DEFINITION
Dupuytren disease (DD) is a fibroproliferative disorder that affects primarily the palmar fascia of the hand, with occasional secondary involvement of other areas in the hand as well as remote tissues. DD has a strong genetic origin that is suggested not only by population studies and family clustering but also by genomewide association study,15 which suggest that chromosomes 6, 11, and 16 may contain genes for the disease and that multiple other genes may be involved in its etiology.It is a sui generis condition that clinically and pathophysiologically resembles no other known condition. Although physiologically DD bears a resemblance to the processes associated with normal wound healing, the difference is the perpetual and progressive proliferation with abnormal collagen deposition and resultant tissue contracture.Attempts to classify DD under other headings such as inflammatory and neoplastic disorders have not been born out.
ANATOMY




FIG 1 • A. The central aponeurosis is the core of DD activity and has a triangular shape with a proximal apex.


PATHOGENESIS




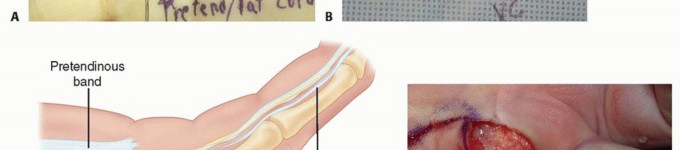
FIG 2 • A,B. Pretendinous cord and a nodule in the palm in line with the ring finger causing MCP flexion contracture. C. Two pretendinous cords in the palm in line with the small and ring fingers causing MCP and PIP flexion contracture of the small finger. A small proximal commissural cord in the first web space is also present. D. Diffuse Dupuytren palmar fascial disease is present with nodular thickening in the entire palm. The distorted anatomy of the neurovascular bundle, which is displaced medially and centrally, and later alsoproximally, is at risk for injury during surgery.23The natatory cord develops from the NL, converting the U-shaped web space fibers into a V shape, resulting in contracture of the second to fourth web spaces.This cord extends along the dorsal lateral aspect of the adjacent digits and is best detected by passively abducting the digits and at the same time flexing one digit and extending the other at the MCP joints.The most commonly encountered digital cord is the lateral cord, followed by the central and spiral cords. These are responsible for proximal interphalangeal (PIP) joint flexion contractures.The central cord is an extension of the pretendinous cord in the palm.The lateral cord originates from the lateral digital sheet and attaches to the skin or to the flexor tendon sheath near the Grayson ligament. The lateral cord causes a contracture of the PIP joint but can also rarely cause a distal interphalangeal joint contracture.The abductor digiti minimi cord, also known as theisolated digital cord, takes origin from the abductor digiti minimi tendon but may also arise from adjacent muscle fascia at the base of the proximal phalanx.It courses superficial to the neurovascular bundle and infrequently entraps and displaces the bundle towardthe midline.It inserts on the ulnar side of the base of the middle phalanx but may attach on the radial side or have an additional insertion in the base of the distal phalanx, causing a distal interphalangeal joint contracture.The distal commissural cord develops from the diseased distal commissural ligament, which is the radial extension of the NL. The proximal commissural cord originates from the proximal commissural ligament, which is the radial extension of the TLPA.Both of these cords cause first web space contracture.The thumb pretendinous cord originates from the thumb pretendinous band and causes thumb MCP joint flexion deformity, which is uncommon.
NATURAL HISTORY
DD has three clinical phases: early, intermediate, and late.16Skin changes with loss of normal architecture and skin pitting characterize the early phase.Nodules and cords form during the intermediate phase.Contractures mark the late phase, with the MCP joint most frequently affected, followed by the PIP joint.
