INTRODUCTION TO SPINAL TUBERCULOSIS SURGERY
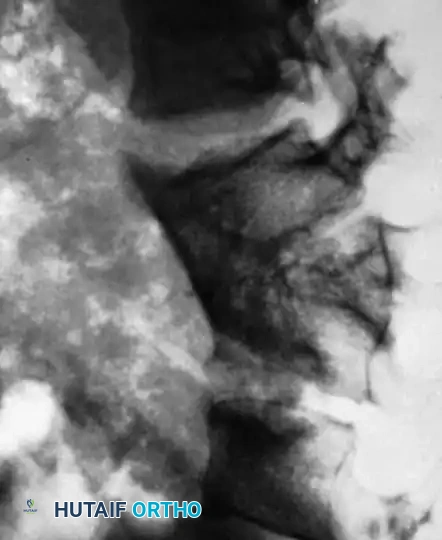
Tuberculosis of the spine, historically known as Pott’s disease, remains a formidable orthopedic challenge characterized by insidious destruction of the anterior vertebral column. The Mycobacterium tuberculosis bacillus exhibits a strong tropism for the vertebral body and intervertebral disc, leading to caseous necrosis, cold abscess formation, and progressive structural collapse. This anterior column failure inevitably results in a characteristic kyphotic deformity and, in severe cases, Pott’s paraplegia due to mechanical compression or epidural abscess extension.
While modern antitubercular therapy (ATT) is the cornerstone of treatment, surgical intervention is strictly indicated in the presence of progressive neurologic deficit, severe or worsening kyphotic deformity, massive paraspinal abscesses, pan-vertebral destruction, or clinical failure of medical management. The gold standard of surgical care, pioneered by Hodgson et al., relies on the principles of radical anterior débridement and structural arthrodesis.
Clinical Pearl: The anterior approach is biomechanically and pathologically superior for spinal tuberculosis. Because the disease primarily obliterates the anterior load-bearing column, posterior laminectomy alone is contraindicated; it destabilizes the spine further without addressing the ventral pathology, accelerating kyphotic collapse and neurologic deterioration.
TECHNIQUE 40-11: RADICAL DÉBRIDEMENT AND ARTHRODESIS (HODGSON ET AL.)
The surgical approach to the tuberculous spine is dictated entirely by the anatomic level of the lesion. The goal is to achieve direct, unhindered access to the anterior vertebral bodies to facilitate complete evacuation of the cold abscess, radical corpectomy of the diseased segments, and precise placement of a structural strut graft.
Upper Cervical Spine (C1–C2)
Approaching the atlantoaxial region requires meticulous airway management and precise soft-tissue handling. The upper cervical spine can be accessed via the transoral or transthyrohyoid approach.
Surgical Warning: In either approach, a preoperative tracheostomy is mandatory. Anesthesia must be administered through the tracheostomy to leave the pharynx completely free of endotracheal tubing, which would otherwise obstruct the surgical field. Furthermore, postoperative pharyngeal edema can rapidly compromise the airway if a tracheostomy is not in place.
The Transoral Approach:
* Position the patient with the head in hyperextension.
* Thoroughly pack the hypopharynx to prevent aspiration of blood and debris.
* Incise and turn back the soft palate on itself, anchoring it with heavy stay sutures to fully expose the nasopharynx.
* Palpate the anterior tubercle of the atlas. Make a 5 cm midline incision in the posterior pharyngeal wall, centered one fingerbreadth inferior to the anterior tubercle. Carry this incision directly down to the bone.
* Subperiosteally strip the posterior pharyngeal wall laterally to the margins of the lateral masses of C1 and C2.
* Retract the raised soft-tissue flaps with long stay sutures and control osseous oozing with packing. The anterior arch of the atlas, the body of the axis, and the bilateral atlantoaxial joints are now exposed for debridement.
