INTRODUCTION AND PATHOANATOMY
A syndesmotic injury represents a critical disruption of the distal tibiofibular articulation, a complex ligamentous structure essential for the stability and congruity of the ankle mortise. The syndesmotic complex comprises the anterior inferior tibiofibular ligament (AITFL), the posterior inferior tibiofibular ligament (PITFL), the interosseous membrane (IOM), and the transverse ligament.
These injuries are most commonly precipitated by specific biomechanical forces, predominantly pronation–external rotation (PER) and pronation-abduction (PA) mechanisms, and infrequently by supination–external rotation (SER) mechanisms. In the Danis-Weber classification, these correspond primarily to Type C and Type B injuries. During these traumatic events, the talus is forced to abduct or rotate externally within the mortise, acting as a wedge that forcefully separates the distal fibula from the tibia, leading to sequential disruption of the syndesmotic ligaments.
Clinical Pearl: Anatomical restoration of the distal tibiofibular syndesmosis is non-negotiable. Even a 1-mm lateral shift of the talus reduces the tibiotalar contact area by 42%, exponentially increasing joint contact stresses and the risk of rapid-onset post-traumatic osteoarthritis.
INDICATIONS FOR OPERATIVE INTERVENTION
Historically, closed reduction and casting were attempted for various ankle fractures; however, contemporary orthopedic consensus strongly favors operative intervention. Nonunion has been reported in approximately 10% of bimalleolar fractures treated by closed methods. Furthermore, 20% of bimalleolar fractures involve intraarticular osteochondral injuries to the talus and tibia—pathologies that remain entirely unaddressed when nonoperative methods are employed.
Randomized, prospective, and long-term follow-up studies of bimalleolar or bimalleolar-equivalent ankle fractures have unequivocally demonstrated the superior results of operative over nonoperative treatment. A landmark long-term follow-up study by Bauer et al. confirmed superior functional outcomes following the operative treatment of supination–external rotation stage IV fractures. Consequently, the AO Foundation and leading orthopedic trauma groups recommend Open Reduction and Internal Fixation (ORIF) of both malleoli for virtually all displaced bimalleolar fractures.
SURGICAL APPROACHES TO THE LATERAL MALLEOLUS
For the vast majority of displaced bimalleolar and syndesmotic injuries, ORIF of the lateral malleolus is the critical first step in restoring the lateral buttress of the ankle mortise. Most Weber Type B and Type C lateral malleolar fractures are stabilized utilizing standard plate and screw osteosynthesis.
Standard Lateral Plating vs. Posterior Antiglide Plating
While lateral plating is the traditional workhorse, hardware prominence can become symptomatic, particularly in patients with minimal subcutaneous tissue. Studies indicate that while hardware removal is common, only about 50% of patients experience complete pain relief post-removal.
To mitigate these issues and enhance biomechanical stability, posterior plating of Weber Type B fractures using an antiglide technique is highly advocated.
Advantages of Posterior Antiglide Plating:
* Biomechanical Superiority: Converts axial loading forces into compression at the fracture site.
* Avoidance of Joint Penetration: Eliminates the risk of placing intraarticular screws into the distal tibiofibular joint.
* Decreased Hardware Prominence: The plate is buried deep to the peroneal tendons, reducing palpable hardware.
In a prospective series of 32 patients treated with posterior antiglide plating, there were zero nonunions, malunions, wound complications, or losses of fixation. However, surgeons must be acutely aware of potential complications. Weber et al. documented peroneal tendon lesions precipitated by posterior antiglide plating. In their series, 30% of patients demonstrated peroneal tendon injury at the time of hardware removal.
Surgical Warning: Peroneal tendon lesions correlate strongly with distal plate placement and screw insertion through the most distal hole of the plate. To prevent peroneal tendinitis, avoid placing hardware too distally on the posterior fibula, and refrain from early hardware removal unless strictly necessary.
Lag Screw Only and Alternative Fixation Techniques
In specific fracture patterns, hardware prominence can be entirely circumvented by utilizing a lag screw-only technique. Several authors have reported highly successful treatment of long oblique lateral malleolar fractures using multiple lag screws without a neutralization plate.
Below are various established methods for fixing the lateral malleolus prior to addressing the syndesmosis:
A, Standard fixation of a fibular fracture utilizing a one-third semitubular 3.5-mm plate and screws in a neutralization mode.
