DEFINITION
Cubital tunnel syndrome is a compression neuropathy of the ulnar nerve that occurs at or around the level of the elbow (cubisis Latin for “elbow”).Cubital tunnel syndrome is the second most common compression neuropathy of the upper limb requiring treatment after carpal tunnel syndrome.
ANATOMY
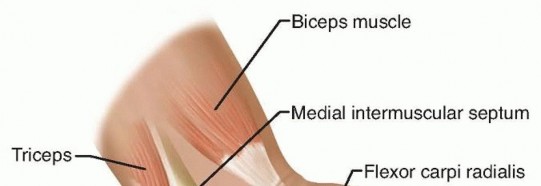
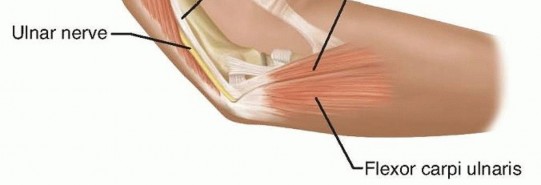
FIG 1 • Anatomy of the cubital tunnel. The arcuate ligament of Osborne at the cubital tunnel, which is the fibrous band extending from the medial epicondyle to the olecranon, can cause stenosis of the cubital tunnel and, thus, ulnar nerve compression.Distally, the nerve can be compressed as it passes between the two heads of the flexor carpi ulnaris (FCU), especially if each muscle head from the medial epicondyle and the olecranon converge close to the elbow joint.The presence of an anconeus epitrochlearis (FIG 2), an anomalous thin muscle extending from the triceps or olecranon to the medial epicondyle, also can cause ulnar nerve compression.The medial antebrachial cutaneous nerve and the medial brachial cutaneous nerve both emanate directly from the medial cord and are thus not ulnar nerve branches, but they importantly may lie in the surgical field. They are usually found deeper than expected, along the fascia of the triceps, brachialis, and FCU.
PATHOGENESIS

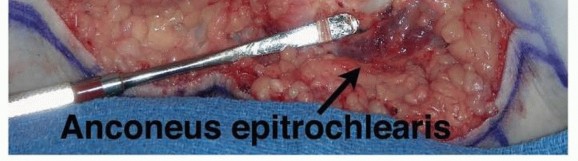


FIG 3 • A. “Perched” ulnar nerve. The nerve subluxates anteriorly, sitting on top of the medial epicondyle with the elbow in flexion. B. Wasting of first dorsal interosseous nerve. (A: Copyright Amy Ladd, MD.) Elbow flexion increases pressure on the nerve and decreases the volume of the cubital tunnel, resulting in compression of the nerve.7
NATURAL HISTORY
Without operative intervention, about half of mild cases can resolve with activity modification.13,14 No long-term studies have been done of the natural history for severe disease.
PATIENT HISTORY AND PHYSICAL FINDINGS
Subjective complaints include numbness in the small and ring fingers, often with accompanying burning pain around the medial epicondyle. Symptoms may be worse at night.As the disease progresses, patients may complain of weakness or clumsiness of their hands. More advanced disease will demonstrate wasting of the intrinsics and clawing of the ring and small fingers.Systemic diseases such as diabetes, amyloidosis, or alcoholism may cause peripheral neuropathy, which can mimic the symptoms of a compressive neuropathy.A smoking history is important not only for impaired vascularity but because it may point to the rare Pancoast tumor, an apical lung tumor, which causes plexus compression, mimicking the symptoms of cubital tunnel syndrome.Elbow trauma can create deformity, causing ulnar nerve compression. Deformities include a cubitus valgus, cubitus varus, or malunion. The elbow trauma can be remote and result in tardy ulnar nerve palsy.Look for atrophy of the intrinsic muscles of the hand or a clawed posture of the ring and small fingers. Check for masses around the elbow.Palpate the elbow and hand to evaluate for tender masses or other anomalous elbow anatomy.Put the elbow through its range of motion and assess whether the ulnar nerve subluxates or perches at the medial epicondyle with elbow flexion (FIG 3A).2Visible atrophy of the first dorsal interosseous nerve correlates with significant ulnar nerve compression and can indicate significant motor impairment (FIG 3B).Perform a sensory examination of the hand, using Semmes-Weinstein monofilaments to obtain threshold measurements. Evaluate sensation on the ulnar dorsum of the hand. If sensation is normal, it suggests the problem may be distal, at the level of Guyon canal.Clinical tests that can help with diagnosis include the following:Tinel test. This test may not be specific because many normal individuals will have a positive Tinel response to percussion.Elbow flexion test. This test is sensitive for cubital tunnel syndrome. Scratch collapse test can help localize the site of compression.3Crossed finger test. This test demonstrates weakness of dorsal and palmar interossei.Froment sign. A positive Froment sign indicates weakness of the adductor pollicis.Wartenberg sign (in which the small finger assumes an abducted posture with finger extension). This sign is the result of weakness in the palmar interossei, resulting in unopposed ulnar pull of the extensor digiti quinti.
IMAGING AND OTHER DIAGNOSTIC STUDIES
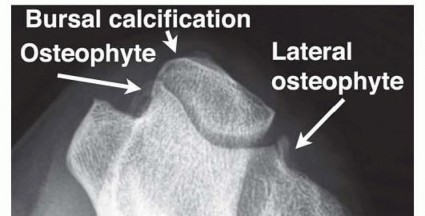

