DEFINITION
Nerve tumors make up less than 5% of tumors about the hand and wrist.13Most nerve tumors are benign and grow without causing neural dysfunction. As a result, the neural origin of a mass is often not anticipated and unexpected loss of function may occur after surgery.The key is to prepare for excision of any mass by discussing the possibility of a nerve tumor with the patient, by recognizing patients and masses with a high likelihood of a nerve tumor, and by being familiar with surgical techniques that allow preservation or, if necessary, reconstruction of the affected nerve.
ANATOMY
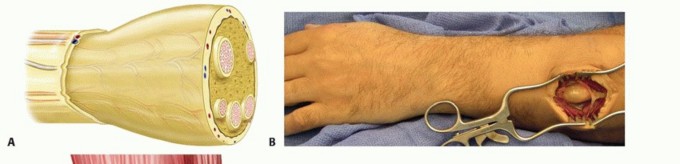
Peripheral nerves consist of axons surrounded by a nerve sheath (FIG 1).The epineurium is a thin outer layer of connective tissue containing blood vessels that supply the nerve. Perineural cells form a strong cellular layer, the perineurium, surrounding each fascicle (bundle) of axons. An endoneurial layer of protective Schwann cells surrounds each individual axon.
PATHOGENESIS
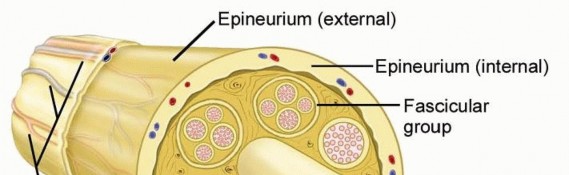
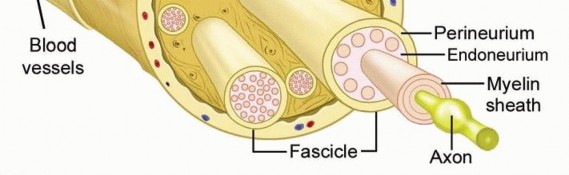
FIG 1 • Peripheral nerve anatomy. Individual axons travel together within a well-organized nerve sheath. The cells of the nerve sheath (not the axons) form the nerve tumor. Neurofibromas also arise from nonmyelinating Schwann cells but are found within the substance of the nerve and cannot be enucleated from the fascicles.11Other benign peripheral nerve sheath tumors (BPNSTs) include the granular cell tumor, neurothekeoma, nerve sheath myxoma, and perineurioma. Electron microscopy and immunohistochemistry may be necessaryto determine the type of tumor and cell of origin in some cases.3Malignant peripheral nerve sheath tumors (MPNSTs) arise de novo or from malignant change within a BPNST, usually a neurofibroma.About half of MPNSTs occur in patients with neurofibromatosis (NF) type I (von Recklinghausen disease).The incidence of a MPNST in patients with NF type I is 2%8 (compared to 0.001% in general population4), although the lifetime risk rises to 13%.2
NATURAL HISTORY
Upper extremity BPNSTs are usually solitary and occur most in middle-aged adults.5,7 Pediatric nerve tumors are uncommon.1BPNSTs are typically painless and slow-growing, with malignant degeneration being exceedingly rare. Mosttumors are relatively small (<2.5 cm), although they may cause nerve dysfunction due to focal impingement on the adjacent axons.Patients with NF type I often have multiple schwannomas, neurofibromas, or both of major upper extremity nerves. Thick tortuous “plexiform” neurofibromas are common in NF type I and have a high risk of progression to malignancy.
