Surgical Treatment of Carpal Bone Fractures Excluding the Scaphoid
DEFINITION
These injuries include fractures of the lunate, triquetrum, pisiform, hamate body or hook, capitate, trapezoid, and trapezial body or ridge.Any fracture involving the carpal bones should raise suspicion of associated carpal instability.
ANATOMY
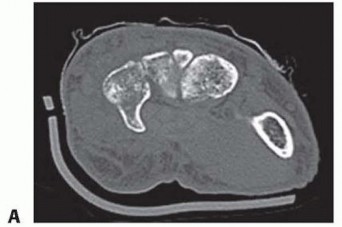

FIG 1 • A. CT scan showing hamate hook. B. CT scan showing trapezial ridge. The constricted neck portion of the capitate lies between the dense head proximally and the body distally. The body, which accounts for the distal half of the capitate, is rigidly constrained by its associations with the index, middle, and ring finger metacarpal bases; the trapezoid; and the hamate. As a result the capitate neck is a biomechanically vulnerable area.Transverse plane fractures through the capitate neck are reported as being the most common.Fractures across the neck place the capitate head at risk for avascular necrosis because the blood supply to the capitate flows retrograde toward the head proximally.
PATHOGENESIS
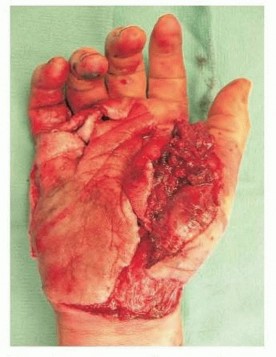
FIG 2 • Exploded hand is a constellation of injuries that can include CMC fracture-dislocations, longitudinal fractures of the metacarpals, severe thumb damage, and significant soft tissue damage. (Reprinted from Graham TJ. The exploded hand syndrome: logical evaluation and comprehensive treatment of the severely crushed hand. J Hand Surg Am 2006;31[6]:1012-1023; copyright 2006, with permission from Elsevier.) P.369More focused direct trauma to individual carpal bones may also cause a fracture. Examples of this include direct blows to the dorsum of the hand, typically causing capitate, hamate body, triquetrum, or trapezium fractures, or direct injury to the palmar surface of the hand usually from a racquet or club, often causing a hamate hook or trapezial ridge fracture.Indirect trauma includes the progressive perilunate instability patterns that are well described and may lead to fractures of the lunate, capitate, triquetrum, or other carpal bones.Scaphocapitate syndrome involves a dorsiflexion and radial deviation mechanism by which the scaphoid bone fractures and is followed by a fracture of the capitate through the neck in the coronal plane. The capitate head may rotate up to 180 degrees from its anatomic position.A progressive perilunate instability pattern can produce a similar coronal fracture through the capitate neck but normally without such a severe degree of capitate head rotation.Minor indirect trauma can cause isolated carpal bone fractures.The commonly seen avulsion fractures from the dorsum of the triquetrum may occur when a fall onto the palmar flexed wrist causes the dorsal radiotriquetral (also known asdorsal radiocarpal) ligament to avulse a portion of the dorsal cortex. However, this seemingly innocuous injury can be associated with significant radiocarpal and/or intracarpal instability patterns and the practitioner should carefully exclude these more severe injuries whenever treating a dorsal triquetral avulsion fracture.An impaction type of fracture of the triquetrum body may be seen more often in patients with an elongated ulnar styloid.
NATURAL HISTORY
The natural history of carpal bone fractures depends both on the specific bone in question as well as associated impairment of other structures.All of the carpal bones have at least three articular surfaces, except the pisiform, which articulates only with the triquetrum. Anatomic reduction of articular facets is a primary surgical goal in an effort to decrease the incidence and severity of posttraumatic arthritis.Avascular necrosis can have a profoundly negative impact on final outcome after carpal bone fracture.Concerns of vascular disruption arise when lunate and capitate fractures occur, although generally, fractures of the lunate are not associated with avascularity.The potential for nonunion is most often seen with hamate hook fractures, capitate neck fractures, and trapezial ridge fractures, especially Palmer type II fractures that involve the tip and not the base of the ridge.Barring nonunion, the related instabilities and involvement of other hand components in association with carpal fractures excluding the scaphoid are the most troublesome issues and will most significantly affect patient outcome.