FIG 4 • Axial view of the elbow demonstrates a hooked osteophyte within the cubital tunnel as well as calcification in the bursa and osteophyte. (Copyright Amy Ladd, MD.)
DIFFERENTIAL DIAGNOSIS
Cervical spine disease affecting C8 and T1Compression of the inferior aspect of the brachial plexus from shoulder trauma Apical lung tumor (Pancoast tumor)Thoracic outlet syndromeEntrapment of the ulnar nerve at the wrist (Guyon canal)
NONOPERATIVE MANAGEMENT
Activity modificationUlnar nerve protection limiting microtrauma to the nerve through elbow padding and limiting direct pressure on the nerveMinimize prolonged elbow flexion, especially at night, through sleep modifications or splints.SplintingSplints to prevent elbow flexion; rigid splints are more effective but are less tolerated by patients. If persistent paresthesias exist, a trial of temporary full-time use is recommended. For milder cases, the splintis worn only at night.4Nonoperative treatment requires a trial of several months before determining its success.
SURGICAL MANAGEMENT
Surgical intervention should be considered for patients presenting with motor involvement or permanent sensory changes or for those who have failed nonoperative treatment.
PREOPERATIVE PLANNING
Review the history and physical examination.Review plain radiographs for evidence of old trauma, valgus or varus deformity, or loose bodies. Electrodiagnostic testing and examination may correlate with postoperative results.A patient with a visible and symptomatic subluxating nerve may be considered for a medial epicondylectomy or transposition.Patients with severe disease with muscle wasting are less likely to have complete recovery.10
POSITIONING
The patient usually is placed in the supine position.If a sterile tourniquet is preferred, drape out the forequarter. A standard tourniquet may be used, but position it high in the axilla, with good padding. A proximally placed tourniquet can be challenging to position in the obese arm in either circumstance because the tourniquet tends to gap distally. It is worth the extra time to position it properly because adequate hemostasis and visualized proximal dissection are important aspects of ulnar nerve surgery.The patient's shoulder is externally rotated and abducted on an arm table. The tourniquet is inflated after exsanguination of the arm.Folded towels stabilize and elevate the elbow (FIG 5).An obese patient with sleep apnea under peripheral nerve block (most commonly supra- or infraclavicular block) may require slight truncal elevation, which may be vexing for the surgeon.
APPROACH