PATIENT HISTORY AND PHYSICAL FINDINGS


FIG 2 • A. Hypesthesia of the thenar eminence caused by an apparent tumor of the palmar cutaneous branch (PCB) of the median nerve. B. Careful dissection reveals a ganglion arising from the radioscaphoid articulation. C. The PCB is freed from the compressive mass. Giant cell tumors (GCTs) of the tendon sheath: reactive lesions of synovium that occur about the palm and fingers in similar locations to nerve tumors. GCTs are often palpably nodular compared to the smooth margins of a nerve tumor.Lipomas: These fatty tumors are usually more superficial and mobile than a nerve tumor. Rarely, lipomas grow in the carpal canal, causing median neuropathy.Epidermal inclusion cysts: should be suspected when examination reveals evidence of prior penetrating trauma. Unlike neuromas, these cysts do not cause nerve symptoms and a Tinel sign is not present.Nodular fasciitis: a firm, reactive soft tissue proliferation that may grow rapidly on the volar surface of the forearm or hand. The location may suggest a nerve tumor and the aggressive spread mimics sarcoma. Although most nerve tumors are mobile in the transverse plane, palpation of nodular fasciitis reveals dense adhesions to the adjacent subcutaneous tissue.Patients with NF type I may have multiple nerve tumors, along with features such as café-au-lait spots, freckling in the axilla or groin, optic pathway tumors, iris hamartomas, and bone dysplasias. In patients with NF type 1, rapid growth of a neurofibroma, severe pain, and a new neurologic deficit often herald malignant degeneration.Examination techniques include the following:Palpation: The examiner moves the mass transversely and longitudinally. Nerve tumors may be translated transversely but are tethered in the longitudinal plane.Sensory testing using Semmes-Weinstein monofilament. Early nerve compression increases threshold, whereas innervation density (two-point) remains normal. In a busy clinical practice, light moving touch may be as reliable (Stauch).12The examiner assesses visible atrophy and weakness in motor units innervated by the affected nerve. Manual strength testing is usually normal.Direct pressure is applied over the nerve just proximal to the mass. Nerves under compression by a mass are sometimes sensitive to touch and may produce paresthesias when manipulated.The nerve is percussed immediately adjacent to the mass. A positive result is paresthesias in the cutaneous distribution of the nerve. The Tinel sign is positive only when an injured nerve is attempting to regenerate. Most nerve tumors do not have a positive Tinel sign.
IMAGING AND OTHER DIAGNOSTIC STUDIES
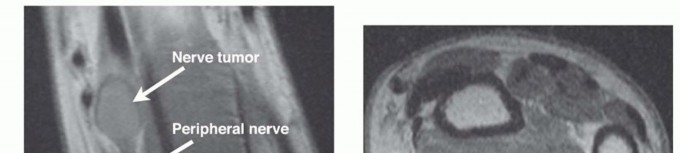
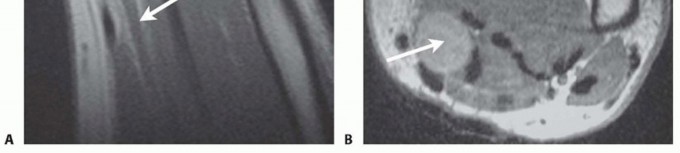
FIG 3 • A. Cross-sectional imaging of a BPNST reveals the mass to be contiguous with normal axons proximally. B.MRI of a benign nerve sheath tumor (arrow) often demonstrates a high fat content, seen best on T1-weighted images.
DIFFERENTIAL DIAGNOSIS
NeuromaLipofibromatous hamartoma (fibrofatty infiltration) Nerve sheath ganglionIntraneural tumors of nonneural origin Intraneural lipomaIntraneural hemangioma
NONOPERATIVE MANAGEMENT
In the absence of rapid growth, pain, or nerve dysfunction, it is reasonable to observe a distal upper extremity mass. An MRI may be obtained to identify features consistent with a BPNST and to exclude signs of malignancy (see earlier).Patients with NF type I often have multiple neurofibromas, including dermal and plexiform types.Dermal neurofibromas grow through the dermis and subcutaneous tissue to form plaque-like swellings. Although sometimes unsightly, these tumors are routinely observed, as the surgical defects are no more cosmetically pleasing.Plexiform neurofibromas are visible as nodular masses lying longitudinally along the course of peripheral nerves. These tumors must be carefully followed as progression to a MPNST (neurofibrosarcoma) is common.Pain is the most predictive symptom of malignant change. If there is no concern for malignancy, surgical excision is generally avoided, as it frequently results in nerve deficits postoperatively.Children and young adults may develop masses of fibrofatty tissue infiltrating major nerves and their branches,particularly the median nerve.These lipofibromatous hamartomas cause slow progressive nodular swelling and, at times, distal soft tissue overgrowth (macrodactyly).When asymptomatic, nonoperative management may be preferred, particularly if MRI shows pathognomonic features of this lesion.15Carpal tunnel symptoms may be treated with limited surgery, including an open carpal tunnel release and a definitive biopsy of a small cutaneous branch of the nerve.
SURGICAL MANAGEMENT
An isolated distal upper extremity mass is treated surgically for definitive diagnosis, to control symptoms, or to exclude malignancy.
PREOPERATIVE PLANNING
MRI is reviewed to confirm characteristics of a BPNST and to plan a surgical approach. Nerve reconstruction options are discussed with the patient.We consider synthetic absorbable nerve conduits for defects of up to 2 cm, particularly in the palm.We avoid conduits when there is any concern of extrusion (eg, about joints in the digits) or in superficial sites where foreign body reaction may be confused with a tumor recurrence.The medial antebrachial cutaneous nerve (MABC) is a suitable graft for the common and proper digital nerves.A sural nerve cable graft may be necessary for major peripheral nerve defects.If significant nerve dysfunction is present before surgery (or is expected afterward), consideration should be given to performing concomitant tendon transfers, particularly in adults.