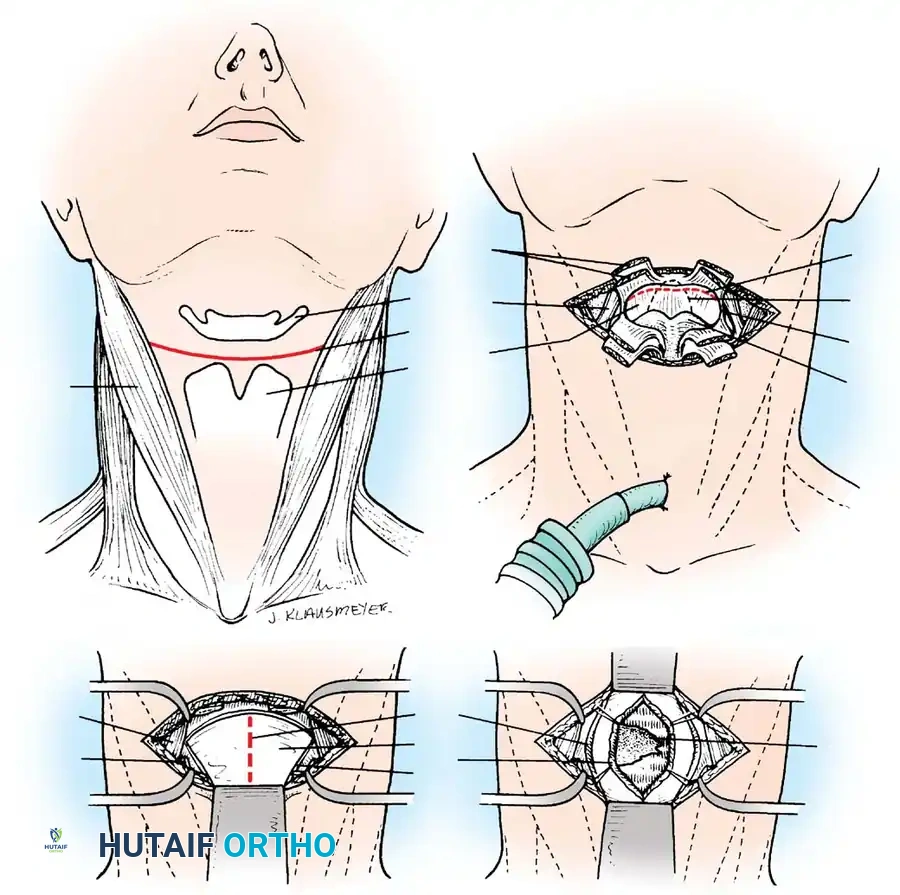
The Transthyrohyoid Approach:
* Make a transverse collar incision along the uppermost crease of the neck, between the hyoid bone and the thyroid cartilage, extending laterally to the carotid sheaths.
* Divide the sternohyoid and thyrohyoid muscles to expose the underlying thyrohyoid membrane.
* Detach the thyrohyoid membrane as close to the hyoid bone as possible. This superior detachment is critical to avoid iatrogenic injury to the internal laryngeal nerve and superior laryngeal vessels, which pierce the membrane near its inferior attachment.
* Enter the hypopharynx by incising the exposed mucous membrane from the lateral aspect to avoid damaging the epiglottis.
* Retract the hyoid bone superiorly and the epiglottis anteriorly. Make a midline incision through the posterior pharyngeal wall down to the bone.
* Raise subperiosteal flaps bilaterally to expose the bodies of C2, C3, and C4.
Lower Cervical (C3–C7) and Upper Thoracic Spine (C7–T3)
- C3–C7: Approach the lower cervical vertebrae through a standard anterior collar incision or a longitudinal incision along the anterior or posterior border of the sternocleidomastoid (SCM) muscle. Longitudinally incise the prevertebral fascia and the abscess wall to expose the diseased spine.
- C7–T3 (Cervicothoracic Junction): This transitional zone is notoriously difficult to access. Approach the spine on the side with the larger paraspinal abscess using a periscapular incision, identical to the exposure used for a first-stage thoracoplasty. Elevate the scapula with a mechanical retractor and resect the third rib. While the pleura is usually opened, an extrapleural approach should be utilized if dense adhesions are present. Ligate and divide the superior intercostal artery and vein at their origins.