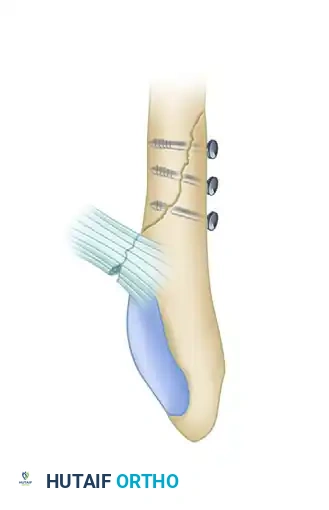
B, Fixation achieved using multiple 3.5-mm interfragmentary lag screws, ideal for long oblique patterns where plate prominence is a concern.
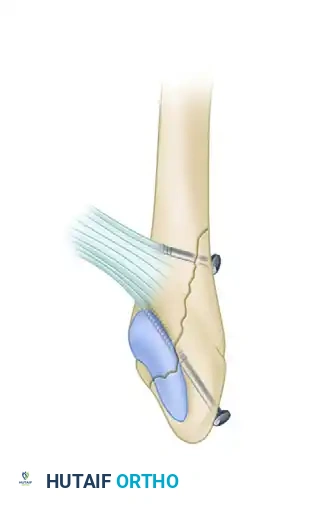
C, Two lag screws utilized for a long oblique fracture, providing absolute stability through interfragmentary compression.
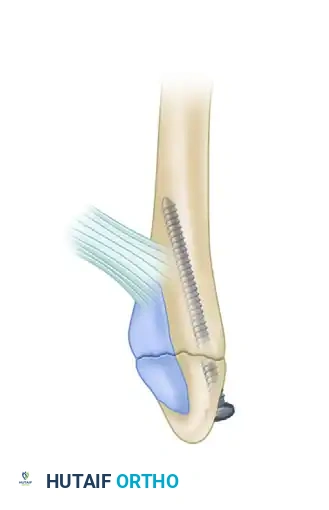
D, A single 3.5-mm malleolar screw utilized for a low transverse avulsion-type fracture.
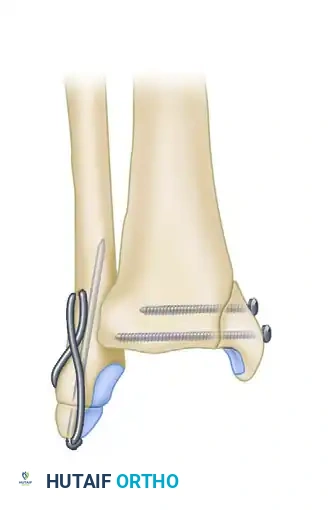
E, Tension band wiring technique for the lateral malleolus; note the concurrent 4-mm lag screw fixation of the associated medial malleolar fracture.
F, Minimally invasive fixation utilizing a 3.5-mm intramedullary screw.
INTRAOPERATIVE ASSESSMENT OF THE SYNDESMOSIS
Once the lateral and medial malleoli are stabilized, the integrity of the syndesmosis must be rigorously evaluated. If a fibular fracture occurs above the level of the distal tibiofibular joint (Weber C), the syndesmosis is assumed to be disrupted.
The Cotton Test and External Rotation Stress Test
The integrity of the syndesmosis is evaluated intraoperatively using the External Rotation Stress Test and the Cotton Test.
- The Cotton Test: Described by Cotton to determine intraoperative incompetence of the syndesmosis. A bone hook or reduction forceps is applied to the fibula, and lateral distraction force is applied to separate it from the tibia (while an opposing force stabilizes the tibia).
- Radiographic Parameters: If more than 3 to 4 mm of lateral displacement occurs, syndesmotic fixation is mandatory. Intraoperative mortise radiographs should demonstrate a tibiofibular clear space of less than 5 mm between the medial wall of the fibula and the lateral wall of the posterior tibial malleolus. Persistent widening indicates an unreduced or unstable syndesmosis.