PATIENT HISTORY AND PHYSICAL FINDINGS
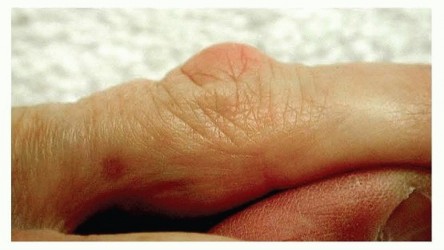
FIG 3 • A Garrod node over the dorsum of the PIP joint. DD may affect areas outside the palmar surface of the hand.Ectopic disease can be either regional in the upper extremity or distant in other parts of the body.Garrod nodes are different from knuckle pads, occur on the dorsum of the hand, and are almost alwayslimited to the finger (FIG 3). We have shown that DD nodules are pathognomonic of DD, whereas knucklepads demonstrate similar prevalence in normal and DD populations.18 Distant ectopic DD affects the plantar fascia and male genitals.Patients said to express a Dupuytren diathesis or genetic predisposition typically have faster and more severe development of the condition.Positive family historyYoung age of onsetEctopic sites of fibromatosis such as the dorsal digital area (Garrod nodes), plantar fascia (Ledderhose disease), and male genitals (Peyronie disease)
DIFFERENTIAL DIAGNOSIS
Non-DD19Occurs in a diverse ethnic group, is unilateral and nonprogressive, usually involves a single digit, and frequently follows trauma or surgeryPatients with this disease rarely require surgical treatment. Confusing this with DD will produce contrasting epidemiologic data.Epithelioid sarcomaOccupational thickening and callus formation that mimic Dupuytren nodulesPalmar subcutaneous soft tissue lesions, such as localized pigmented villonodular synovitis, palmar ganglions, and inclusion cystsStenosing tenosynovitis without triggering can be associated with thickening and adherence of the skin to the underlying flexor tendon sheath.Prominent flexor tendons can be confused with pretendinous cords because of attenuation of annular pulleys, as seen in rheumatoid arthritis.
NONOPERATIVE MANAGEMENT
No treatment is necessary for non-DD.Observation is appropriate for nonprogressive DD with minimal contracture and without compromise of function.Surgical treatment for minor disease or pitting can result in a disease flare and must be avoided.Basic science research has shown the potential of certain local agents in the treatment of DD. These include calcium channel blockers, nifedipine, and verapamil,20 especially for early stages of the disease.Steroid injection of nodules has been used to suppress the disease.
MINIMALLY INVASIVE TREATMENT METHODS
Percutaneous fasciotomy was used initially by the British surgeon Sir Astley Cooper in the early 19th century. The appeal for this procedure has recently reemerged in the pursuit of lower morbidity and fewer complications that may be encountered with conventional open surgical treatment.Needle aponeurotomy and collagenase1,10 injection have recently been used for DD more broadly by treating surgeons and gained appeal among patients because of their “noninvasive” nature. These procedures, however, are mistakenly labeled as nonoperative treatment methods. In fact, these are minimally invasive procedures, which create distinct deep soft tissue wounds with the potential for accidental injury to neurovascular structures or infection.For elderly patients with comorbidities, minimally invasive procedures especially percutaneous fasciotomy can be a practical approach for the treatment of DD.
PROCEDURES


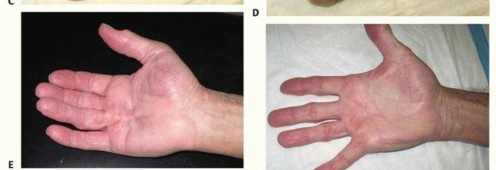
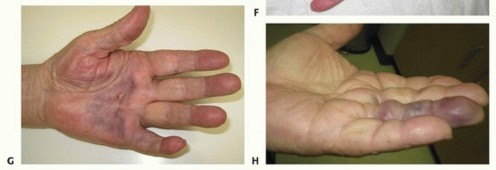
FIG 4 • A. A patient with DD pretendinous digital spiral cord affecting the small finger. B. Combined needle fasciotomy in the palm and limited open fasciectomy in the digit were done. C. Two weeks postoperatively, the patient had satisfactory correction of the flexion deformity. D. He had near full flexion. E. A patient with pretendinous cord in the palm along the ring finger with moderate MCP joint contracture, immediately after collagenase injection which is an ideal indication for this treatment. F. Six weeks after collagen injection showing satisfactory correction of the deformity. G. Second day after collagenase injection of a pretendinous cord showing the ecchymosis in the palm. H. Another patient the second day after collagenase injection of a nonspiral digital cord in the ring finger showing the digital ecchymosis.(continued)
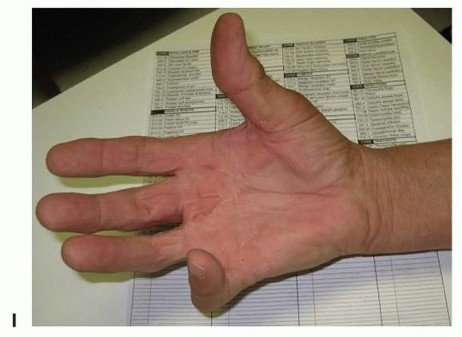
