DEFINITION AND PATHOGENESIS
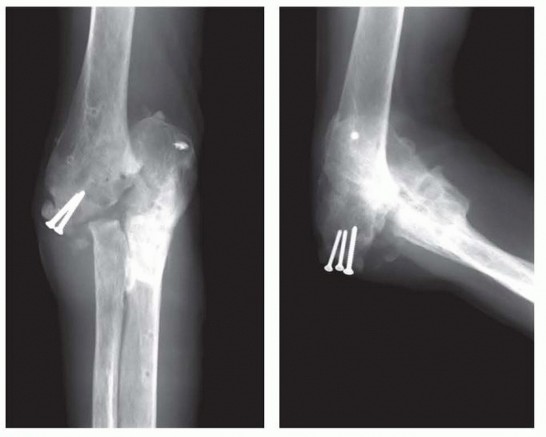
FIG 1 • Radiograph demonstrating dissociation of the forearm from the brachium after four attempts to manage a terrible triad injury. This degree of deformity was not considered amenable to interposition; a total elbow was performed despite the patient's high level of activity.
PATIENT HISTORY AND PHYSICAL FINDINGS
PATIENT HISTORY
The patient history is directed at gaining information about the initial injury, treatments undertaken, complications of treatment, presenting complaints, and patient expectations.Detailed investigation of the patient's symptoms should include questions regarding the degree of pain, presence of instability or stiffness, and mechanical symptoms of catching or locking.Presence of radiating pain especially in the ulnar nerve distribution is solicited.Special attention is paid to night pain and pain at rest, as these suggest a possibility of sepsis. Note: A historyof drainage or any evidence of infection is especially critical to elicit.
PHYSICAL EXAMINATION
Physical examination of the elbow should follow a systematic approach.Inspection of the elbowEspecially for warmth and rednessPresence and location of previous skin incisions or persistent wounds Alignment of the extremity at restProminent hardware Range of motionLocalization of pain during active and passive motionActive range of motion (AROM) is assessed and compared to the opposite side. The degree of motion, smoothness of motion, and feel of the end point is established.Normal AROM varies but should be symmetric with the opposite unaffected side.Range of motion should be from near full extension (may have hyperextension) to 130 to 140 degrees of flexion.Normal forearm rotation is an arc of 170 degrees, with slightly more supination than pronation. Functional range of motion has been defined as a flexion-extension arc from 30 to 130 degrees and a pronation-supination arc from 50 degrees of pronation to 50 degrees of supination.10Passive range of motion (PROM) is then assessed and compared to the active motion arc.Palpation of the elbowShould systematically review all of the bony and soft tissue structures of the elbowP.941The ulnar nerve needs to be carefully assessed. If previously surgically manipulated, its location should be identified if possible.Examine for the presence of Tinel sign.Motor function of the elbow should be assessed. In particular, the flexor (biceps and brachialis) and extensor (triceps) function should be evaluated.
IMAGING AND OTHER DIAGNOSTIC STUDIES
PLAIN X-RAYS
Orthogonal views of the elbow are mandatory.A good lateral radiograph can typically be obtained.A useful anteroposterior (AP) radiograph can be difficult to obtain, particularly if the patient has a significant flexion contracture.Note: If difficulty is encountered, use fluoroscopic guidance to obtain proper orientation.Oblique radiographs can be helpful in obtaining more detail.