Clinical Pearl: Stark et al. identified a 39% incidence of syndesmotic instability after lateral malleolar fixation in Weber B fractures. Therefore, intraoperative external rotation stress evaluation is mandatory for all unstable ankle fractures, not just Weber C patterns. Furthermore, Xenos et al. demonstrated that posterior displacement of the fibula on a lateral stress radiograph correlates more closely with anatomical diastasis than displacement on standard mortise views.
SYNDESMOTIC REDUCTION AND FIXATION TECHNIQUES
Direct Visualization and Reduction
The syndesmosis must be anatomically reduced and provisionally held with Kirschner wires or a large reduction clamp before definitive screws are inserted. Blind reduction using only fluoroscopy is fraught with error. Miller et al. noted a significant decrease in syndesmotic malreductions in cohorts where the syndesmosis was directly visualized. We strongly advocate for open reduction of the syndesmosis with direct visualization of the anterior incisura.
Screw Trajectory and Placement
Various methods exist to fix the syndesmosis, most commonly utilizing cortical screws. These screws hold the joint anatomically reduced while stabilizing the lateral buttress of the ankle mortise.
- Positioning: The screw should be positioned 2 to 3 cm proximal to the tibial plafond.
- Trajectory: It must be directed parallel to the joint surface and angled 30 degrees anteriorly to ensure it is perpendicular to the tibiofibular joint axis.
- Pitfalls of Malpositioning:
- Placed too proximally: May deform the fibula and cause the mortise to widen.
- Not parallel to the joint: The fibula may shift proximally.
- Not perpendicular (lacking the 30-degree anterior angle): The fibula may remain laterally displaced or subluxated posteriorly.
Implant Selection: Size, Number, and Cortices
- Screw Size: Either 3.5-mm or 4.5-mm cortical screws are acceptable; biomechanical studies show equivalent efficacy. A survey by Bava et al. noted that 51% of surgeons prefer 3.5-mm screws, while 24% use 4.5-mm screws.
- Number of Screws: Two screws provide a more secure construct than one. Vander Griend, Michelson, and Bone highly recommend using two syndesmotic screws in large, heavy, or noncompliant patients.
- Cortical Engagement: The screw should pass through both cortices of the fibula and either one (tricortical) or two (quadricortical) cortices of the tibia. Engaging four cortices is the most common construct (used by 44% of surveyed surgeons).
The Dorsiflexion Controversy
Traditionally, it was taught that the ankle must be maximally dorsiflexed during syndesmotic screw insertion to accommodate the wider anterior dome of the talus and prevent postoperative stiffness. Current evidence refutes this. Maximal dorsiflexion may induce an external rotation moment, risking malreduction of the fibula out of the incisura. Cadaveric studies have found no loss of dorsiflexion when the syndesmosis is fixed with the ankle in neutral or slight plantar flexion.
Integration with Fibular Plating
If a plate has been used to fix the fibular fracture, the syndesmotic transfixing screw can seamlessly be integrated through one of the plate's holes.
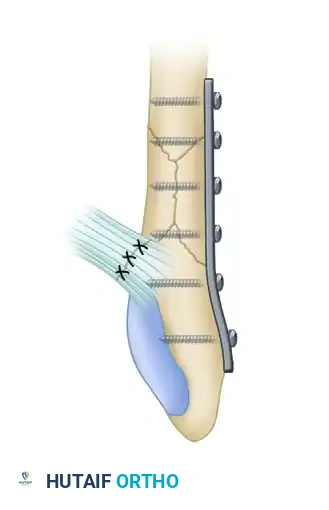
FIGURE 54-4: Fracture of the fibula above the level of the syndesmosis with disruption of the distal tibiofibular syndesmosis and rupture of the deltoid ligament. The deltoid was repaired, a small fragment plate was applied to the fibula, and the syndesmosis was repositioned and held by a transfixing screw through the distal hole of the fibular plate.

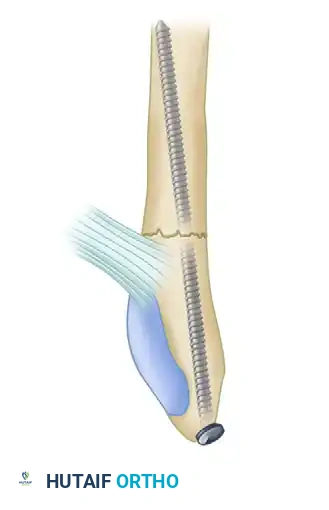
FIGURE 54-5: Bimalleolar ankle fracture featuring an oblique fracture of the lower fibula treated with interfragmentary screw fixation. Kirschner wires were utilized for the internal fixation of the medial malleolus.
