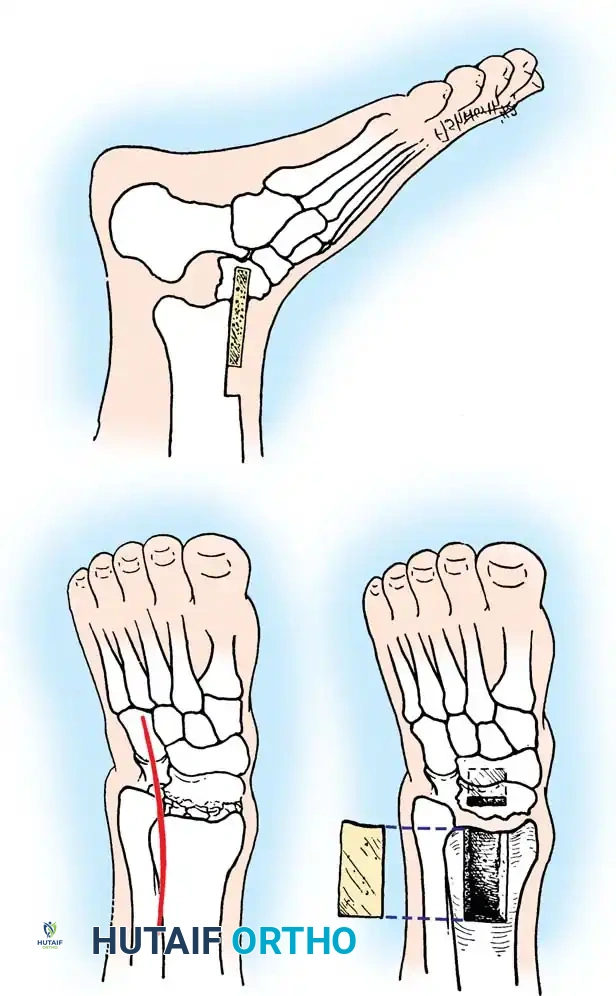
Clinical Pearl: Osteonecrosis of the talar head occurs in roughly 10% of cases. If severe post-traumatic degenerative arthrosis develops, a talonavicular arthrodesis may be indicated. However, isolated talonavicular arthrodesis eliminates nearly all motion in the triple joint complex. To prevent medial column shortening and a resultant varus hindfoot deformity, an inlay tricortical bone graft (as described by Adelaar) should be utilized during the fusion.
Talar Neck Fractures
Talar neck fractures are fraught with controversy regarding assessment, optimal surgical approaches, fixation constructs, and the management of frequent postoperative complications. First termed "aviator’s astragalus" by Anderson in 1919 after observing Royal Flying Corps pilots who crashed with their feet braced against the rudder pedals, these injuries typically result from high-energy axial loading with forced dorsiflexion.
The Hawkins Classification System
In 1970, Hawkins published a landmark review of 57 talar neck fractures. His classification system remains the universal standard today, providing critical prognostic guidelines for the development of osteonecrosis (AVN).