FIG 4 •(continued)I. A patient was referred for treatment with severe Dupuytren diathesis, a condition with predisposition to recurrence, showing disease recurrence, after surgical treatment and six collagenase injections, all were done in another facility. Collagenase InjectionCollagenase injection is a staged office procedure done on two separate consecutive days.During the first visit, the diseased pretendinous or digital cord is injected with a 10,000 units (0.58 mg) of collagenase clostridium histolyticum using an insulin syringe (FIG 4E). Every effort is made not to allow the collagenase to extravasate subcutaneously or deep to the cord. The patient is instructed to avoid applying pressure to the site or using the hand.During the second visit on the following day, finger manipulation is done by passive extension to rupture the cord and achieve extension. The manipulation is often performed with local anesthetic injected into the affected site(s).The hand is immobilized in a splint for night use for 4 weeks (FIG 4F). If the cord does not rupture, the procedure is repeated 4 weeks later. If the second procedure fails, then an open method is used 2 to 3 months later. Multiple cords in the same hand should be treated at different times.Complications include ecchymosis (FIG 4G,H), which is common and usually resolves within 3 weeks; failure to rupture the cord; possible infiltration of the collagenase into the flexor tendon, causing tendon rupture26; potential neurovascular injury; and disease recurrence, which is common especially amongpatients with Dupuytren diathesis (FIG 4I).
SURGICAL MANAGEMENT
Surgery remains the most widely used treatment method for symptomatic DD especially in primary cases with severe and multiple digit involvement and in recurrent cases.Outpatient surgery offers substantial savings and should be used in an otherwise healthy patient with moderate hand involvement.Local, regional, or general anesthesia can be used depending on the procedure performed.Flexion contractures of the MCP joint of greater than 30 degrees and PIP flexion contractures of 15 degrees interfere with function and, in the presence of a well-developed cord, are indications for surgical treatment.The outcome after surgery for MCP joint contracture is more successful than that for PIP joint contracture.PIP joint checkrein release may be indicated if 40 degrees of residual flexion is present after conventional fasciectomy.
PROCEDURES
Percutaneous FasciotomyPercutaneous fasciotomy is indicated for palmar cords in elderly unhealthy patients.This technique carries a higher risk for complications when performed in the thumb as compared to the digits.In severe cases, this technique may be useful as a preliminary procedure before definitive removal of diseased tissue.Injuries to flexor tendons and digital nerves as well as chronic regional pain syndromes have been reported after percutaneous releases.Open Palm FasciectomyThis method was first used by Dupuytren, who left the transverse palmar incision wound open after fasciectomy.Leaving the wound open is indicated for extensive involvement of the palmar fascia and if primary closure is not possible and skin grafting is not desired.Satisfactory results with this method continue to be reported in the literature,8,12,25 including less pain, better motion, and low rates of complication. The primary disadvantage is prolonged postoperative wound healing.Partial FasciectomyPartial fasciectomy is the excision of the diseased tissue with preservation of normal-appearing fascia.Other terms for this procedure are selective, regional, or limited fasciectomy.Partial fasciectomy remains the most widely used technique for treatment of DD among hand surgeons today. It is associated with a lower recurrence rate than fasciotomy.DermofasciectomyDermofasciectomy involves excision of skin and diseased tissue simultaneously followed by grafting of the skin defect.9Dermofasciectomy is considered the procedure of choice by many surgeons for recurrent or aggressive disease with marked adherence of skin to underlying diseased cords. It was reported to have lower recurrence rates compared to other surgical techniques even for recurrent disease.11Extensive FasciectomyExtensive fasciectomy involves a wide, generous fasciectomy of diseased tissue involving most of the palmar fascial complex.This can be combined if necessary with partial fasciectomy in the digits.This technique is indicated when broad involvement of the palmar fascial complex is present.The NL and TLPA may be involved in severe DD and these can be included in the extensivefasciectomy.After extensive fasciectomy, the skin sometimes can be closed primarily. If a defect is present, the wound can be skin grafted or left open.P.1229Total or radical fasciectomy entails removal of the entire diseased and normal palmar fascia with or without excision of the overlying skin.This highly morbid, radical approach is rarely indicated.
