DEFINITION
Septic arthritis is defined as an infection within the closed space of a joint. It is usually acute and purulent secondary to a bacterial infection.It can cause irreversible damage to articular cartilage and therefore warrants prompt treatment with adequate drainage and an appropriate antibiotic regimen.Delay in making the diagnosis and initiating treatment can have serious negative implications to the condition of the joint and health of the patient.2
ANATOMY

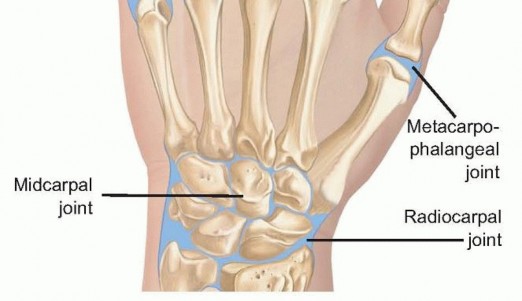
FIG 1 • Anatomy of the IP, MP, and wrist joints.
PATHOGENESIS
Septic arthritis may affect any joint of the hand or wrist.Septic arthritis does not have a gender or race predilection, but it is more common in adults than in children. The inoculation of the joint is most likely due to a penetrating injury (ie, lacerations, puncture wounds, and bites). Other causes include hematogenous seeding or contiguous spread.10At the distal IP joint, septic arthritis is common from penetrating trauma as well as contiguous infection from a mucous cyst, felon, paronychia, or suppurative flexor tenosynovitis.At the proximal IP joint, contiguous infection is most commonly related to a suppurative flexor tenosynovitis. At the MP joint, septic arthritis is most common after direct inoculation from a clenched fist injury or fight bite.Hematogenous spread can result from any concomitant or preceding infection of the body, including oral, upper respiratory, gastrointestinal, and genitourinary infections.The synovium is highly vascular and contains no limiting basement membrane, promoting easy access of blood contents to the synovial space.3The presence of bacteria within the joint induces a cellular and immunologic response that is detrimental to the joint. Bacteria rapidly replicate, producing toxins. The presence of bacteria stimulates an immunogenic response, resulting in the arrival of leukocytes, which produce proteolytic enzymes. Both the bacterial toxins and leukocytic enzymes destroy the articular cartilage of the joint by degrading proteoglycans and eventually injuring the underlying chondrocytes.Multiple risk factors can predispose a patient to septic arthritis6 (Table 1).Any disorder that results in an immunocompromised state can predispose to septic arthritis.Local factors|Systemic disorders---|---Penetrating joint trauma Recent joint surgeryOpen reduction of intra-articular fractures OsteoarthritisProsthetic jointsSocial factors Newborns ElderlyOccupational exposure to animalsLow socioeconomic status|Rheumatoid arthritis Diabetes mellitusLiver diseases, alcoholism Chronic renal failure, hemodialysis MalignanciesAIDSImmunosuppressive medication IV drug abusers Table 1 Common Risk Factors Predisposing to Septic Arthritis IV, intravenous.P.1166 Table 2 Common Microorganisms Causing Septic Arthritis
GRAM-POSITIVE AEROBESSTAPHYLOCOCCUS AUREUS STREPTOCOCCUS PYOGENES
Streptococcus pneumoniae
GRAM-NEGATIVE AEROBESHAEMOPHILUS INFLUENZAE ESCHERICHIA COLI
P. multocidaN. gonorrhoeae
ANAEROBES
Eikenella corrodens Borrelia burgdorferi Mycobacterial species
FUNGUS
SporotrichosisCryptococcusBlastomycosisRheumatoid arthritis, in particular, poses a higher risk of infection. This risk is related to a variety of factors including general debilitation, immunosuppressive medication, tumor necrosis factor blockers (eg, infliximab or etanercept), and chronic joint injury.In patients with rheumatoid arthritis, a diagnosis of septic arthritis may be delayed because of misinterpretation of a rheumatoid flare. A high index of suspicion must be maintained when evaluating forseptic arthritis in patients with rheumatoid arthritis.9Virtually, any microbial pathogen is capable of causing pyogenic septic arthritis (Table 2).Staphylococcus aureus and Streptococcus species are the most common offending organisms.Gram-negative, anaerobic, and polymicrobial infections also are possible, especially in intravenous (IV) drug abusers and immunocompromised patients.Specific bacterial pathogens are related to certain circumstances, for example,Eikenella corrodensin human bite wounds,Pasteurella multocidaafter domestic animal bites,Neisseria gonorrhoeaeinfections in sexually active young patients, and fungal and mycobacterial infections in immunocompromised patients.