PATIENT HISTORY AND PHYSICAL FINDINGS
Determining the mechanism of injury is the most important component of taking the patient's history.Neurovascular symptoms should be explored, especially when a severe crush or high-energy mechanism is involved, or in cases of hamate hook or pisiform fractures, with special attention to the ulnar neurovascular structures within Guyon's canal.A complete evaluation of the median, radial, ulnar, and digital nerves is warranted. Assessment of capillary refill, color, temperature, and Doppler signal determines the vascular status. Clinical or Doppler Allen examination may be warranted if radial and/or ulnar artery thrombosis or disruption is suspected.The examiner should observe the patient's hand and wrist for swelling, deformity, and skin and soft tissue injuries, including possible open fractures or fracture-dislocations.Swelling and soft tissue damage give an indication as to the severity of the injury. The presence of deformity alerts the examiner to possible carpal dislocations that require emergent reduction. Open fractures and fracture-dislocations will guide surgical management.The examiner should ask the patient where the pain is most significant. The examination should start away from, and progress toward, this point. The hand, forearm, and elbow should also be palpated to assess for possible associated injuries.The most obvious area of pain and tenderness is usually the most structurally significant. However, it may mask other more subtle injuries that should be detected by a more thorough global examination.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Routine AP, lateral, and oblique views of the wrist and hand are obtained (FIG 3A).Radiographs of the elbow and forearm are ordered if indicated.Dynamic radiographic images, including stress and distraction views, help to rule out carpal instability and may determine the ability to obtain closed reduction.Special views, often best performed with fluoroscopy, help to profile difficult-to-see structures.The hook of the hamate is evaluated with the carpal tunnel view or the supinated/oblique/radial deviation view with the thumb abducted (referred to as thepapillon view) (FIG 3B).The trapezial ridge is visualized on the carpal tunnel view (FIG 3C).The pisotriquetral joint is best seen on a 45-degree supinated lateral view of the wrist.Computed tomography (CT) scans effectively assess osseous detail and will often detect more subtle associated carpal fractures that may be missed on routine radiographs.CT is considered the imaging modality of choice for confirming a hamate hook fracture if plain films are nondiagnostic.
NONOPERATIVE MANAGEMENT
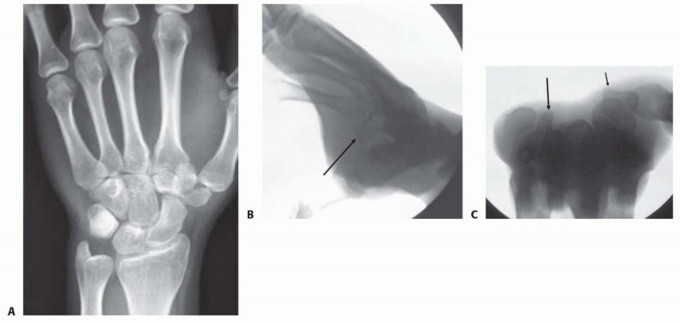
FIG 3•A.AP radiograph of wrist showing trapezial body fracture.B.Supination, oblique, radial deviation radiograph showing normal hamate hook (arrow).C.Carpal tunnel view showing normal hamate hook (large arrow) and trapezial ridge (small arrow).A specific fracture of note is the hamate hook.These fractures can be treated with cast immobilization if nondisplaced and acute (<1 month).There is a relatively high rate of symptomatic nonunion, and surgical intervention may eventually be necessary. Close follow-up to determine whether union has occurred is warranted because nonunions may lead to flexor tendon rupture.Similar to the treatment of the hamate hook, trapezial ridge fractures may be initially immobilized and later excised if symptomatic nonunion develops.