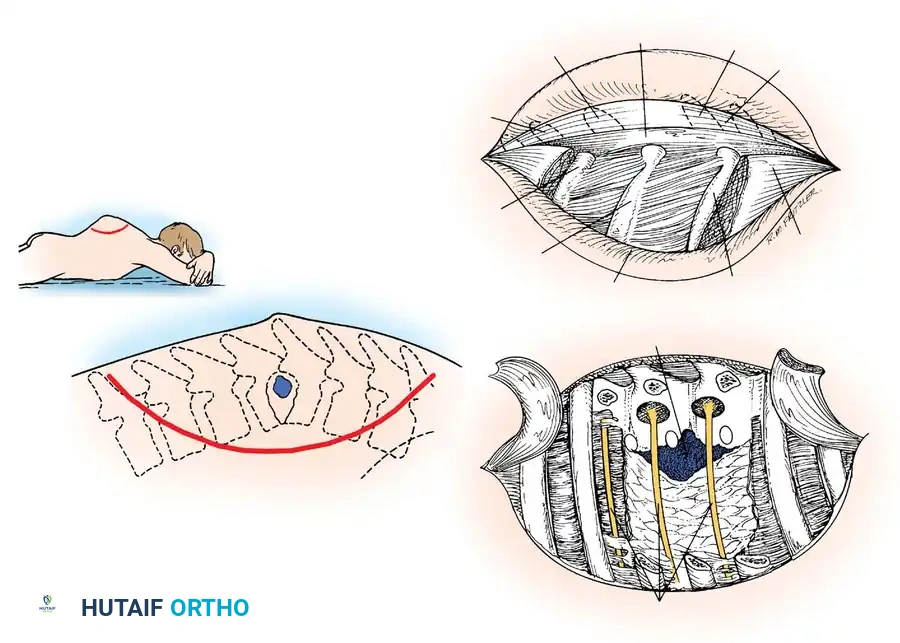
Midthoracic Spine (T4–T11)
The midthoracic spine is best approached via a standard thoracotomy, typically from the left side to avoid the liver and to work adjacent to the easily mobilized aorta rather than the thin-walled, easily torn inferior vena cava.
- Select the rib that lies in the midaxillary line directly opposite the maximal convexity of the kyphos. This is generally two ribs superior to the center of the vertebral focus.
- Make an incision along the selected rib, resect it subperiosteally, and enter the thoracic cavity.
- The tuberculous abscess is usually immediately visible, though dense adhesions between the parietal pleura and the lung may require careful sharp dissection. Mobilize the lung and retract it anteriorly.
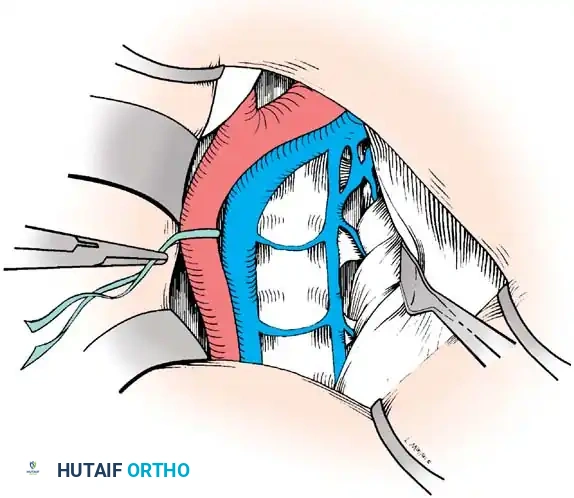
- Make a longitudinal incision in the pleura in the groove between the descending aorta and the abscess wall.