POSITIONING


FIG 5 • A. Partial fasciectomy through a zigzag Brunner incision. B. A longitudinal incision closed with multiple Z-plasties.
APPROACH
The most commonly used incision is the zigzag Brunner incision (FIG 5A).A midline longitudinal incision that is closed with multiple Z-plasties can be also used (FIG 5B).Transverse palmar incisions can be used for the open palm method or for removal of extensive palmar fascial complex disease.Local rotation flaps sometimes should be used to cover exposed flexor tendons or neurovascular structures, and the remaining secondary defect can be grafted with full-thickness skin.
TECHNIQUE
PERCUTANEOUS FASCIOTOMY

TECH FIG 1 • The no. 11 blade is used to incise the midline cord to improve the PIP joint contracture in this elderly patient.






TECH FIG 3 • In a patient with recurrent DD with two pretendinous cords in the palm in line with the small and ring fingers causing severe MCP and PIP flexion contracture of the small finger, dermofasciectomy was done for the small finger and partial fasciectomy through a zigzag Brunner incision was done for the ring finger. Correction of the contractures was achieved. Skin shortage in the small finger was covered with a full-thickness skin graft from the volar wrist.

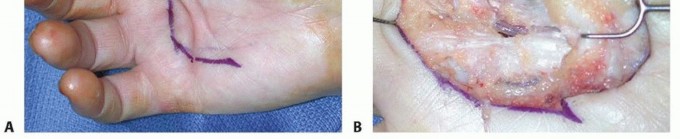
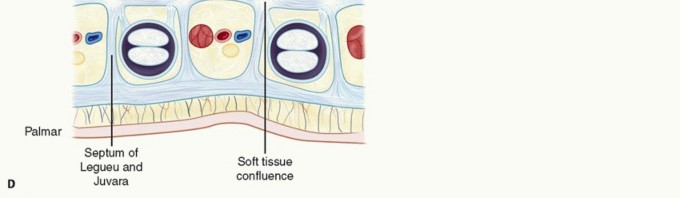
TECH FIG 4 • A. A U-shaped incision is planned in a patient with diffuse Dupuytren palmar fascial disease with nodular thickening in the entire palm. B. The diseased fascia is exposed after reflection of the proximally based skin flap.(continued) Keep the neurovascular structures in sight and protected throughout the procedure.The TLPA is usually involved, forming a transverse cord that extends from the ulnar to the radial aspect of the palm.This should be removed with the diseased tissue, along with any natatory cords.Divide all the septa of Legueu and Juvara to remove most of the diseased fascial carpet.If these septa are diseased, they will form vertical cords that should be incorporated in the mass of excised tissue.Release the tourniquet and achieve adequate hemostasis.Close the wound if possible (TECH FIG 4D), leaving a Penrose drain; it is removed on the second postoperative day.If skin shortage is present, perform full-thickness skin grafting. Alternatively, the wound can be left open as in the open palm method.P.1232 TECH FIG 4 •(continued)C. The excised specimen includes a pretendinous cord from the ring finger and diseased TLPA. D. The surgical wound after skin closure.