SURGICAL MANAGEMENT
INDICATIONS
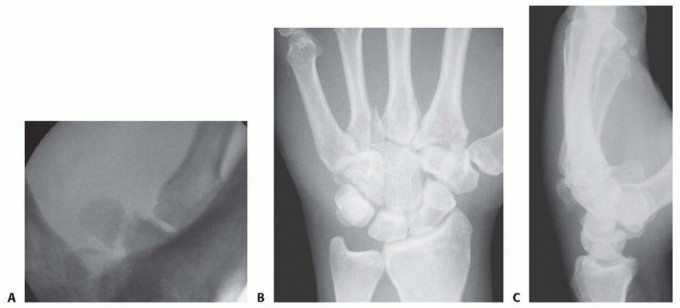
FIG 4 • Hamate fractures. A. Supination, oblique, radial deviation radiograph showing hamate hook fracture. B,C. AP and lateral radiographs of a hamate body dorsal shear fracture associated with the small finger and ring finger CMC articulation as well as a fracture of the base of the ring finger metacarpal. Capitate FracturesCapitate fractures are by and large associated with high-energy trauma to the wrist.In addition to fractures associated with progressive perilunate instability patterns and the scaphocapitate syndrome, capitate fractures may also occur due to axial loading along the middle finger ray or via direct trauma.If caused by axially directed forces, the fracture line is often in the frontal plane and involves the long finger CMC joint, similar to the hamate dorsal shear fractures described earlier. The capitate may be essentially divided in half in this frontal plane.In these cases, ORIF is performed through a dorsal approach.Truly isolated capitate fractures with minimal displacement heal by immobilization, but this often takes time.Trapezoid FracturesThe trapezoid is believed to be the least frequently fractured carpal bone.As with the other bones of the distal carpal row, assessment of the associated index CMC joint is necessary to rule out a fracture-dislocation.Frontal plane dorsal shear fractures of the trapezoid can destabilize the index CMC.These fractures and fracture-dislocations can often be treated by closed reduction and pinning.If an open approach is required to reduce the articular surface and CMC joint, a standard third and fourth extensor compartment interval dorsal approach may be used. Fixation can be accomplished with pins or screws.A limited exposure (as described in the following text) is an alternative.Trapezium FracturesFractures of the body of the trapezium nearly always involve one of its four articular facets and frequently lead to subluxation of the thumb CMC joint (FIG 5).P.372 FIG 5 • A,B. Trapezial body fractures.


PREOPERATIVE PLANNING
Examination under anesthesia, possibly with concomitant fluoroscopic imaging, helps confirm whether carpal instability coexists.The surgeon should ensure that all needed fixation implants and systems are available before bringing the patient to the operating room.A hand table, a well-padded upper arm tourniquet, and a mobile mini-fluoroscopy unit are used. Anesthesia and analgesia may be obtained through regional or general methods.
APPROACH
Carpal fractures may be approached dorsally, palmarly, radially, or ulnarly depending on the reduction needs, implants used, and location and characteristics of the fracture(s).Some surgeons use wrist or small joint arthroscopy as an aid to fracture reduction and management.
TECHNIQUES
Open Reduction and Internal Fixation of Lunate Fractures
Open Reduction and Internal Fixation of Lunate Fractures
INCISION AND DISSECTION
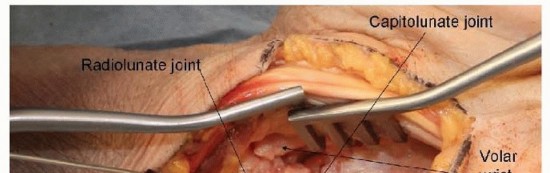
An extended carpal tunnel approach is used for palmar exposure.The incision begins in the palm, just ulnar to the thenar crease and in line with the radial border of the ring finger. If the surgeon is comfortable with the deep anatomy, especially the possible anatomic variations involving the thenar motor branch, the incision in the palm may also be along the thenar crease itself.The incision is extended proximally until the distal volar wrist crease is reached.A curved or zigzag continuation of the incision is made at the crease to avoid crossing perpendicular to the wrist crease and associated scarring and flexion contracture.The incision may be continued into the distal forearm, staying ulnar to the palmaris longus so as to avoid damage to the palmar cutaneous branch of the median nerve (TECH FIG 1A).The exposure is deepened distally until the palmar fascia is encountered (TECH FIG 1B). This fascia is incised longitudinally just radial to the hamate hook. Dissection distal to the level of the hamate hook must be performed very carefully, as the ulnar neurovascular bundle is in this region.The transverse carpal ligament is opened longitudinally, staying just radial to the hamate hook and again being very cautious at the distal aspect of the exposure.The incision is continued proximally, releasing the distal volar forearm fascia, again staying ulnar to the palmaris longus.The contents of the carpal canal are now visualized (TECH FIG 1C).The digital flexors and median nerve are gently and bluntly retracted radially, revealing the floor of the canal that overlies the volar carpus (TECH FIG 1D).The volar capsule of the wrist joint is incised longitudinally, providing exposure of the volar carpus and radiocarpal joint.