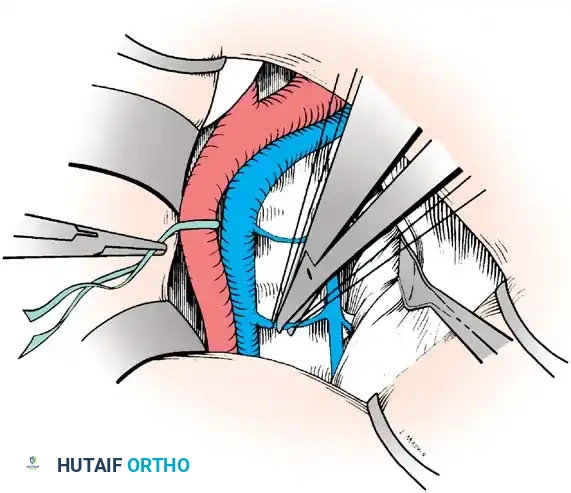
- Carefully displace the aorta anteriorly and medially. This maneuver reveals the segmental intercostal vessels. Securely ligate and divide these vessels across the entire length of the abscess cavity to allow further mobilization of the aorta away from the spine.
- Divide the overlying elements of the splanchnic nerves.
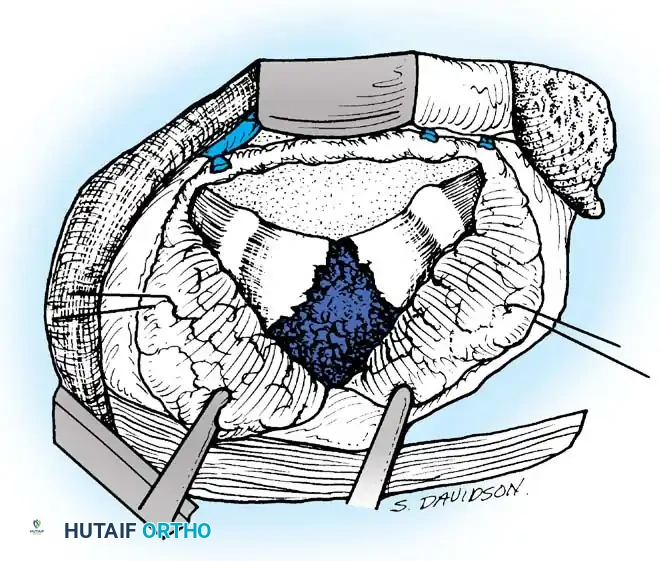
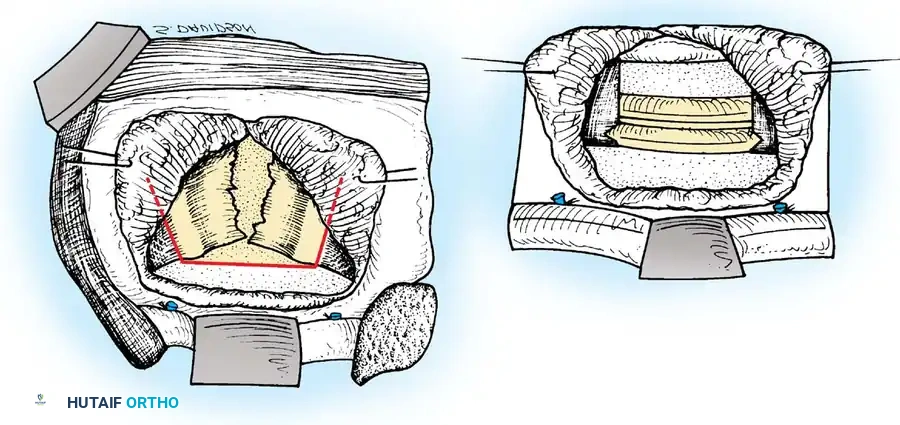
- Palpate the extent of the abscess across the anterior vertebral bodies. Make a T-shaped incision through the thick abscess wall: the transverse limb should be opposite the center of the disease, and the longitudinal limb medial to the ligated intercostal vessels.
- Raise the two triangular flaps to reveal the caseous necrotic core and the destroyed vertebral bodies.
Thoracolumbar (T12–L2) and Lower Lumbar Spine (L3–L4)
- T12–L2: Approach this region through an incision over the left 11th rib. Maintain an extrapleural and retroperitoneal dissection plane. Detach the crus of the diaphragm from the spine. Divide the psoas muscle transversely and reflect it distally. Ligate the lumbar segmental arteries and veins similarly to the thoracic intercostals.