NATURAL HISTORY
The combination of the growing bacterial load and the ensuing inflammatory response results in a growing effusion that causes synovial ischemia, pressure necrosis of the cartilage, and infiltration of the bacteria into both the subchondral bone and overlying skin.Bacterial infiltration out of the joint can result in secondary osteomyelitis, suppurative flexor tenosynovitis, and skin breakdown with spontaneous drainage.
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients will complain of pain and swelling about the joint.Systemic signs of joint infection may include fevers, chills, malaise, and tachycardia.The patient should be asked about a history of penetrating trauma; human, animal, or insect bites; recent joint aspirations; recent infections elsewhere; and the presence of an immunocompromising condition.On examination, patients will manifest a painful swollen joint, with overlying erythema and warmth.The most important physical examination finding is exquisite pain with precise joint motion, different from that typically seen when a noninfectious effusion or overlying cellulitis is present.Use of a regional block for pain relief, often performed by an emergency or primary care physician, will mask the condition and must be discouraged.Attempted active digital motion will result in significant guarding, and passive flexion and extension should induce exquisite pain.Physical examination of the wrist often is less dramatic than that of the digits. The joint typically is held in a neutral position.Active wrist motion also will induce guarding and pain.Passive flexion will also cause the patient to guard secondary to pain.Passive pronation and supination may also help determine involvement of the distal radioulnar joint.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Laboratory studies should include white blood cell (WBC) count, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and blood cultures.The WBC usually is not elevated, but the ESR and CRP levels are consistently elevated (unless the patient is immunocompromised).Diagnosis of a septic arthritis is best accomplished by joint aspiration, microscopic analysis, and culture.If an infection is present, increased fluid turbidity will be noted.Joint aspirates should be sent for a cell count with differential, Gram stain, crystal analysis, glucose, and cultures (aerobic, anaerobic, fungal, and mycobacterial) (Table 3). Table 3 Differential Diagnosis of Synovial Fluid Analysis WBC, white blood cell; PMN, polymorphonuclear leukocyte.Diagnosis can be made most reliably with a joint fluid WBC count greater than 50,000 (and a differential of 75% or more segmented neutrophils), a Gram stain confirming the presence of bacteria, or positive cultures.5Test|Normal|Septic|Inflammatory------|---Clarity|Transparent|Opaque|Straw------|---Color|Clear|Yellow-green|YellowViscosity|High|Variable|HighWBC count|<200|

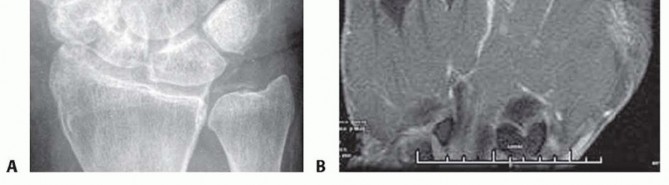
FIG 2 • A. Radiograph showing chondrocalcinosis of the triangular fibrocartilage complex from chronic pseudogout. B. Coronal T2-weighted MRI of an MP joint with underlying septic arthritis. Note the normal bone signal but the presence of high signal within the joint from the fluid and surrounding soft tissue inflammation. A low WBC count with a high percentage of neutrophils (>90%) may indicate an early septic arthritis.11 A joint glucose of 40 mg/dL or less compared with the fasting blood glucose level also suggests a septic process.7Crystal analysis is necessary to rule out the presence of gout or pseudogout because they also can present similarly, including an elevated WBC count in the aspirate.The role of imaging studies early in the course of the septic process is limited. Radiographs may reveal joint distention, presence of foreign bodies, osteomyelitis, air in the soft tissues, and chondrocalcinosis (characteristic of both gout and pseudogout) (FIG 2A). Later radiographs may reveal joint destruction.Magnetic resonance imaging (MRI) is effective in diagnosing early septic arthritis and in differentiating it from osteomyelitis or overlying tenosynovitis (FIG 2B).