TO FIX OR NOT TO FIX: PROXIMAL EXTENSION RULES
In the past, internal fixation of all syndesmotic injuries was considered mandatory. However, landmark cadaveric studies by Boden et al. revolutionized this approach. They demonstrated that disruption of the syndesmosis does not cause ankle instability if the medial structures (deltoid ligament or medial malleolus) are intact or rigidly repaired.
The Boden Criteria:
* If a medial lesion is present and repaired, syndesmotic injuries extending less than 3 cm proximal to the ankle joint do not alter joint mechanics and do not require fixation.
* Syndesmotic injuries extending more than 4.5 cm proximal to the joint significantly alter mechanics and demand fixation.
* Disruptions between 3.0 and 4.5 cm produce variable results and require intraoperative judgment.
Kennedy et al. further evaluated Weber Type C fractures where the fibular fracture was within 5 cm of the joint. They found that if the fracture was anatomically reduced and immobilized for 6 weeks, syndesmotic screw fixation was unnecessary.
Current Consensus Indications for Syndesmotic Fixation:
1. Syndesmotic injuries associated with proximal fibular fractures (Maisonneuve) where fibular plating is not planned, combined with a medial injury.
2. Syndesmotic injuries extending more than 5 cm proximal to the plafond.
3. Any demonstrated intraoperative instability (via Cotton test) after medial and lateral fixation.
CONTROVERSIES: HARDWARE REMOVAL
Whether and when syndesmotic screws need to be removed remains one of the most debated topics in orthopedic trauma.
- The Argument for Removal: Advocates contend that rigid syndesmotic fixation disrupts normal ankle kinematics by restricting the physiologic external rotation and proximal migration of the fibula that occurs during dorsiflexion. Routine removal is often suggested before weight-bearing (at 6 to 8 weeks).
- The Argument Against Removal: Removing the screw too early risks recurrent diastasis. Late diastasis is a catastrophic clinical problem, far more difficult to manage than a broken screw. If tricortical fixation is used, the screw typically loosens rather than breaks, allowing physiologic motion without catastrophic failure. If quadricortical fixation is used and the screw breaks, the retained fragments rarely cause symptoms.
Evidence-Based Recommendation:
Recent studies reveal that at 1-year follow-up, there is no difference in clinical outcomes between patients with intact versus removed syndesmotic screws. Surprisingly, subsets of patients with broken screws often demonstrate improved clinical outcomes, likely due to the restoration of physiologic micro-motion.
Surgical Protocol: We have transitioned toward not routinely removing syndesmotic fixation, unless the hardware becomes specifically symptomatic. If removal is elected, it is strictly advised to leave the screw in place for a minimum of 12 weeks to ensure adequate ligamentous healing.
POSTOPERATIVE PROTOCOL AND OUTCOMES
Postoperative management requires a delicate balance between protecting the syndesmotic reduction and preventing joint stiffness.
* 0-2 Weeks: The patient is placed in a well-padded short leg splint, strictly non-weight-bearing.
* 2-6 Weeks: Transition to a CAM boot. Range of motion exercises are initiated, but weight-bearing is generally restricted, especially if rigid quadricortical screws are utilized.
* 6-12 Weeks: Progressive weight-bearing is allowed. If suture-button (flexible) fixation was used, earlier weight-bearing may be permitted based on surgeon preference.
Prognosis:
It is vital to counsel patients regarding long-term expectations. Egol et al. evaluated outcomes after unstable ankle fractures and determined that at 1-year follow-up, patients who required syndesmotic fixation had poorer functional outcomes compared to those who had malleolar fracture fixation alone. This discrepancy is not necessarily a failure of the fixation technique, but rather a reflection of the higher energy and greater severity of the initial soft-tissue and chondral injury inherent to syndesmotic disruptions.
Postoperative radiographic measurements (plain films) are notoriously unreliable markers of syndesmotic reduction. If malreduction is suspected postoperatively, Computed Tomography (CT) is the gold standard for assessing the congruity of the distal tibiofibular articulation and should be utilized liberally.