REDUCTION AND FIXATION




TECH FIG 1 • Fixation of lunate palmar lip fractures. A. Carpal tunnel approach. The incision can be continued into the distal forearm, staying ulnar to the palmaris longus to avoid damage to the palmar cutaneous branch of the median nerve. B. Palmar fascia and antebrachial fascia exposed. C. Transverse carpal ligament released from hamate hook. D. Volar wrist capsule exposed.

TECH FIG 2 • Palmar lunate lip exposed and instrumented.
Open Reduction and Internal Fixation of Triquetral Fractures Excision or Open Reduction and Internal Fixation of Pisiform Fractures
HOOK OF HAMATE EXCISION
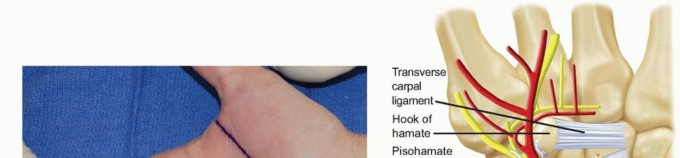
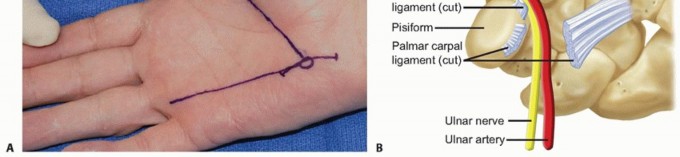
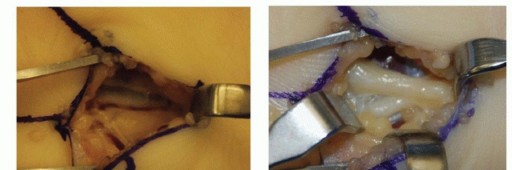
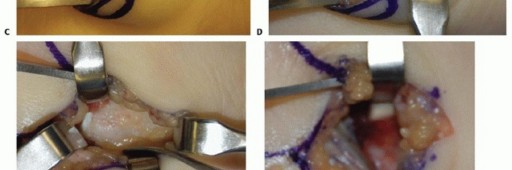
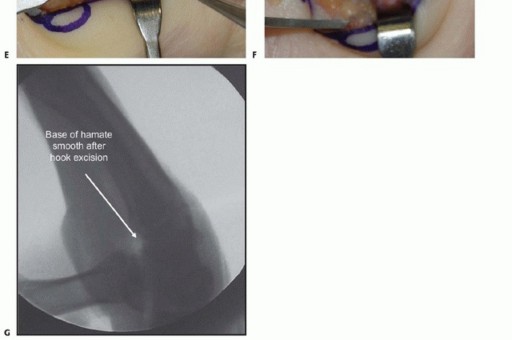
TECH FIG 3 •(continued)C. The ulnar artery is encountered first, volar and radial to the ulnar nerve. D. With the artery retracted ulnarly, the common digital nerve to the fourth web space and the small digit ulnar sensory nerve are visualized. The deep motor branch and the hypothenar motor branch have already been given off. E. The hamate hook is subperiosteally exposed and its margins are palpated with an elevator. The deep motor branch curves radially, closely associated with the distal surface of the hook. F. Care is also taken to protect the flexor tendons during exposure and resection, seen here on the radial margin of the hook. G. Fluoroscopy after hook excision can be helpful to ensure that the hook has been removed in its entirety and that no significant prominences remain.