PEARLS AND PITFALLS
Injury to digital nerves is more common in cases with severe MCP and PIP joint contracture and altered nerve anatomy by a spiral cord. Such a complication is especially common in previously operated cases with an exuberant amount of scar tissue. Preventive measures include isolation of the neurovascular bundle by careful dissection, using loupe magnification, and knowledge of pathoanatomy. The dissection is carried out in a proximal to distal direction and is sometimes combined with distal to proximal dissection before removal of the diseased cord. If the nerve is transected, a primary repair should be performed.Vascular injury can be in the form of an arterial laceration, arterial spasm, intimal hemorrhage, or vessel rupture from vigorous correction of severe digital joint contracture. Arterial laceration that results in vascular compromise requires immediate repair or interposition vein graft. Arterial spasm and intimal hemorrhage are treated first by repositioning the digit in flexion, then irrigating with warm saline, applying topical lidocaine, even using intravenous heparin, and, if all else fails, vascular reconstruction.Separating diseased tissue from adherent skin is difficult, especially in recurrent cases. To reduce the risk of buttonholing the skin, using a no. 15C scalpel and the back of the knife blade as a dissector will allow precise separation of diseased tissue from normal skin. In addition, using an operating room light to transilluminate from the epidermal side of the skin allows visualization of the thickness of the flap and can alert the surgeon when the dissection is too superficial.
POSTOPERATIVE CARE
OPEN PALM FASCIECTOMY
The surgical wound is covered with sterile nonadhesive gauze, which can be changed daily. By 4 weeks, no dressings should be necessary.Forty-eight to 72 hours after surgery, the patient begins active range of motion every 2 to 3 hours butmaintains nocturnal extension splint immobilization.Whirlpool therapy can be used early in the postoperative period if unwarranted or excessive bleeding occurred.Wound healing takes place within 6 to 8 weeks, depending on the extent of the incision.
PARTIAL FASCIECTOMY AND DERMOFASCIECTOMY
Range-of-motion exercises are encouraged out of the splint after 1 week. The sutures are removed and splint use is discontinued 2 weeks after surgery in uncomplicated cases.Formal hand therapy is used after surgery for extensive disease, especially if residual flexion deformity is present. Range of motion alternating with extension splinting is emphasized.
OUTCOMES
The recurrence rate varies between 2% and 60%, with an average of 33%. This may be a true recurrence (recurrent disease at the operated site) or disease extension (disease outside the area of prior surgery). Recurrence is more common in patients with PIP joint involvement, disease in the small finger, more than one digit affected, a longer time since surgery, and a secondary fasciectomy.Werker et al24 in a 2012 literature review found that the reported recurrence rates in the literature ranged from 12% to 73% for patients treated with fasciectomy/aponeurectomy and from 33% to 100% for fasciotomy/aponeurotomy.Roush and Stern21 reported that the postoperative total range of motion of recurrent DD was better after fasciectomy and flap converge compared to skin grafting or arthrodesis.DD has intrigued basic scientists and clinicians for centuries. Both ancient7 and current publications5,22 underscore the interest in and the advances toward understanding the pathophysiology of this disease and improving its treatment.
COMPLICATIONS
Complications related to patient physiology include postoperative stiffness, chronic regional pain syndromes (CRPS), recurrence, and digital stiffness.4 The surgeon has little influence in preventing these complications.Early postoperative complicationsHematoma is prevented by tourniquet deflation and adequate hemostasis before wound closure. Deflating the tourniquet and assessing the skin vascularity before closure to ensure adequate circulation is the best way to prevent skin necrosis.P.1233Closure under tension should be avoided and consideration should be given to grafting or the open palm method if a primary closure is too tight.Skin necrosis develops after excessive thinning of skin flaps and tight skin closure. Small areas of skin necrosis may be allowed to heal by secondary intention, but large areas of necrotic tissue should be excised, and skin graft or flap coverage is done.A simultaneous carpal tunnel release with DD surgery, especially in women, is a predisposing factor toCRPS atraumatic technique and gentle handling of nerves and tissues during surgery reduces the riskof this complication.Late postoperative complicationsInclusion cysts can occur near the scar due to dermal tissue entrapment in the subcutaneous space. This can be prevented by careful attention to skin approximation during wound closure. The risk of hypertrophic scar formation is lessened by careful attention to placement of the skin incisions.