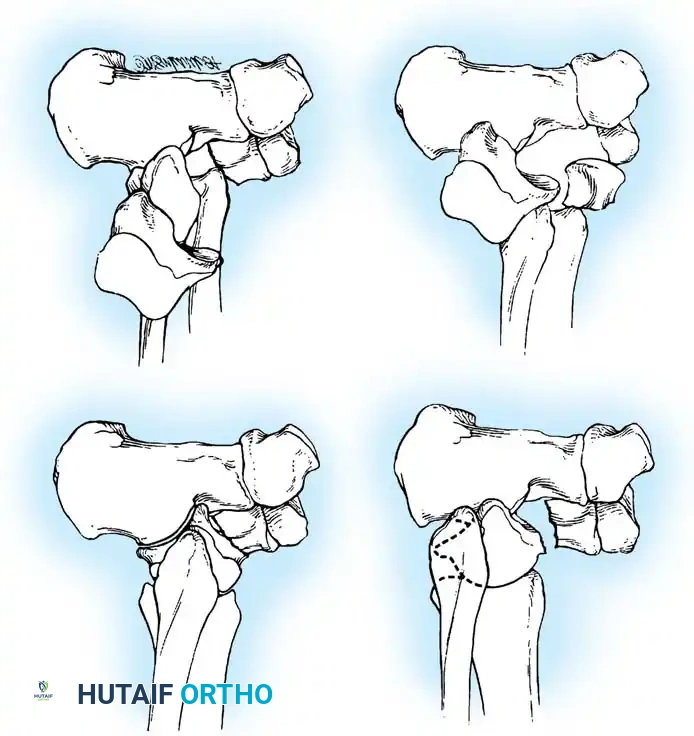
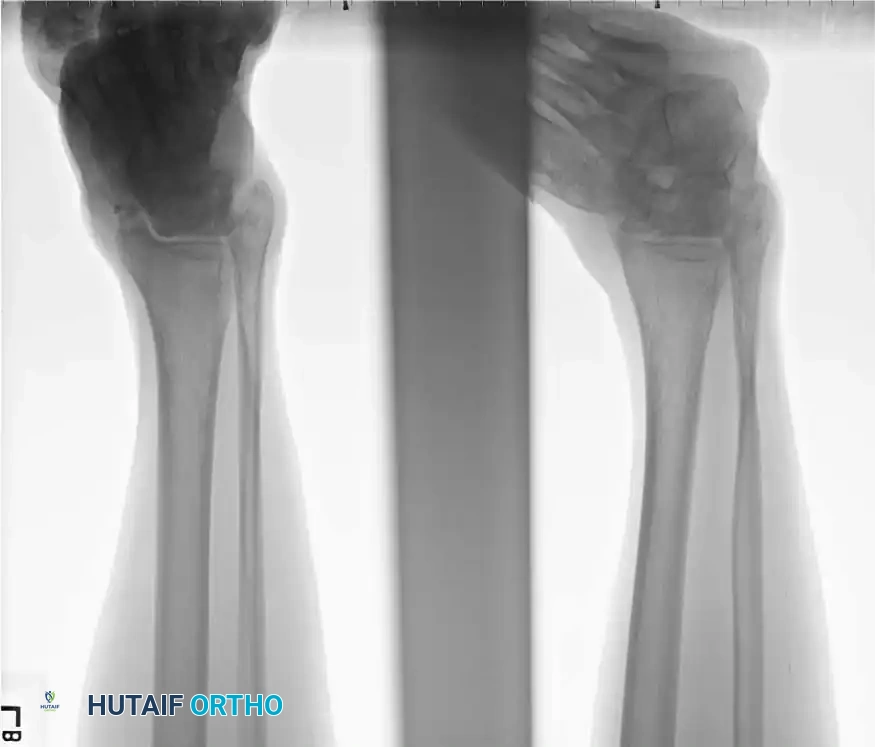
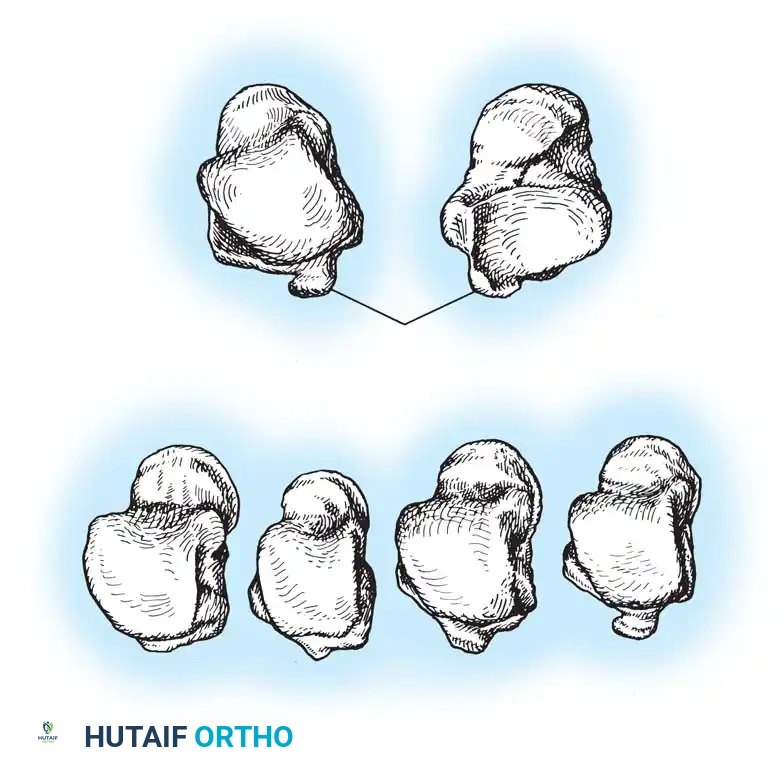
- Type I: Nondisplaced vertical fracture of the talar neck. The subtalar, tibiotalar, and talonavicular joints remain congruous. AVN risk is historically 0-10%.
