INTRODUCTION AND EMBRYOLOGY
The human knee joint develops from a single mesenchymal cleft during early embryogenesis. During fetal development, the knee is initially separated into three distinct compartments (the suprapatellar pouch and the medial and lateral tibiofemoral compartments) by thin, vascularized synovial membranes. At approximately 4 to 5 months of fetal development, these synovial partitions undergo a process of progressive cavitation and resorption to form a single, unified joint cavity.
When this physiological resorption is incomplete or partial, it results in the persistence of incomplete synovial shelves, clinically referred to as synovial plicae. While the vast majority of these embryological remnants remain asymptomatic throughout an individual's life, they possess the potential to undergo pathological changes secondary to trauma, altered joint kinematics, or chronic inflammation, ultimately leading to symptomatic internal derangement of the knee.
ANATOMICAL CLASSIFICATION OF SYNOVIAL PLICAE
Synovial plicae of the knee are anatomically categorized based on their location relative to the patella and the tibiofemoral joint. They are commonly described in four distinct variations: suprapatellar, mediopatellar, infrapatellar, and lateral.
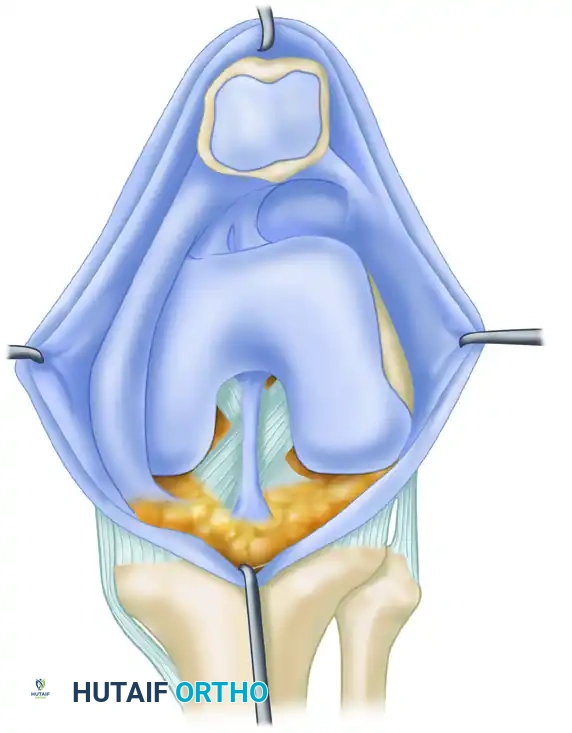
Infrapatellar Plica (Ligamentum Mucosum)
The infrapatellar plica is universally reported as the most common synovial plica in the human knee. It originates from the intercondylar notch of the femur, broadens as it descends anteriorly, and inserts into the synovial lining of the infrapatellar fat pad. Because of its central location, it is rarely implicated in impingement syndromes but can occasionally obscure arthroscopic visualization of the anterior cruciate ligament (ACL).
Suprapatellar Plica (Plica Synovialis Suprapatellaris)
Present in approximately 17% of individuals, the suprapatellar plica divides the suprapatellar pouch from the main tibiofemoral joint cavity. It can range from a small crescent-shaped fold to a complete septum with a central opening (the porta). While usually asymptomatic, a complete or near-complete suprapatellar plica can complicate arthroscopic entry into the suprapatellar pouch and may occasionally cause localized fluid loculation.
Medial Patellar Plica (Plica Synovialis Patellaris)
The medial patellar plica is the most clinically significant variant, reported in 5% to 70% of individuals. It originates from the medial wall of the joint capsule, runs obliquely downward across the medial aspect of the patella, and inserts into the synovial covering of the infrapatellar fat pad. It is this specific plica that is most frequently responsible for "plica syndrome" due to its anatomical propensity to bowstring across the medial femoral condyle during knee flexion.