REFERENCES
- Badalamente M, Hurst L. Enzyme injection as nonsurgical treatment of Dupuytren disease. J Hand Surg Am 2000;25(4):629-636.
- Bilderback K, Rayan G. Dupuytren's cord involving the septa of Legueu and Juvara: a case report. J Hand Surg Am 2002;27(2):344-346.
- Bilderback K, Rayan G. The septa of Legueu and Juvara: an anatomic study. J Hand Surg Am 2004;29(3):494-499.
- Boyer M, Gelberman R. Complications of the operative treatment of Dupuytren's disease. Hand Clin 1999;15:161-166.
- Brenner P, Rayan G. Dupuytren's Disease: A Concept of Surgical Treatment. Vienna, Austria: Springer, 2002.
- Eaton C. Percutaneous fasciotomy for Dupuytren's contracture. J Hand Surg Am 2011;36(5):910-915.
- Elliot D. The early history of Dupuytren's disease. Hand Clin 1999; 15:1-19.
- Gelberman R, Panagis J, Hergenroeder P, et al. Wound complications in the surgical management of Dupuytren's contracture: a comparison of operative incisions. Hand 1982;14:248-254.
- Heuston J. The control of recurrent Dupuytren's contracture by skin replacement. Br J Plast Surg 1969;22:152-156.
- Hurst LC, Badalamente MA, Hentz VR, et al. Injectable collagenase clostridium histolyticum for Dupuytren's contracture. N Engl J Med 2009;361(10):968-979.
- Ketchum L, Hixson FP. Dermofasciectomy and full-thickness grafts in the treatment of Dupuytren's contracture. J Hand Surg Am 1987;12(5 pt 1):659-664.
- Lubahn J. Open-palm technique and soft-tissue coverage in Dupuytren's disease. Hand Clin 1999;15:127-136.
- Luck JV. Dupuytren's contracture; a new concept of the pathogenesis correlated with surgicalmanagement. J Bone Joint Surg Am 1959; 41-A(4):635-664.
- McFarlane RM. Patterns of the diseased fascia in the fingers of Dupuytren's contracture. Displacement of the neurovascular bundle. Plast Reconst Surg 1974;54:31-44.
- Ojwang JO, Adrianto I, Gray-McGuire C, et al. Genome-wide association scan of Dupuytren's disease. J Hand Surg Am 2010;35(12):2039-2045.
- Rayan G. Dupuytren disease: anatomy, pathology, presentation, and treatment. J Bone Joint Surg Am 2007;89(1):189-198.
- Rayan G. Palmar fascial complex anatomy and pathology in Dupuytren's disease. Hand Clin 1999;15:73-86.
- Rayan G, Ali M, Orozco J. Dorsal pads versus nodules in normal population and Dupuytren's disease patients. J Hand Surg Am 2010;35(10):1571-1579.
- Rayan G, Moore J. Non-Dupuytren's disease of the palmar fascia. J Hand Surg Br 2005;30(6):551-556.
- Rayan G, Parizi M, Tomasek J. Pharmacologic regulation of Dupuytren's fibroblast contraction in vitro. J Hand Surg Am 1996;21(6): 1065-1070.
- Roush T, Stern P. Results following surgery for recurrent Dupuytren's disease. J Hand Surg Am 2000;25(2):291-296.
- Tubiana R, Leclercq C, Hurst L, et al. Dupuytren's Disease. London: Martin Dunitz, 2000.
- Ulmas M, Bischoff R, Gelberman R. Predictors of neurovascular displacement in hands with Dupuytren's contracture. J Hand Surg Br 1994;19(5): 664-666.
- Werker P, Pess G, van Rijssen A, et al. Correction of contracture and recurrence rates of Dupuytren contracture following invasive treatment: the importance of clear definitions. J Hand Surg Am 2012; 37(10):2095-2105.
- Zachariae L. Operation for Dupuytren's contracture by the method of McCash. Acta Orthop Scand 1970;41:433-438.
- Zhang AY, Curtin CM, Hentz VR. Flexor tendon rupture after collagenase injection for Dupuytren contracture: case report. J Hand Surg Am 2011;36(8):1323-1325.