ADVANCED IMAGING
Computed tomography (CT) scanCT scans are particularly helpful in assessing the integrity of the bone and establishing whether the joint space is reasonably preserved.Three-dimensional reconstructions provide a better understanding of complex osseous injuries (FIG 2).Magnetic resonance imaging (MRI)MRI is rarely needed in the assessment of a posttraumatic joint and is therefore used sparingly. May be helpful to assess suspicious and atypical soft tissue deformity or swelling
DIFFERENTIAL DIAGNOSIS
Nonunion/malunion of the distal humerus Posttraumatic stiffness of the elbow Chronic dislocation of the elbow
NONOPERATIVE MANAGEMENT
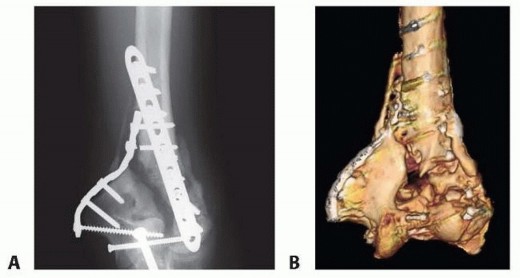
FIG 2 • A. Complex injury with unclear joint pathology or state of healing. B. The 3-D reconstruction clarifies the extent of the problem. Maintain range of motion of the elbow. Aggressive efforts to regain lost motion can inflame and thus aggravate the joint.External bracing is occasionally used to support an unstable extremity. However, in general, bracing is poorly tolerated and functionally limiting.
SURGICAL MANAGEMENT
Surgical management is directed at addressing the underlying cause of disability, taking into consideration thepatients age, pathology, physical requirements, and expectations.
INDICATIONS
Age and functional need prompt consideration of this intervention. Age is a surrogate for activity.In general, patients younger than age 55 years are always candidates for interposition—all else being equal.Those older than age 70 years with similar pathology are usually better candidates for replacement.Patients with pain and/or loss of range of motion who have failed nonoperative managementPosttraumatic arthritis in patients who are either too young for total elbow arthroplasty (TEA) or who are unwilling to accept the functional restrictions with TEAThe patients who do best following interposition are those with painful loss of motion when there is no requirement for aggressive, heavy use of the extremity.
CONTRAINDICATIONS
Active or subacute infection (septic arthritis with persistent infection)8 Grossly unstable elbowMarked angular deformity (exceeding 15 degrees) Inadequate bone stockPatients unable or unwilling to follow postoperative instructions Inexperience with the techniquePain at rest or pain without associated functional loss (relative contraindication)
PREOPERATIVE PLANNING
Graft optionsAllograft Achilles tendon7: has the advantage of no donor site morbidityThe abundance of the tissue allows for variable thickness depending on reconstructive need. Can also be used to reconstruct the collateral ligaments if necessaryAutogenous dermis or fascia lataBest used for limited applications (eg capitellum) Allograft dermal tissueAn articulated (hinged) external fixator must be available.
PATIENT POSITIONING

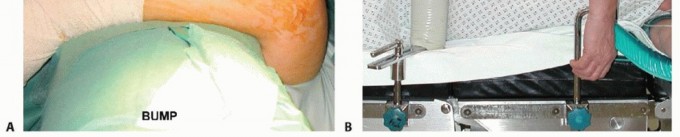
FIG 3 • A. Patient is placed in the supine position and the arm is brought across the chest and is supported with a bolster. B. Alternative lateral decubitus position with the arm maintained over an arm support.