Lateral Patellar Plica
The lateral plica is an exceedingly rare anatomical variant. When present, it is located along the lateral parapatellar gutter. It is almost universally asymptomatic and is typically noted only as an incidental finding during diagnostic arthroscopy.
PATHOPHYSIOLOGY AND BIOMECHANICS
A normal synovial plica is a thin, highly vascular, and pliable structure that glides seamlessly over the underlying articular cartilage during knee range of motion. However, any condition that produces chronic irritation, direct trauma, or intra-articular scarring may result in the pathological transformation of the plica.
Clinical Pearl: Poorly placed medial arthrotomy incisions or improperly localized anteromedial arthroscopy portals can damage a previously asymptomatic medial plica sufficiently to cause iatrogenic scarring, fibrosis, and subsequent symptomatic plica syndrome.
Mechanisms of Injury
- Direct Trauma: Bumping the flexed knee on a hard object (e.g., a dashboard injury during a motor vehicle collision) may directly traumatize the medial plica, inciting an acute inflammatory response.
- Repetitive Microtrauma: Activities requiring repetitive knee flexion and extension (such as cycling, running, or rowing) can subject the plica to continuous friction against the medial femoral condyle.
- Intra-articular Pathology: Concurrent conditions such as meniscal tears, osteochondritis dissecans, or chronic synovitis can alter joint kinematics and synovial fluid composition, leading to secondary plica inflammation.
Histological and Biomechanical Changes
When inflamed, the plica undergoes edema and thickening. If the inflammatory stimulus persists, the highly cellular synovial tissue undergoes fibrocartilaginous metaplasia. The plica becomes fibrotic, hyalinized, and profoundly inelastic.
Biomechanically, an inelastic medial plica acts as a rigid bowstring. As the knee flexes past 30 degrees, the thickened plica snaps forcefully across the medial femoral condyle. Several authors have noted a strong association between the presence of a pathological medial plica and the development of localized chondral lesions on the medial femoral condyle. These degenerative changes are directly caused by the mechanical impingement and shear forces generated by the snapping plica during repetitive knee motion.
CLINICAL EVALUATION
Diagnosing a symptomatic synovial plica requires a high index of suspicion and a meticulous clinical examination, as the symptoms frequently mimic other forms of internal derangement, most notably medial meniscus tears or patellofemoral pain syndrome.
History and Symptomatology
Patients typically present with insidious onset of anteromedial knee pain. Careful history-taking should differentiate the symptoms of a thickened, inelastic plica from those of a torn meniscus:
* Meniscal Pathology: Usually causes periodic episodes of true giving way, buckling, true locking (inability to fully extend), and pain strictly localized along the joint line. Pain is often increased or reproduced by torsion of the tibia on the femur (e.g., a positive McMurray test).
* Plica Syndrome: Produces popping, catching, and pseudo-locking in the knee caused by the plica snapping across the patella or medial femoral condyle. Pain is typically located superior to the joint line, along the medial parapatellar border.
Physical Examination
The hallmark of a pathological medial plica is a palpable, tender cord along the medial aspect of the patella.
The Stutter Test:
1. Position the patient seated on the edge of the examining table with the leg dangling freely.
2. Place your fingers lightly over the medial parapatellar region.
3. Instruct the patient to actively flex and extend the knee.
4. As the knee moves between 30 and 60 degrees of flexion, the abnormal plica flips over the medial femoral condyle. This often localizes the exact point of pain and may produce a palpable, momentary "stuttering" or snapping of the patella.
IMAGING MODALITIES
While the diagnosis of plica syndrome is primarily clinical, imaging can assist in ruling out concomitant pathology and confirming the presence of a thickened synovial shelf.
- Radiographs: Standard weight-bearing anteroposterior, lateral, and Merchant (skyline) views are typically normal but are essential to rule out osteoarthritis, loose bodies, or patellofemoral malalignment.