POSITIONING
The patient is positioned supine with the affected extremity placed on a hand table. A brachial tourniquet is applied proximally, allowing access to the medial elbow for MABC nerve harvest if necessary.If sural nerve harvest is considered a possibility, we place a proximal thigh tourniquet and prepare and drape the contralateral lower extremity so that a second team may operate unencumbered.
APPROACH
The surgical approach varies with tumor location.A midlateral approach to digital nerve lesions allows excellent visualization of the tumor, protection of the adjacent digital artery, and good soft tissue coverage of the adjacent flexor tendon sheath.P.1326Lesions in the palm are approached with a Brunner zigzag type of skin incision, which provides excellent visualization and minimizes restrictive postoperative longitudinal scar formation.An open carpal tunnel approach is included for tumors close to the median nerve to decrease nerve compression from postoperative edema.Any suspected malignancy is managed according to the principles described in the oncology section of thistext: A biopsy incision must allow optimal definitive resection options later. For example, a biopsy of a possible neurofibrosarcoma of the radial sensory nerve should be made through the mobile wad compartment as opposed to the more familiar Henry approach to this region.
TECHNIQUE
ENUCLEATION




TECH FIG 1 • A. Nerve fascicles and fascicular groups are displaced by a schwannoma. B. The tumor may be “shelled out” from between the splayed fascicles. C. Intact fascicles after tumor resection. D. Specimen.
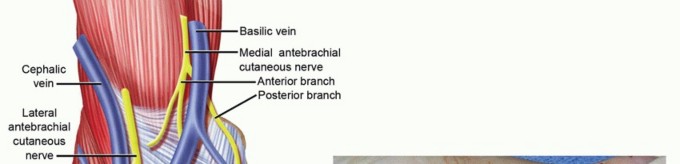


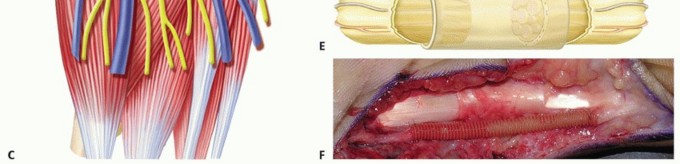
TECH FIG 2 • A. Fascicles are intertwined with tumor cells in a neurofibroma; tumor resection often requires excising a segment of nerve. B. A neurofibroma of the posterior interosseous nerve (PIN). This tumor was inseparable from normal nerve fascicles and excision resulted in permanent loss of finger extension. C. Branches of the MABC run with the basilic vein. The anterior branch is a good match for a digital nerve and can be harvested near the elbow. D. The ulnar digital nerve of the thumb has been grafted with the MABC in this patient, with prior nerve tumor resection and iatrogenic soft tissue loss. E. Nerve conduits provide an environment for nerve regeneration and have been shown to be as good as or better than nerve grafts in many situations. F. A digital neurofibroma was resected and a nerve conduit placed to bridge the intercalary defect. The soft tissues were slow to heal due to motion about the conduit at the metacarpophalangeal joint. Newer, less rigid collagen nerve guides may be better suited for use around the finger joints; however, human trials are lacking.




TECH FIG 3 • A. Painful expanding soft tissue mass along the common digital nerve to the third web space. The middle and ring fingers had slowly lost sensibility on the affected sides. B. MRI shows that the mass originates from the median nerve and extends to the proximal interphalangeal joint. Low-intensity normal nerve fascicles are seen coursing through the high-intensity fatty mass. C. At surgery, normal fascicles cannot be distinguished from the fibrofatty proliferation. D. Specimen. E. Sural nerve graft to the middle and ring finger proper digital nerves. Sagittal plane MRI images will show the extent of the lesion (TECH FIG 3B).Surgical exposure begins with an open carpal tunnel release to identify the transition zone between normal and abnormal nerve. The incision is carried distally in a Brunner zigzag type of fashion to find the end of the lesion (TECH FIG 3C).The hamartoma is excised en bloc at healthy-appearing fascicular margins (TECH FIG 3D). A sural nerve is harvested and interposed as a cable graft (TECH FIG 3E).Diagnosis1. A nerve tumor must be part of the differential diagnosis for any distal upperextremity mass.2. Anticipation allows for appropriate preoperative planning and discussions with the patient.Nonsurgicalmanagement1. Watch for signs of malignancy, including increasing nerve dysfunction, rapidgrowth, and pain.2. Plexiform neurofibromas seen in patients with NF type 1 have a high risk for malignant change.Surgicalapproach1. Masses should be resected through an extensile approach; avoid transverseincisions.2. Tumors that are invasive into the adjacent tissue are likely malignant. An incisional biopsy should be performed and the wound closed.Tumorresection1. Loupe magnification and microinstruments facilitate enucleation of a tumor(schwannoma).2. A microscope should be available should microdissection or nerve resection and reconstruction become necessary (neurofibroma).P.1329
PEARLS AND PITFALLS
POSTOPERATIVE CARE
At a minimum, short arcs of joint motion are initiated early to discourage adhesion formation between the cutaneous scar and the underlying nerve.If necessary, the end range of motion may be avoided for up to 1 month to protect nerve repairs or reconstructions.When axons have been injured, a hand therapist may assist with desensitization or sensory reeducation. A Tinel sign may be followed for reinnervation along the course of the affected nerve.Late changes in nerve function or swelling suggest the possibility of recurrence.