TECHNIQUES
Interposition Arthroplasty
INTERPOSITION ARTHROPLASTY
SURGICAL TECHNIQUE2,7,8****


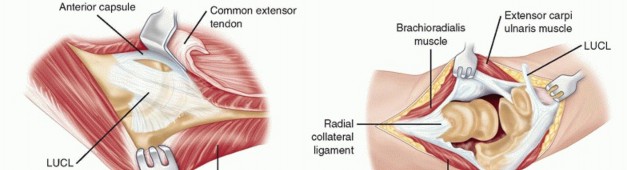
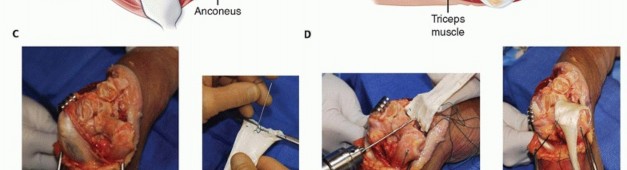
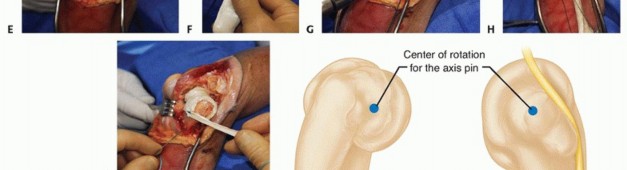
TECH FIG 1 •(continued)C. The anconeus and triceps are elevated off of the posterolateral capsule whereas the common extensor group is elevated off of the anterior capsule. Exposure can be expanded posteriorly with partial release of the triceps from the lateral aspect of the olecranon. D. Deep extensile exposure requires release of the lateral collateral ligament and anterior and posterior capsule. E. The released lateral margin of the triceps attachment is retracted. With flexion and supination, the joint is exposed. F. The interposition membrane is prepared with mattress sutures placed distally. The Achilles tendon allograft also permits reconstruction of the collateral ligaments if necessary. G. Drill holes are placed from posterior to anterior across the supracondylar region to align with the graft as much as possible. H. The interposition membrane is secured to the distal humerus. I. If necessary the graft can be fashioned to reconstruct the collateral ligaments. J. Drawing demonstrating the center of rotation on the lateral and medial side of the elbow. K. A stylus is impacted into the axis of rotation using the axis target guide.(continued) P.944Four nonabsorbable no. 1 sutures are placed in the graft.Note: If the Achilles is used, care is taken to ensure the rough side is applied to the humerus and the smooth side exposed to articulate with the ulna.Typically, four drill holes are placed across the supracondylar region from posterior to anterior (TECH FIG 1G). These drill holes are placed at the medial aspect of the trochlea, above the trochlear sulcus, at the lateral margin of the trochlea, and at the lateral aspect of the capitellum.Note: Care is taken to align the drill holes with the sutures placed in the graft.The interposition tissue is then draped over the distal humerus and secured with sutures drawn through the drill holes from anterior to posterior. They are passed through the graft posteriorly in a manner to tightly apply the graft to the distal humerus and tied (TECH FIG 1H). The medial and lateral sutures are first secured, followed by the middle two, through the graft from front to back. If there is collateral ligament insufficiency, the tails of graft (especially when using Achilles tendon) can be fashioned to reconstruct the collateral ligaments (TECH FIG 1I).The radial head is left intact, especially if medial collateral ligament reconstruction is performed, in order to contribute to the valgus stability of the elbow.The lateral collateral ligament is repaired through drill holes at the center of rotation laterally. The ligament is not tied until the external fixator is securely applied.
HINGED ELBOW EXTERNAL FIXATOR
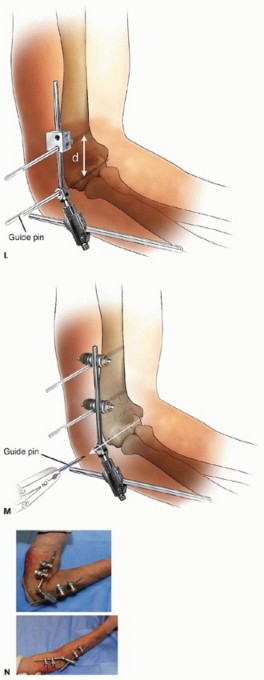
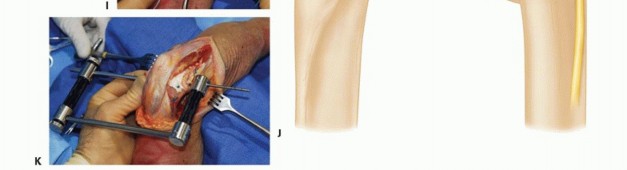
TECH FIG 1•(continued)L.The distal humeral pin is placed less than one humeral width dimension proximal to the axis to avoid injury to the radial nerve.M.Once the humeral pins are secured, the axis pin is removed.N.When properly applied, a markedly functional extension (top) and flexion (bottom) arc is possible.P.945PEARLS AND PITFALLS
|Indications ▪ Interposition arthroplasty is considered in patients with a stable elbow and a limited, painful range of motion.1. TEA is considered in carefully selected patients where other nonoperative|Interpositionarthroplasty1. Predictors of poor outcome1. Painful, mobile elbow1. Preoperative instability1. Fixed deformity1. Need to reconstruct both the medial collateral ligament and lateral ulnarcollateral ligament at the time of interposition1. Maintain the fixator for 3-4 weeks (do not exceed 6 weeks).1. Meticulous pin care is required.1. Regardless of the treatment undertaken, the goal of treatment is a pain-free, functional arc of motion.Goals oftreatmentand operative measures have been exhausted.