- Magnetic Resonance Imaging (MRI): MRI can visualize thickened plicae, particularly on T2-weighted axial and sagittal sequences, appearing as low-signal-intensity bands within the high-signal joint fluid. MRI is also invaluable for assessing the underlying articular cartilage for impingement lesions.
- Dynamic Ultrasonography: Dynamic ultrasound has emerged as a useful adjunct. It has been reported to have a diagnostic accuracy of 88%, a sensitivity of 90%, and a specificity of 83% in the evaluation of medial plica syndrome. The real-time nature of ultrasound allows the clinician to visualize the plica snapping over the condyle during active motion. However, it must be noted that this technique is highly operator-dependent.
ARTHROSCOPIC DIAGNOSIS
Despite advances in non-invasive imaging, an abnormal plica is diagnosed best by direct arthroscopic examination of the knee. Arthroscopy serves as both the definitive diagnostic gold standard and the primary therapeutic intervention.

During diagnostic arthroscopy, careful assessment of the width, thickness, and texture of the plica by viewing and tactile probing is paramount. A normal plica will feel soft and yield easily to the probe. A pathological plica will feel rigid, fibrotic, and unyielding.
Surgical Warning: When a suprapatellar or medial plica is sufficiently prominent, it can present significant difficulties during the initial stages of arthroscopy. The plica may act as a physical barrier as the arthroscope is introduced into the suprapatellar pouch, potentially leading to iatrogenic scuffing of the trochlear cartilage if forced.
Furthermore, the surgeon must dynamically evaluate the plica. By viewing from the anterolateral portal and slowly flexing and extending the knee, the surgeon can directly observe the medial plica impinging upon and abrading the medial femoral condyle, confirming its pathological nature.
CONSERVATIVE MANAGEMENT
Treatment of plica syndrome should initially be strictly conservative. Because the primary driver of symptoms is inflammation and edema, non-operative modalities are highly effective in the early stages of the disease before irreversible hyalinization occurs.
- Activity Modification: Restriction of offending activities (e.g., deep squatting, stair climbing, cycling) to reduce repetitive friction.
- Pharmacotherapy: A short course of oral nonsteroidal anti-inflammatory drugs (NSAIDs) to reduce synovial inflammation.
- Intra-articular Injections: Corticosteroid injections into the intra-articular space can provide profound relief by directly targeting the localized synovitis.
- Physical Therapy: Institution of a targeted, isometric exercise program for the quadriceps muscles. Strengthening the vastus medialis obliquus (VMO) alters patellar tracking, often pulling the medial plica anteriorly and reducing its impingement against the medial femoral condyle.
These conservative measures often result in a sufficient reduction of edema and synovitis so that the plica assumes a more normal resiliency and ceases to produce symptoms.
SURGICAL MANAGEMENT: ARTHROSCOPIC EXCISION
If a plica has become chronically fibrotic and hyalinized, and a minimum of 3 to 6 months of conservative measures fail to relieve the patient’s symptoms, surgical excision is indicated and should be curative.
While a limited excision can technically be performed through a small medial parapatellar arthrotomy incision, modern orthopedic standards dictate that excision is almost exclusively performed via arthroscopic techniques to minimize morbidity and accelerate rehabilitation.
Surgical Pitfall: Simply incising or sectioning the plica (a "plica release") is strongly discouraged. Because the knee joint is a highly cellular synovial environment, the continuity of a merely sectioned plica will rapidly be restored by dense scar tissue, leading to recurrent and often more recalcitrant symptoms. Complete resection is mandatory.
Patient Positioning and Setup
- The patient is placed in the supine position on the operating table.
- A well-padded tourniquet is applied to the proximal thigh (inflation is optional and based on surgeon preference, though it aids in visualization during synovectomy).
- The operative leg is placed in a lateral post or a dedicated leg holder to allow for valgus stress and full range of motion during the procedure.