- Type II: Displaced fracture of the talar neck with subluxation or dislocation of the subtalar joint. The ankle joint remains aligned. AVN risk is 20-50%.
- Type III: Displaced fracture of the talar neck with dislocation of both the subtalar and tibiotalar (ankle) joints. The talar body is often extruded posteromedially. AVN risk is 50-90%.
- Type IV: (Added later by Canale and Kelly). Displaced fracture of the talar neck with dislocation of the subtalar, tibiotalar, and talonavicular joints. The head of the talus is subluxed or dislocated. AVN risk approaches 100%.
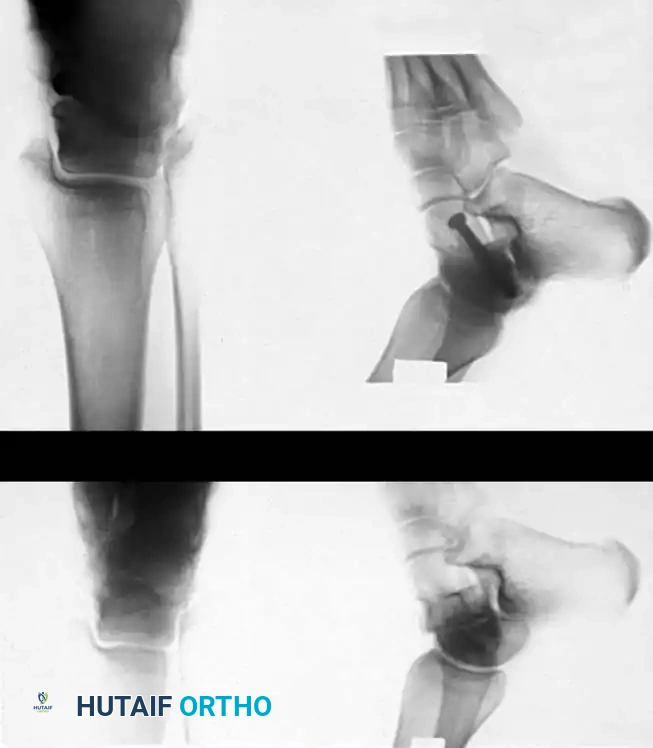
Radiographic Evaluation
Standard trauma radiographs must include anteroposterior (AP), lateral, and mortise views of the ankle, alongside an AP, lateral, and oblique of the foot.
The Canale View:
Intraoperatively and postoperatively, the Canale view is indispensable for profiling the talar neck and assessing for varus malreduction. The foot is maximally plantarflexed and internally rotated 15 degrees, with the X-ray beam angled 75 degrees cephalad from the horizontal plane.
Surgical Management of Talar Neck Fractures
Any fracture involving a weight-bearing joint surface demands anatomical reduction, and the talus is no exception. More weight per unit of area is borne by the superior dome of the talus than by any other bone in the human body.
Type I Fractures (Nondisplaced)
A talar neck fracture must be exhaustively evaluated before being definitively labeled as Type I. Subtle displacement is easily missed on plain radiographs; therefore, a CT scan is mandatory to confirm true non-displacement. If confirmed, treatment consists of immobilization in a non-weight-bearing below-knee cast for 8 to 12 weeks. Weight-bearing is only permitted once radiographic trabeculation across the fracture site is evident.
Types II, III, and IV Fractures (Displaced)
Displaced talar neck fractures are orthopedic emergencies, particularly Type III and IV injuries where the extruded talar body places severe tension on the neurovascular bundle and the skin. Immediate closed reduction should be attempted in the emergency department. If unsuccessful, emergent operative intervention is required.