FIG 5 • The arm is draped, the sterile tourniquet is placed proximally, and a bump under the elbow assists visualization. Alternatively, a proximal tourniquet may be placed before the arm is draped. P.844 Table 1 Techniques for Cubital Tunnel Release Technique|Advantages|Disadvantages|Contraindications|Indications---------In situ release Simplestdissection Does not devascularize the nerve with circumferential dissection Early mobilizationKeeps nerve in same tissue bedDoes not address subluxation of the nerveSubluxating ulnar nerveAbnormal elbow anatomyDiabetic patient Frail patient Patient with focalcompression distal to medial epicondyleEndoscopic releaseSmall incision Early mobilization Shortened recovery timeKeeps nerve in same tissue bedPotential iatrogenic nerve compressionAbnormal elbow anatomy Revision surgeryIn situ release with medial condylectomyPreserves vascular supply to the nerve Early mobilizationKeeps nerve in same tissue bedRisk of destabilizing the medial elbow by damaging the medial collateral ligament of the elbowTenderness at operative siteAbnormal elbow anatomyNot for throwing athletesPatients with mild to moderate symptomsAnterior subcutaneous transferPlaces the nerve in a fresh tissue bedNerve is superficial and may be more susceptible to trauma.Very thin patient Patient with a poor ulnar nerve bedGreater dissectionMore prolonged immobilizationPossible creation of new point of compressionfrom tumor,osteophyte, heterotopic bone Throwing athleteAnteriorintermuscular transpositionTension withelbow range of motion is minimized.Nerve is in fresh tissue bed.Greater dissectionNeed for longer immobilizationDiabetic patientPatient witha poor ulnar nerve bed from tumor, osteophyte, heterotopic boneAnteriorsubmuscular transpositionTension withelbow range of motion is minimized.Nerve is well padded.Greater dissectionNeed for longer immobilizationThin patientRepeat cubital tunnel release Patients with severe compression
TECHNIQUES
In Situ Release
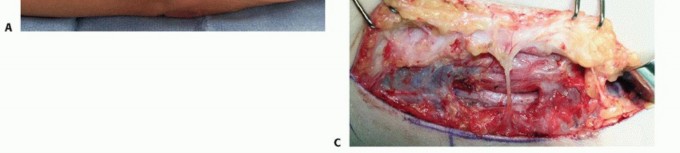
Center the longitudinal incision just anterior to the medial epicondyle, making an incision about 6 cm long (TECH FIG 1A).
Dissect through the fat, down to the level of the medial epicondyle.
IN SITU RELEASE
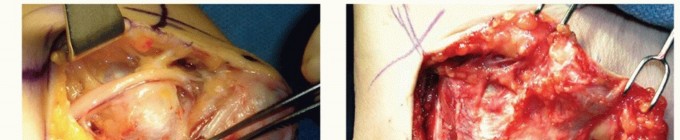
TECH FIG 1 • A. The standard incision, centered just anterior or posterior to the medial epicondyle. B,C.
TECH FIG 3 • Medial epicondylectomy. A. The medial epicondyle is exposed and the most prominent aspect is removed. We recommend removal of the most prominent and inferior portion, 2 to 3 mm in depth, to avoid disruption of the medial collateral ligament. B. Once the epicondylectomy is performed and the fascia closed, the elbow is flexed to visualize smooth movement of the nerve. The nerve no longer perches on the medial epicondyle. (Copyright Amy Ladd, MD.)


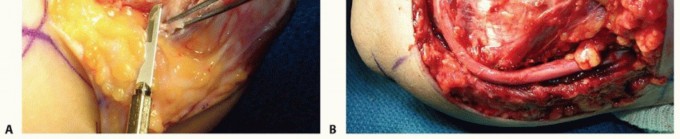
TECH FIG 4 • Anterior subcutaneous transposition. A. The subcutaneous flap at the level of the flexor pronator fascia has been developed and the nerve transposed anteriorly. B. A 1-cm fascial sling is developed from the flexor pronator mass to provide an inferior restraint for the transposed nerve. (A:




TECH FIG 5 • Intramuscular transposition. The nerve is placed in a tunnel in the muscle, and the fascia is closed. (Courtesy of William Kleinman, Indiana Hand Center.)
ANTERIOR SUBMUSCULAR TRANSPOSITION