- L3–L4: Utilize a standard renal approach via a left 12th rib incision. The psoas muscle is divided transversely at a more distal level.
Pitfall: Tuberculous abscesses frequently track down the psoas sheath (psoas abscess). When dissecting through the ill-defined, inflamed muscle fibers, exercise extreme caution to avoid injuring the trunks of the lumbar plexus, which lie immediately posterior to the psoas muscle belly.
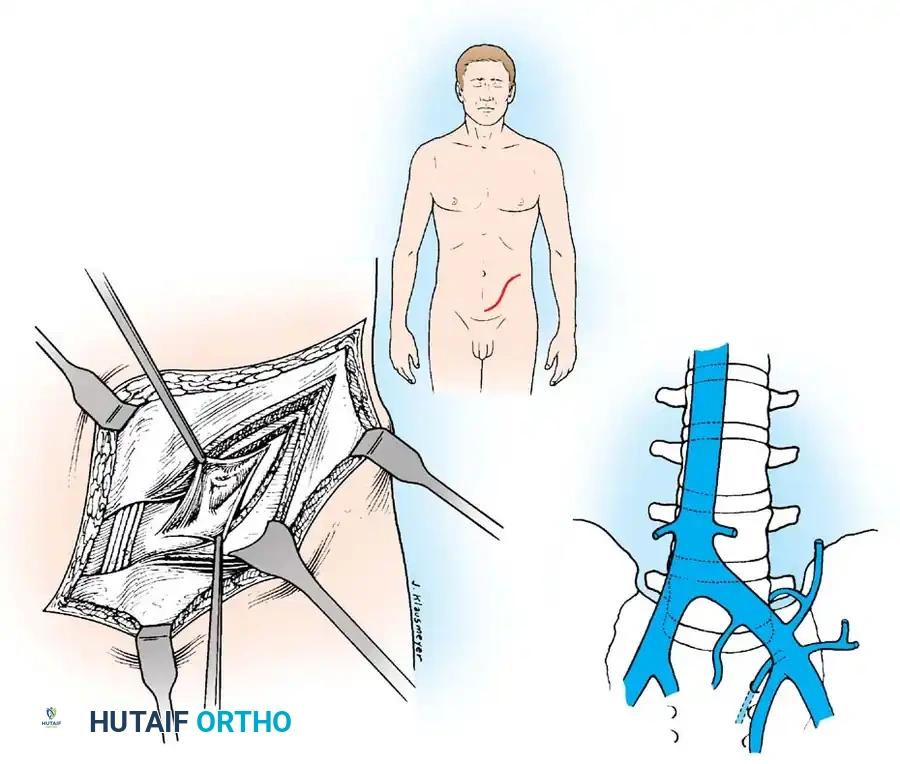
Lumbosacral Junction (L5–S1)
Expose the L5 and S1 vertebrae through an extraperitoneal approach.
* Make a "lazy-S" incision starting in the midline (midway between the symphysis pubis and the umbilicus) and curving laterally to a point midway between the iliac crest and the lowest rib.
* Divide the abdominal musculature (external oblique, internal oblique, transversus abdominis) in line with the incision.
* Sweep the peritoneum medially off the lateral abdominal wall, exposing the left psoas muscle and the lumbosacral spine.
Vascular Management at the Bifurcation:
The approach to the L5-S1 disc space is dictated by the anatomic level of the aortic bifurcation.
* High Bifurcation: The safest approach is directly between the common iliac vessels. The primary vessels encountered here are the middle sacral artery and vein, which must be cauterized and divided.
* Low Bifurcation: The approach must be made lateral to the aorta, vena cava, and common iliac vessels. To safely mobilize the left common iliac vein to the right, you must meticulously isolate, ligate, and divide the iliolumbar and ascending lumbar veins. If a higher exposure is needed, ligate the 4th and 5th lumbar vessels.
EXCISION OF DISEASED TISSUE AND ANTERIOR ARTHRODESIS
Regardless of the spinal level, the principles of radical debridement and structural grafting remain uniform. The objective is to remove all infected, avascular tissue until healthy, bleeding cancellous bone is reached, providing a vascularized bed for the bone graft.