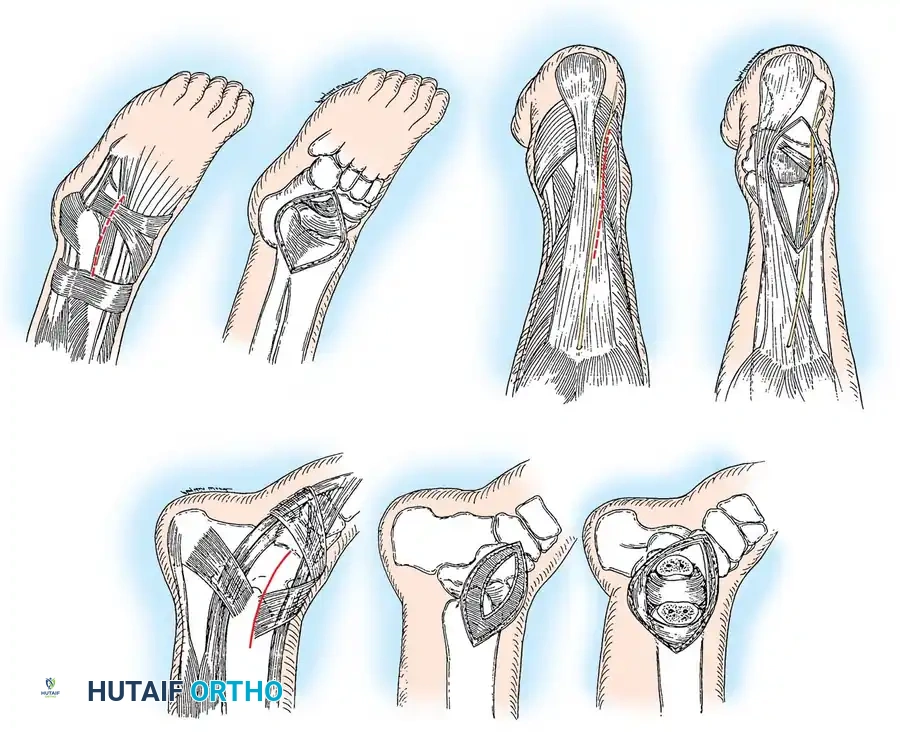
Surgical Approaches:
Modern treatment dictates early open reduction and rigid internal fixation. A dual-incision technique (anteromedial and anterolateral) is highly recommended to adequately visualize the fracture, debride interposed debris, and prevent the dreaded varus malunion.

- Anteromedial Approach: An incision is made medial to the tibialis anterior tendon, extending from the medial malleolus to the navicular. This exposes the medial talar neck. Crucial: Dissection must not extend inferiorly to the deltoid ligament, as this protects the critical deltoid arterial branches supplying the talar body.
- Anterolateral Approach: An incision is made in line with the fourth ray, lateral to the extensor digitorum longus (EDL) and superficial peroneal nerve. This allows visualization of the lateral talar neck and the subtalar joint.
Pitfall: Relying solely on a medial approach often leads to a varus malunion. The medial cortex is frequently comminuted. If compressed without restoring the lateral column length (visualized via the anterolateral approach), the talar neck collapses into varus, leading to devastating loss of subtalar eversion and chronic lateral foot pain.