DIFFERENTIAL DIAGNOSIS
Rheumatoid arthritisCrystalline arthropathies: gout, pseudogoutSeronegative arthropathies: systemic lupus erythematosus, psoriatic arthritis, Reiter syndrome, ankylosing spondylitis, rheumatic feverLyme disease Cellulitis OsteomyelitisSuppurative flexor tenosynovitis
NONOPERATIVE MANAGEMENT
Septic arthritis is predominantly a surgical problem warranting operative management.However, if septic arthritis is detected or suspected early enough, antibiotics alone have been suggested in the medical literature to be sufficient in the eradication of the infection.3In cases where comorbid conditions contraindicate surgery, serial aspiration of the involved joint can be done to decrease the bacterial load, decompress the joint, and allow medical management with antibiotics to treat the infection.However, this technique has been shown to be less effective than open surgical drainage in large joints and, therefore, would be even less reliable in small joints.4
SURGICAL MANAGEMENT
Septic arthritis typically warrants prompt surgical intervention to drain and lavage the joint.Open and arthroscopic techniques are available for surgical drainage of the wrist. Arthroscopic intervention is recommended to maximize drainage, visualization, lavage, and débridement while minimizing the surgical morbidity.
PREOPERATIVE PLANNING
Arrangements for instruments, irrigation fluid, drains, sutures, and assistants should be made in advance of surgery.
POSITIONING
Approaches to the hand and wrist can be accomplished with the patient supine and the operative extremity extended on a hand table with the surgeon and assistants seated.The hand table should be stable and well-secured and should allow adequate space for both the operative limb and the surgeon's elbow and forearm to minimize surgeon fatigue and enhance stability.Tourniquet use is advised to obtain a bloodless field and clear visualization of anatomic structures.The limb usually is exsanguinated via gravity with elevation before inflating the tourniquet to avoid proximal spread of the bacteria with the use of an Esmarch.A small joint wrist arthroscopy tower should be used. This will provide appropriate positioning and application of traction during arthroscopy and also facilitate conversion to an open procedure if necessary. Additionally, small joint arthroscopy equipment, including a 30-degree 2.7-mm camera, should be available for use.
APPROACH
Multiple approaches to a joint are available. The choice of which approach to use should be based on ease of the approach while still allowing adequate joint exposure for débridement and minimizing contiguous spread of infection.All surgical approaches of the hand and wrist warrant a sound understanding of surface anatomy, surgical anatomy, internervous planes, and surgical technique.P.1168
TECHNIQUE
Aspiration of Interphalangeal or Metacarpophalangeal Joints Surgical Drainage of Interphalangeal or Metacarpophalangeal Joints
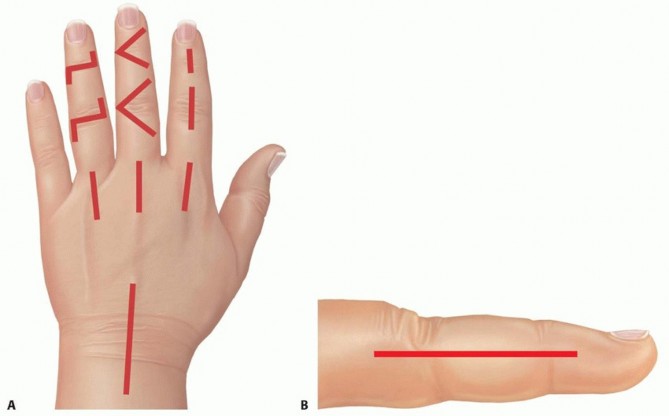
TECH FIG 1 • A. Sample incisions for open dorsal drainage of the IP, MP, and radiocarpal joints. B.
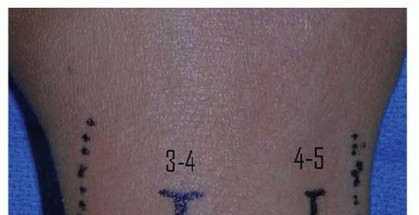
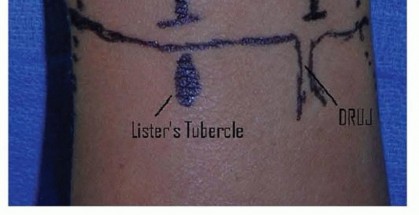

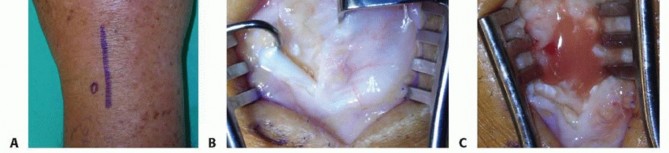
TECH FIG 3 • A. Incision for open drainage of the wrist. B. The distal third of the extensor retinaculum is released and the interval between the third and fourth dorsal compartment developed. C. The capsule is arthrotomized with an inverted T. The joint should be thoroughly irrigated with gravity cystoscopy tubing or a bulb syringe.Pulse lavage should be avoided due to its potential to cause additional soft tissue injury.The joint should be ranged during irrigation to maximize the effect of the lavage.The joint surfaces are inspected for articular damage.Leave a small wick or drain in the joint and loosely close the skin around the wick.Primary closure of the joint risks reaccumulation of the purulence. Typically, two to three loosely placed 4-0 nylon sutures will be sufficient.Place the wrist in a volar splint for comfort and encourage limb elevation.Diagnosis1. Diagnosis is best accomplished by joint aspiration and analysis.Antibiotics1. Obtain cultures before beginning antibiotics.2. Empiric antibiotics should be tailored to the most likely organism based on mechanism of injury and patient factors.Aspiration1. Avoid using larger syringes because the vacuum created can collapse the jointand may be less effective for aspiration.Arthroscopicdrainage1. Identify the surface landmarks of the joint and avoid inadvertent injury to thedorsal tendons and cutaneous nerve.2. Be prepared to convert to an open procedure if adequate exposure and débridement are not possible.Open surgicaldrainage1. Be prepared to perform a second open surgical débridement if symptoms do notimprove.