Radical Débridement (Corpectomy)
- Evacuate all liquid pus, caseous debris, and sequestrated bone or disc material using high-powered suction and pituitary rongeurs. If the abscess spans bilaterally, pass the suction tip anterior to the vertebrae into the contralateral cavity to ensure complete evacuation.
- Using osteotomes, high-speed burrs, and rongeurs, radically excise all diseased, sclerotic, and necrotic bone.
- The excision must extend posteriorly to the posterior longitudinal ligament (PLL). Remove the PLL and any tuberculous granulation tissue to fully decompress the ventral dura.
- Crucial Step: Excise the entire affected vertebral body. Tuberculous collections and sequestrated disc fragments frequently hide in the spinal canal posterior to seemingly intact posterior vertebral body walls.
- Remove the intervertebral discs at the cranial and caudal extents of the cavity until normal, bleeding endplates are exposed.
Structural Arthrodesis
- Attempt partial correction of the kyphotic deformity by applying direct posterior pressure on the spine (often done by the anesthesia team or via positioning).
- Cut a deep, precise mortise (keyhole) into the healthy vertebral bodies at both the superior and inferior ends of the defect.
- Measure the defect and insert one or more structural strut grafts. The grafts must be slightly oversized to keep the vertebrae "sprung apart" under compression, ensuring immediate biomechanical stability and preventing graft dislodgment.
Graft Selection:
* Thoracic Spine: Fashion strut grafts from the rib resected during the thoracotomy. Supplemental bone bank allograft may be added.
* Cervical Spine: Utilize tricortical iliac crest autograft or structural allograft.
* Lumbar Spine: Due to high compressive loads, a massive structural graft from the anterior or posterior iliac crest is mandatory.

Prior to closure, instill topical antitubercular agents (e.g., streptomycin and isoniazid powder) directly into the debrided cavity. Close the surgical site in standard layered fashion. For thoracic approaches, maintain closed suction drainage (chest tube) of the pleural space for 2 to 3 days.
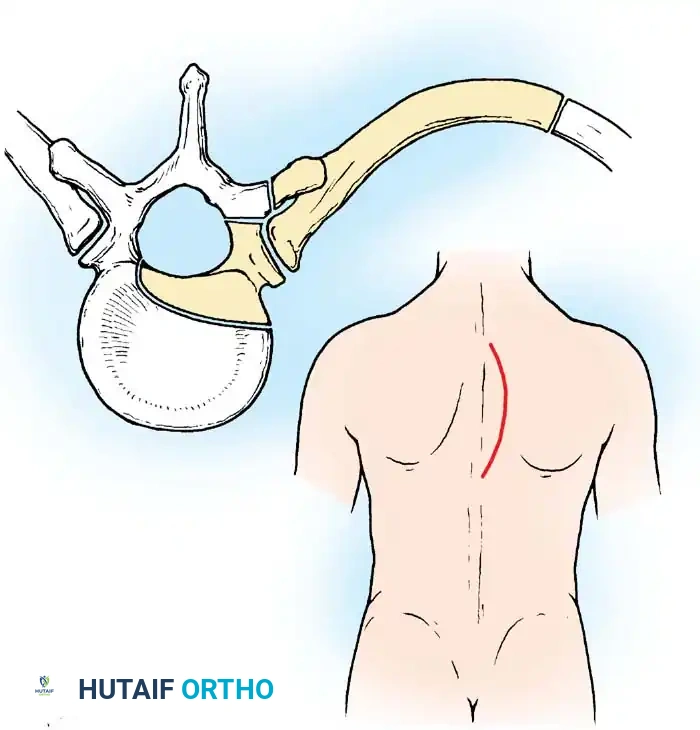
TECHNIQUE 40-12: DORSOLATERAL APPROACH TO THE DORSAL SPINE (ROAF ET AL.)
While the anterior approach is the gold standard, the dorsolateral approach is a highly effective alternative for the thoracic spine when a formal thoracotomy is contraindicated (e.g., severe pulmonary compromise) or when posterior drainage of a massive abscess is preferred.