TECH FIG 4 • Fixation of hamate dorsal shear fractures. A. Dorsal curvilinear incision centered on ring finger-small finger CMC joint. B. Extensor tendons exposed. C. Ring finger-small finger CMC joint exposed. D. Dorsal hamate reduced and instrumented.(continued)
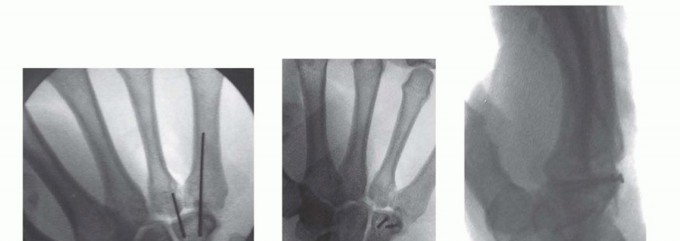
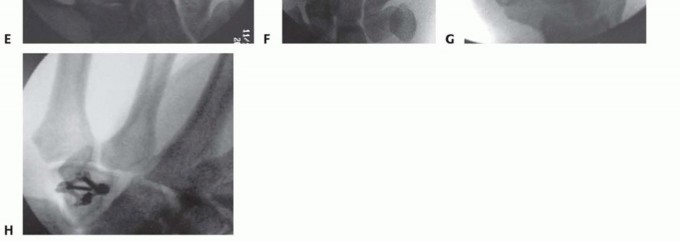
TECH FIG 4 •(continued)E. Temporary Kirschner wire. F,G. Screw fixation. H. Plate fixation.
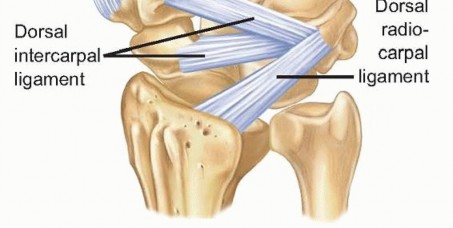
TECH FIG 5 • Dorsal intercarpal ligament anatomy.
TECH FIG 6 • ORIF of a trapezial body fracture. Isolated trapezial ridge fractures and nonunions are best approached using the FCR approach centered on the scaphotrapezial joint, with retraction of the FCR ulnarly or radially out of its trapezial groove to gain access to the ridge. The Wagner approach is also effective.For the Wagner approach, an incision is made along the radial border of the thumb metacarpal at the glabrous skin border.At the distal volar wrist crease, the incision is continued ulnarly to the level of the FCR tendon.Superficial radial sensory nerve and lateral antebrachial cutaneous nerve branches may be encountered and should be carefully preserved.The thenar musculature is elevated in a radial to ulnar direction off the thumb metacarpal base.Once the FCR tendon sheath is reached, it is incised longitudinally and the tendon is retracted ulnarly if necessary.The capsule overlying the trapeziometacarpal and scaphotrapezial joints is opened and the joints are visualized.The entire length of the trapezium may be exposed if needed, but we avoid excessive subperiosteal dissection, doing so only where necessary for accurate fracture reduction.Extensive exposure may result in delayed union or nonunion.At this point, internal fixation is performed if technically feasible, usually using lag screw fixation. The capsule is carefully reapproximated, and the subcutaneous tissues and skin are closed.
PEARLS AND PITFALLS
P.379Carpalinstability1. Be aware of the carpal instability patterns that can accompany these fracturesand treat accordingly.2. Failure to recognize an associated carpal instability pattern can lead to progressive carpal collapse and degeneration.Fracture ▪ Preoperative imaging is critical so that all fractures that require stabilization areidentification identified; consider CT scanning if plain radiographs are insufficient.1. Failing to identify all unstable fractures before or during surgery can necessitate a return to the operating room.Screw size1. Use small interfragmentary screws or even small plates for fracture fixationwhenever possible to decrease chances for hardware migration and to increase stability and possibly allow earlier range of motion.Excisionversus fixation1. We recommend hamate hook excision as opposed to fixation due to the minimal,if any, added benefit with fixation and the concern for significant nerve and tendon injuries with internal fixation.Futuresurgery1. Be sure the patient is aware of the possible need for further surgery in the future,such as for hamate hook excision, addressing capitate avascular necrosis, excisional arthroplasty or arthrodesis for posttraumatic articular degeneration of any joints involved with the initial trauma, and so forth.