Portal Placement
Standard anterolateral (AL) and anteromedial (AM) portals are utilized.
* The AL portal is established first for the arthroscope.
* The AM portal is established under direct intra-articular visualization using a spinal needle to ensure the trajectory allows parallel access to the medial plica without damaging the anterior horn of the medial meniscus or the articular cartilage.
Step-by-Step Surgical Technique
- Diagnostic Sweep: Perform a comprehensive diagnostic arthroscopy to rule out concomitant pathology (meniscal tears, loose bodies, ACL/PCL integrity).
- Dynamic Assessment: With the arthroscope in the AL portal, visualize the medial compartment while taking the knee through a full range of motion. Confirm the mechanical impingement of the medial plica against the medial femoral condyle.
- Resection: Introduce a motorized oscillating shaver (typically 4.0 mm or 4.5 mm) or an arthroscopic biting punch through the AM portal.
- Complete Excision: Begin resecting the plica at its free edge. Systematically resect the fibrotic tissue back to its origin on the medial capsular wall. Ensure that the entire shelf is removed from its superior origin near the suprapatellar pouch down to its insertion at the infrapatellar fat pad.
- Hemostasis: Because the base of the plica is highly vascular, use a radiofrequency (RF) ablation wand to achieve meticulous hemostasis along the resected capsular margin. This step is critical to prevent postoperative hemarthrosis.
- Final Inspection: Re-evaluate the knee through a full range of motion to ensure no residual plica tissue impinges on the condyle. Flush the joint copiously with saline to remove all synovial debris.
POSTOPERATIVE REHABILITATION PROTOCOL
The postoperative rehabilitation following arthroscopic plica excision is generally rapid, but it must be carefully structured to prevent intra-articular adhesions and recurrent scarring at the resection site.
Phase I: Immediate Postoperative (Days 1-7)
- Weight Bearing: Weight-bearing as tolerated (WBAT) with crutches. Crutches can typically be weaned within the first 3 to 5 days as quadriceps control returns.
- Range of Motion (ROM): Immediate emphasis on restoring full extension and progressive flexion. Early ROM is critical to prevent the medial capsule from scarring down to the medial femoral condyle.
- Exercises: Quadriceps sets, straight leg raises (SLR), ankle pumps, and patellar mobilizations.
- Cryotherapy: Aggressive icing to control effusion and hemarthrosis.
Phase II: Intermediate (Weeks 2-4)
- ROM: Achieve full, symmetrical ROM.
- Strengthening: Initiate closed kinetic chain exercises (e.g., mini-squats, leg presses) keeping flexion angles within a pain-free range. Emphasize VMO strengthening.
- Proprioception: Begin balance board and single-leg stance exercises.
Phase III: Return to Activity (Weeks 4-6)
- Advanced Strengthening: Progress to dynamic and functional strengthening.
- Cardiovascular: Stationary cycling and swimming.
- Clearance: Patients are typically cleared to return to full, unrestricted athletic activities by 4 to 6 weeks postoperatively, provided they have full ROM, no effusion, and symmetrical quadriceps strength.
COMPLICATIONS
While arthroscopic excision of a synovial plica is generally considered a safe and highly successful procedure, potential complications include:
* Postoperative Hemarthrosis: The most common complication, resulting from inadequate hemostasis of the vascular capsular base during resection.
* Recurrence of Symptoms: Usually due to incomplete resection of the plica, allowing scar tissue to bridge the defect and recreate the bowstring effect.
* Iatrogenic Cartilage Damage: Scuffing of the medial femoral condyle or trochlea by arthroscopic instruments during the resection process.
* Infection: Rare, but carries the standard risks associated with any arthroscopic intervention.
By adhering to strict diagnostic criteria, ensuring complete surgical resection rather than simple sectioning, and implementing early postoperative mobilization, orthopedic surgeons can achieve excellent, long-lasting clinical outcomes in the management of synovial plicae syndrome.