PEARLS AND PITFALLS
POSTOPERATIVE CARE
P.1171Empiric IV antibiotics are initiated immediately after obtaining cultures and then later tailored to the results of laboratory cultures and sensitivities.IV antibiotics should be continued for 2 weeks or at least through symptom resolution, followed by oral antibiotics.8The duration of antibiotics is the subject of some controversy. This should be determined on a case-by-case basis, with consideration of surgical findings, virulence of the offending bacterial pathogen, and the response to treatment.Early range of motion (active and active-assisted) in diluted povidone-iodine soaks is initiated three times daily to provide mechanical lavage of the joint and to prevent premature wound closure.The wick or drain is removed 1 or 2 days postoperatively.As symptoms resolve, the soaks are discontinued to allow the wound to heal and progressive range-of-motionexercises are initiated.If symptoms do not improve within 2 days, then a repeat surgical drainage should be considered.
OUTCOMES
The results of surgical treatment of septic arthritis are not well documented in the literature, and it is difficult to predict the outcome even during the course of treatment.Functional outcome is most closely correlated to the duration of symptoms before treatment is initiated.10 Some loss of motion and joint stiffness are expected, even in cases treated with early surgical drainage and rehabilitation.1,10,12,13,14Some joint space narrowing usually is seen following treatment, and significant arthrosis and ankylosis may occur in severe cases or when treatment has been delayed.
COMPLICATIONS
Joint stiffness, arthrosis, osteomyelitis, and secondary tendon adhesionsSalvage options for postseptic arthritis include arthrodesis, resection arthroplasty, or amputation. Implant arthroplasty is controversial and is not generally recommended for a previously infected joint.
REFERENCES
- Boustred AM, Singer M, Hudson DA, et al. Septic arthritis of the metacarpophalangeal and interphalangeal joints of the hand. Ann Plast Surg 1999;42:623-628.
- Glass KD. Factors related to the resolution of treated hand infections. J Hand Surg Am 1982;7:388-394.
- Goldenberg DL, Reed JI. Bacterial arthritis. N Engl J Med 1985; 312:764-771.
- Leslie BM, Harris JM III, Driscoll D. Septic arthritis of the shoulder in adults. J Bone Joint Surg Am 1989;71:1516-1522.
- Li SF, Cassidy C, Chang C, et al. Diagnostic utility of laboratory tests in septic arthritis. Emerg Med J 2007;24:75-77.
- Linscheid RL, Dobyns JH. Common and uncommon infections of the hand. Orthop Clin North Am 1975;6:1063-1104.
- Moran G, Talan D. Hand infections. Emerg Med Clin North Am 1993;11:601-619.
- Murray PM. Septic arthritis of the hand and wrist. Hand Clin 1998;14:579-587.
- O'Dell JR. Anticytokine therapy—a new era in the treatment of rheumatoid arthritis. N Engl J Med 1999;340:310-312.
- Rashkoff E, Burkhalter W, Mann R. Septic arthritis of the wrist. J Bone Joint Surg Am 1983;65:824-828.
- Shmerling RH, Delbanco TL, Tosteson AN, et al. Synovial fluid tests. What should be ordered? JAMA 1990;264:1009-1014.
- Sinha M, Jain S, Woods DA. Septic arthritis of the small joints of the hand. J Hand Surg Br 2006;31:665-672.
- Willems C. Treatment of purulent arthritis by wide arthrotomy followed by immediate active mobilization. Surg Gynecol Obstet 1919;28:546-554.
- Wittels N, Donley J, Burkhalter W. A functional treatment method for interphalangeal pyogenic arthritis. J Hand Surg Am 1984;9:894-898.