Surgical Steps for the Dorsolateral Approach
- Select the side with the larger paraspinal abscess shadow on preoperative imaging. If symmetric, default to the left side.
- Make a large, curved incision. Begin posteriorly 3.8 cm from the midline and 7.5 cm proximal to the center of the lesion. Curve the incision distally and laterally to a point 12.5 cm from the midline at the apex of the lesion, then curve it back medially to end 3.8 cm from the midline and 7.5 cm distal to the lesion.
- Divide the superficial fascia, deep fascia, and paraspinal musculature down to the ribs. Retract the large myocutaneous flap medially.
- Identify the rib corresponding to the center of the tuberculous focus. You must resect 7.5 to 10 cm of this rib, as well as the ribs immediately proximal and distal to it (three ribs total).
- Free the ribs subperiosteally and divide them with rib shears laterally. Medially, disarticulate and resect the ribs at the tips of the transverse processes.
- Under direct vision, divide the costotransverse ligaments and resect the transverse processes.
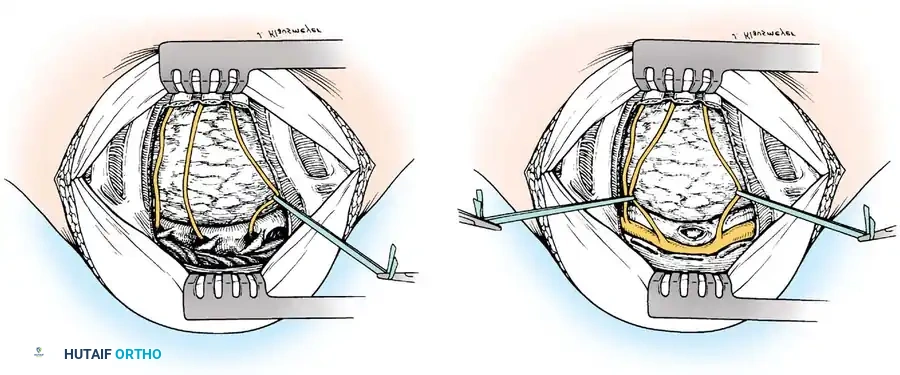
- Neural Identification: Identify two (preferably three) intercostal nerves. Trace them medially into the intervertebral foramina. These nerves serve as critical anatomic landmarks, indicating the exact level of the spinal cord within the canal.
- Isolate the intercostal vessels near the vertebral column, clamp, ligate, and divide them.
- Divide the intercostal muscles near the spine.
- Using blunt dissection, carefully separate the parietal pleura from the lateral and anterolateral aspects of the vertebral bodies.
Surgical Warning: The pleura is often highly adherent and thickened due to the adjacent inflammatory process. Avoid perforating it. If an iatrogenic pleural tear occurs, it must be sutured immediately and a chest tube considered.
- Pass a finger into the wound, sweeping anterior to the vertebral bodies to locate the center of the lesion. Perform a thorough evacuation of all pus, granulation tissue, and necrotic bone.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The success of spinal tuberculosis surgery relies as much on rigorous postoperative immobilization and medical management as it does on surgical execution.
- Immobilization: Historically, patients were placed in a custom-molded plaster cast consisting of anterior and posterior shells. In modern practice, a rigid Thoracolumbosacral Orthosis (TLSO) or Cervicothoracic Orthosis (CTO) is utilized. The patient must remain strictly immobilized until the strut graft has incorporated and the spine is judged to have united clinically and radiographically.
- Duration: The average time of rigid immobilization is approximately 3 months.
- Mobilization: After 3 months, mobilization is initiated gradually over a period of 6 to 8 weeks. During this phase, the patient must be monitored meticulously with serial upright radiographs to detect any graft subsidence, increasing kyphosis, or signs of recurrent disease activity.
- Medical Management: Surgery is an adjunct to, not a replacement for, medical therapy. Systemic multidrug antitubercular therapy (ATT) must be continued uninterrupted for a minimum of 9 to 18 months postoperatively, guided by infectious disease consultation and inflammatory markers (ESR, CRP).