POSTOPERATIVE CARE
Patients are placed in a well-padded volar plaster wrist splint postoperatively.The digits, including the metacarpophalangeal (MCP) joints, are left free unless there is some contraindication, such as a dorsal hamate fracture with CMC dislocation, which may require inclusion of MCP joints.If there is no contraindication, we encourage early digital range of motion and elevation. Following ORIF of a trapezial fracture, a short-arm thumb spica splint is applied.One to 2 weeks postoperatively, the patient is placed in a custom-fabricated splint (assuming there is noassociated carpal instability).If pins were used and are left outside of the skin, pin care is initiated at this time. Pins are usually removed 4 to 8 weeks postoperatively.In the case of a CMC joint fracture in which relatively large fracture fragments are anatomically stabilized with rigid internal fixation, near-immediate postoperative range of motion is initiated.For most other fractures, a total of about 6 weeks of wrist immobilization is followed by progressive range of motion.
OUTCOMES
Most isolated carpal bone body fractures unite, and it is generally thought that these patients do quite well with regard to symptomatic and functional recovery.The potentially symptomatic exceptions involving the hamate hook and trapezial ridge are easily treated by excision. Posttraumatic symptoms from other fractures, such as of the pisiform, trapezium, or triquetrum, may usually be addressed with isolated carpal bone excision with or without reconstruction, depending on the bone in question and other soft tissue and ligamentous considerations. For those carpal bones that cannot typically be simply excised, such as the hamate body and capitate, symptomatic posttraumatic changes may require partial or total wrist arthrodesis or other reconstructive options.Associated injuries are often the most problematic, and patients must understand the guarded prognosis for severe destabilizing carpal injuries.
COMPLICATIONS
Those complications common to all surgical procedures may occur, including but not limited to bleeding, infection, damage to structures, failure of surgery, potential need for more surgery, and untoward effects of anesthesia.Patients must also understand the relative severity of their injuries and risk for pain, stiffness, and loss of function.Capitate neck fractures are sometimes associated with nonunion or delayed union (up to 50% or more of isolated fractures) and may be analogous to scaphoid proximal pole fractures.Treatment of such nonunions is similar for both entities.Although rare, avascular necrosis of the capitate head may follow a capitate neck fracture that disrupts the vascular supply.The capitate head may be excised with or without interpositional arthroplasty if attaining union is not likely because of avascularity or other issues.Intra-articular fractures of the carpal bones are often complicated by posttraumatic arthritis. When symptomatic, treatment with traditional arthritis remedies, such as activity modification, anti-inflammatory medications, immobilization, or steroid injection, can be tried. If these fail to relieve the patient's symptoms to his or her satisfaction, the patient may elect to proceed with partial or total wrist arthrodesis, partial carpectomy, whether of the proximal row or otherwise, or selective arthroplasties as indicated.
SUGGESTED READINGS
- Adler JB, Shaftan GW. Fractures of the capitate. J Bone Joint Surg Am 1962;44-A:1537-1547.
- Amadio PC, Moran SL. Fractures of the carpal bones. In: Green DP, Hotchkiss DP, Pederson RN, et al, eds. Operative Hand Surgery, ed 5. Philadelphia: Elsevier, 2005;771-768.
- Cohen MS. Fractures of the carpal bones. Hand Clin 1997;13:587-599.
- Gelberman RH, Gross MS. The vascularity of the wrist: identification of arterial patterns at risk. Clin Orthop Relat Res 1986;(202):40-49.
- Hoppenfeld S, deBoer P. Surgical Exposures in Orthopaedics: The Anatomic Approach, ed 2. Philadelphia: Lippincott Williams & Wilkins, 1994.
- Vigler M, Aviles A, Lee SK. Carpal fractures excluding the scaphoid. Hand Clin 2006;22:501-516.
- Yu HL, Chase RA, Strauch B. Atlas of Hand Anatomy and Clinical Implications. St. Louis: Mosby, 2004.