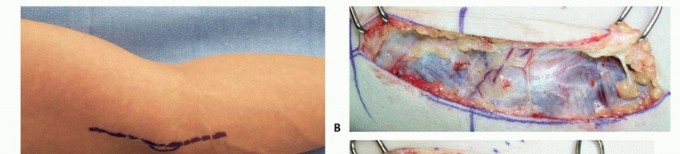
TECH FIG 6 • Submuscular transposition. The flexor pronator mass is incised (A), and the nerve is passed deep to the flexor pronator muscle mass (B). Sutures are in place to repair the muscle origin following use of a simple straight incision. (A: Copyright Amy Ladd, MD; B: Courtesy of Thomas R. Hunt, III, MD.) The median nerve and brachial artery lie in this plane. Transpose the ulnar nerve in the medial position (TECH FIG 6B).Take care to avoid injury to the medial collateral ligament complex.Flex the elbow and repair the flexor pronator mass with 3-0 Ethibond suture.Place a drain.The arm is immobilized with a pronated forearm in an elbow splint for 2 to 3 weeks at 45 to 60 degrees of flexion with progressive protected mobilization.P.848
PEARLS AND PITFALLS
Dissection ▪ Avoid cutting the medial brachial and antebrachial nerves. Damage to these nerves is the most common cause of pain after cubital tunnel release.9,161. Make an adequate proximal dissection: Follow the nerve to the crossover of theanterior to posterior compartment, where a thin or thick fascial band is present at the septum, or, rarely, the arcade of Struthers. Make certain the tourniquet is high enough to reach this spot, usually 5-8 cm above the epicondyle.2. Make an adequate distal dissection: Follow the nerve several centimeters into the muscle bellies to ensure a full release, including the fascia of the FCU encasing its branches.Transposition ▪ Preserve the longitudinal blood supply to the nerve.3. If transposing the nerve, ensure that a new point of compression is not created. Compression may be created at the following sites: proximally at the crossover from anterior to posterior, the intermuscular septum just proximal to the medial epicondyle, the flexor pronator mass if submuscular or intramuscular transposition is performed, and the entrance to the FCU muscle bellies.
POSTOPERATIVE CARE
Postoperative care instructions are given individually with the discussion of each technique. In general, the more extensive the dissection, the more protected postoperative splinting and mobilization is required.Strengthening may begin a few weeks after an in situ decompression, for example, and 6 to 8 weeks following a submuscular transposition.
OUTCOMES
Overall, all procedures have a success rate of about 90% for mild cases. The rate of total relief decreases as severity of disease increases.11Postoperative outcomes are proportional to disease severity: That is, severe disease is less likely to achieve full recovery.6Recent studies suggest that outcomes are similar for the different procedure types.1,6,12
COMPLICATIONS
Pain at the elbowDecreased sensation around the scar Incomplete symptom reliefPainful neuroma of cutaneous nerves Symptomatic subluxating nerveInjury to motor branches to the FCU
REFERENCES
- Bartels RH, Verhagen WI, van der Wilt GJ, et al. Prospective randomized controlled study comparing simple decompression versus anterior subcutaneous transposition for idiopathic neuropathy of the ulnar nerve at the elbow. Part 1. Neurosurgery 2005;56:522-530.
- Calfee RP, Manske PR, Gelberman RH, et al. Clinical assessment of the ulnar nerve at the elbow: reliability of instability testing and the association of hypermobility with clinical symptoms. J Bone Joint Surg Am 2010;92(17):2801-2808.
- Cheng CJ, Mackinnon-Patterson B, Beck JL, et al. Scratch collapse test for evaluation of carpal and cubital tunnel syndrome. J Hand Surg Am 2008;33(9):1518-1524. doi:10.1016/j.jhsa.2008.05.022.
- Dellon AL, Hament W, Gittelshon A. Nonoperative management of cubital tunnel syndrome: an 8-year prospective study. Neurology 1993;43:1673-1677.
- Eaton RG, Crowe JF, Parkes JC III. Anterior transposition of the u1nar nerve using a noncompressing fasciodermal sling. J Bone Joint Surg Am 1980;62(5):820-825.
- Gervasio O, Gambardella G, Zaccone C, et al. Simple decompression versus anterior submuscular transposition of the ulnar nerve in severe cubital tunnel syndrome: a prospective randomized study. Neurosurgery 2005;56:108-117.
- Iba K, Wada T, Aoki M, et al. Intraoperative measurement of pressure adjacent to the ulnar nerve in patients with cubital tunnel syndrome. J Hand Surg Am 2006;31;553-558.
- Kleinman WB, Bishop AT. Anterior intramuscular transposition of the ulnar nerve. J Hand Surg Am 1989;14:972-979.
- Lowe JB III, Maggi SP, Mackinnon SE. The position of crossing branches of the medial antebrachial cutaneous nerve during cubital tunnel surgery in humans. Plast Reconstr Surg 2004;114:692-696.
- Matsuzaki H, Yoshizu T, Maki Y, et al. Long-term clinical and neurologic recovery in the hand after surgery for severe cubital tunnel syndrome. J Hand Surg Am 2004;29;373-378.
- Mowlavi A, Andrews K, Lille S, et al. The management of cubital tunnel syndrome: a meta-analysis of clinical studies. Plast Reconstr Surg 2000;106:327-334.
- Nabhan A, Ahlhelm F, Kelm J, et al. Simple decompression or subcutaneous anterior transposition of the ulnar nerve for cubital tunnel syndrome. J Hand Surg Am 2005;30:521-524.
- O'Driscoll SW, Horii E, Carmichael SW, et al. The cubital tunnel and ulnar neuropathy. J Bone Joint Surg Br 1991;73(4):613-617.
- Padua L, Aprile I, Caliandro P, et al. Natural history of ulnar entrapment at elbow. Clin Neurophysiol 2002;113:1980-1984.
- Practice parameter for electrodiagnostic studies in ulnar neuropathy at the elbow: summary statement. American Association of Electrodiagnostic Medicine, American Academy of Neurology, American Academy of Physical Medicine and Rehabilitation. Muscle Nerve 1999;22(3):408-411.
- Sarris I, Göbel F, Gainer M, et al. Medial brachial and antebrachial cutaneous nerve injuries: effect on outcome in revision cubital tunnel surgery. J Reconstr Microsurg 2002;18:665-670.
- Siqueira MG, Martins RS. The controversial arcade of Struthers. Surg Neurol 2005;64(suppl 1):S17-S20.
- Zajonc H, Momeni A. Endoscopic release of the cubital tunnel. Hand Clin 2014;30(1):55-62.