OUTCOMES
Transient paresthesias, numbness, or weakness are common after enucleation of a schwannoma (75%); however, long-term nerve function is generally the same as or improved compared to the preoperativestate with a recovery rate of 95%.10 Tumor recurrence is rare.Permanent neurologic deficits follow en bloc resection of a neurofibroma, thus limiting the surgicalindications for this procedure. Microdissection preserves nerve function13 but likely has an increased risk of recurrence.Resection of a lipofibromatous hamartoma of the median nerve (including partial excision or interfascicular dissection) often results in permanent nerve deficits. There is limited long-term follow-up for nerve grafting of these lesions.
COMPLICATIONS
Loss of nerve function after tumor resection. Although this is more common in excision of neurofibromas, it is possible in enucleation of schwannomas (18%). The risk of major neurologic deficit or severe neuropathic pain and the fact that these complications may warrant reexploration with or without graftingshould be discussed with the patient.10Loss of motion due to prolonged immobilizationNeuroma formation at a nerve donor site (eg, MABC neuroma) Wound breakdown over a nerve conduit, especially in the digits
REFERENCES
- Colon F, Upton J. Pediatric hand tumors. A review of 349 cases. Hand Clin 1995;11:223-243.
- Evans DG, Baser ME, McGaughran J, et al. Malignant peripheral nerve sheath tumours in neurofibromatosis 1. J Med Genet 2002;39: 311-314.
- Forthman CL, Blazar PE. Nerve tumors of the hand and upper extremity. Hand Clin 2004;20:233-242.
- Hajdu SI. Peripheral nerve sheath tumors. Histogenesis, classification, and prognosis. Cancer 1993;72:3549-3552.
- Holdsworth BJ. Nerve tumours in the upper limb. A clinical review. J Hand Surg Br 1985;10(2):236-238.
- Houpt P, Storm van Leeuwen JB, van den Bergen HA. Intraneural lipofibroma of the median nerve. J Hand Surg Am 1989;14(4):706-709.
- Kehoe NJ, Reid RP, Semple JC. Solitary benign peripheral-nerve tumours. Review of 32 years' experience. J Bone Joint Surg Br 1995;77(3):497-500.
- King AA, Debaun MR, Riccardi VM, et al. Malignant peripheral nerve sheath tumors in neurofibromatosis 1. Am J Med Genet 2000;93:388-392.
- Kransdorf MJ, Jelinek JS, Moser RP Jr. Imaging of soft tissue tumors. Radiol Clin North Am 1993;31:359-372.
- Park MJ, Seo KN, Kang HJ. Neurological deficit after surgical enucleation of schwannomas of the upper limb. J Bone Joint Surg Br 2009;91(11):1482-1486.
- Rinaldi E. Neurilemomas and neurofibromas of the upper limb. J Hand Surg Am 1983;8(5 pt 1):590-593.
- Strauch B, Lang A, Ferder M, et al. The ten test. Plast Reconstr Surg 1997;99:1074-1078.
- Strickland JW, Steichen JB. Nerve tumors of the hand and forearm. J Hand Surg Am 1977;2(4):285-291.
- Stull MA, Moser RP Jr, Kransdorf MJ, et al. Magnetic resonance appearance of peripheral nerve sheath tumors. Skeletal Radiol 1991;20:9-14.
- Toms AP, Anastakis D, Bleakney RR, et al. Lipofibromatous hamartoma of the upper extremity: a review of the radiologic findings for 15 patients. AJR Am J Roentgenol 2006;186:805-811.