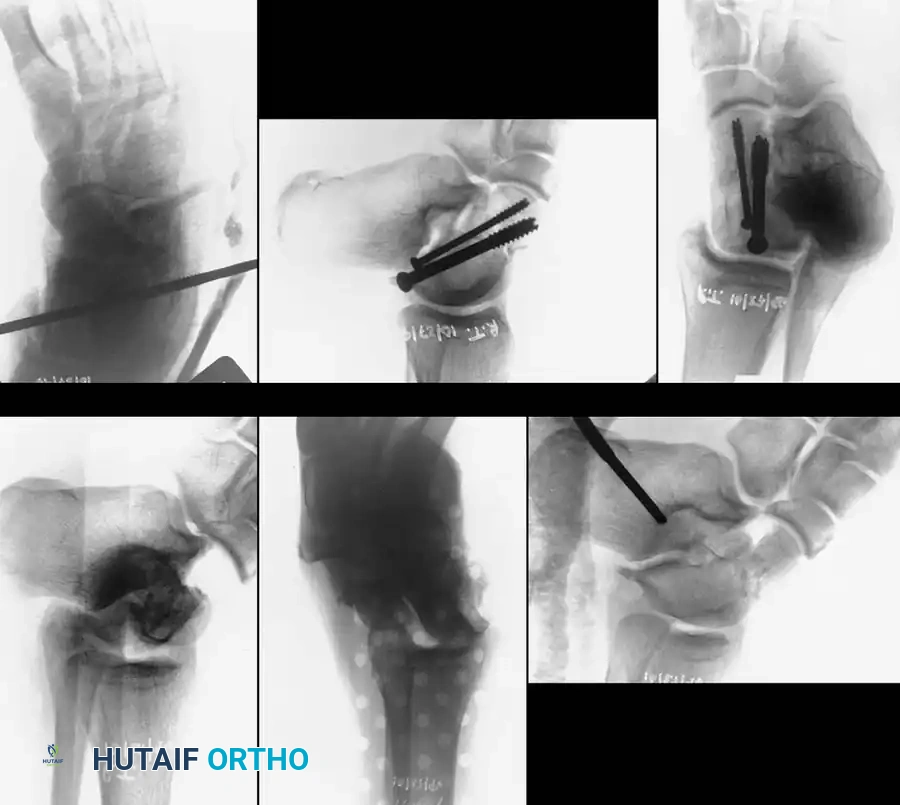
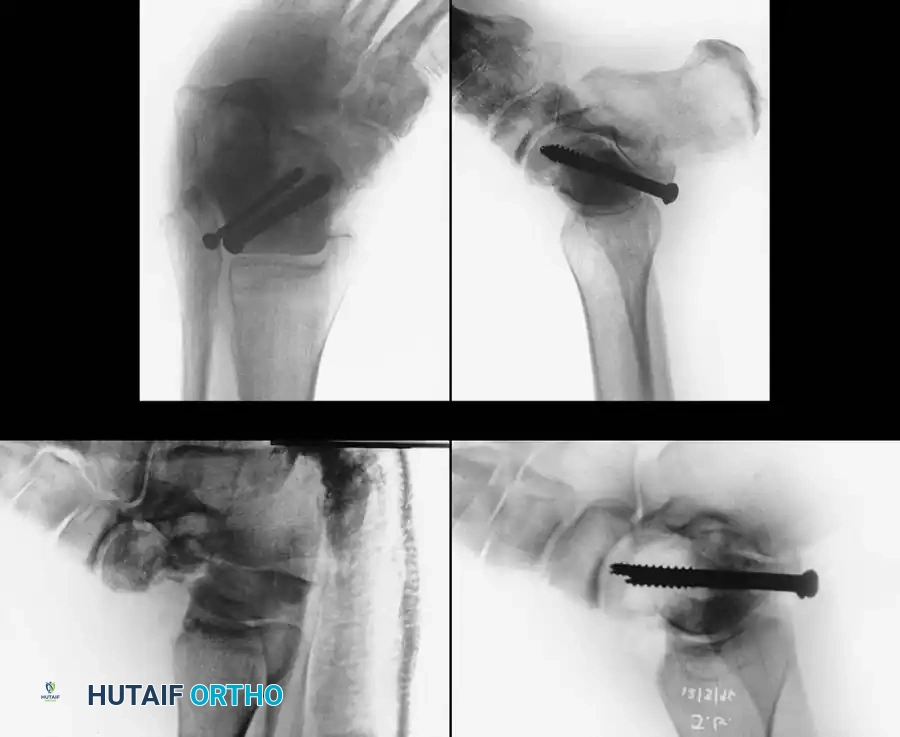
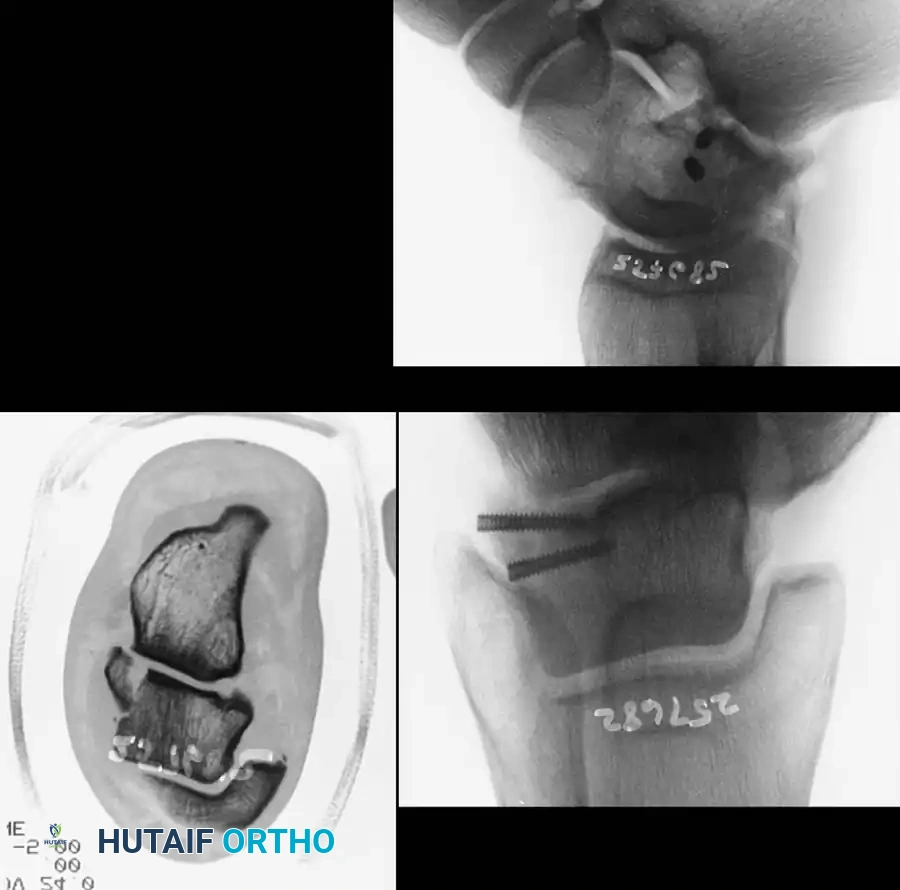
Reduction and Fixation:
Once anatomically reduced, provisional fixation is achieved with K-wires. Definitive fixation typically involves multiple lag screws (3.5 mm or 4.0 mm) placed from anterior to posterior, or posterior to anterior.

Posterior-to-anterior screw placement (via a posterolateral approach) is biomechanically superior as it engages the denser bone of the talar head, but it requires careful avoidance of the flexor hallucis longus (FHL) and the neurovascular bundle.

In cases of severe medial comminution, a mini-fragment plate (e.g., 2.0 mm or 2.4 mm) may be applied to the medial talar neck to act as a buttress and maintain length, preventing varus collapse.

Postoperative Protocol and Complications
Postoperatively, the limb is placed in a bulky Jones splint. Once incisions heal, early active range of motion of the ankle and subtalar joints is encouraged to nourish the articular cartilage. Strict non-weight-bearing is maintained for 10 to 12 weeks, guided by radiographic evidence of union.
Avascular Necrosis (AVN) and the Hawkins Sign
The most feared complication of talar neck fractures is AVN of the talar body. At 6 to 8 weeks post-injury, an AP or mortise radiograph of the ankle should be scrutinized for the Hawkins Sign.
The Hawkins sign is a subchondral radiolucent band visible in the dome of the talus. This radiolucency represents subchondral osteopenia secondary to hyperemic bone resorption. The presence of a Hawkins sign is a highly reliable indicator that the talar body retains its vascular supply. Conversely, a sclerotic, radiodense talar dome at 8 weeks indicates AVN.
If AVN develops but the talar dome has not collapsed, prolonged protected weight-bearing (often using a patellar tendon-bearing orthosis) may be utilized until creeping substitution occurs, which can take up to 24 months. If subchondral collapse and severe arthrosis occur, a tibiotalocalcaneal (TTC) arthrodesis or Blair fusion (tibiotalar fusion with a sliding anterior tibial graft) is required as a salvage procedure.
Post-Traumatic Arthritis
Even with anatomical reduction and stable internal fixation, post-traumatic arthritis of the subtalar joint is exceedingly common, reported in up to 50% of displaced fractures. This is due to the initial chondral injury sustained at the moment of impact. Patients must be counseled preoperatively that secondary reconstructive surgeries, such as subtalar or triple arthrodesis, may be necessary in the years following the initial trauma.