POSTOPERATIVE MANAGEMENT
Range of motion is started as quickly as allowed by the condition of the soft tissues. In general, immediate motion is preferred. However, the prerequisite is a quiet soft tissue envelope. Range of motion may be assisted with a continuous passive motion machine if desired.Patients are taught pin care that is performed daily at home.Patients are seen at 10 to 14 days postoperatively for staple removal and wound check and every 2 weeks thereafter until pin removal.The external fixator is left in place for approximately 3 to 4 weeks and then removed in the operating room (OR) with assessment of elbow stability and motion under anesthesia.Note: At the time of pin removal, access the elbow for stability and smoothness of the flexion arc. We then stretch the arc to regain the flexion and extension arc obtained at the time of surgery.Rehabilitation is continued with concentration on obtaining a functional range of motion.
OUTCOMES
The most predictable results for interposition occur in patients presenting with the following2,7,8,9,12: Stiffness and pain preoperativelyStable elbowOne or no ligament reconstruction required at surgery Less than 15 degrees of angular deformity preoperativelyPoor results noted whenPain, especially pain at rest, is the only presenting complaint Unstable elbowNeed to reconstruct both the medial and lateral collateral ligaments at the time of interposition Fixed angular deformity exceeding 15 degrees; rotatory deformityMost studies report 70% satisfaction rate among patients with respect to pain relief, and 80% of patients regain a functional range of motion.9Cheng and Morrey2 found 67% of patients treated for rheumatoid arthritis (RA) had satisfactory relief of pain and 75% of patients treated for osteoarthritis (OA) were satisfied at 5-year follow-up. Those with functional arcs of motion did less well than the stiff joint.Larson and Morrey7 reported 88% of patients would repeat the procedure with a mean surveillance of 8 years.
COMPLICATIONS
Complications of interposition arthroplasty include the following: InstabilityInfectionUlnar neuropathy Resorptive bone loss Heterotopic bone formationComplications related to the external fixator include the following3: Superficial pin tract infectionsDeep infection (osteomyelitis)Pin breakageNote: Complications with external fixators are statistically correlated to prolonged period of application.3Complications for the overall procedure have been reported to occur in up to 25% of patients.7,9
REVISION
The salvage for a failed interposition arthroplasty is a TEA.1Interposition arthroplasty should not be undertaken unless the surgeon is comfortable performing a total elbow replacement in the face of failure.
REFERENCES
- Blaine TA, Adams R, Morrey BF. Total elbow arthroplasty after interposition arthroplasty for elbow arthritis. J Bone Joint Surg Am 2005;87(2):286-292.
- Cheng SL, Morrey BF. Treatment of the mobile, painful arthritic elbow by distraction interposition arthroplasty. J Bone Joint Surg Br 2000;82(2):233-238.
- Cheung EV, O'Driscoll SW, Morrey BF. Complications of hinged external fixators of the elbow. J Shoulder Elbow Surg 2008;17(3):447-453.
- Cobb TK, Morrey BF. Use of distraction arthroplasty in unstable fracture dislocations of the elbow. Clin Orthop Relat Res 1995;(312): 201-210.P.946
- Kamineni S, Ankem H, Patten DK. Anatomic relationship of the radial nerve to the elbow joint: clinical implications of safe pin placement. Clin Anat 2009;22(6):684-688.
- Kamineni S, Hirahara H, Neale P, et al. Effectiveness of the lateral unilateral dynamic external fixator after elbow ligament injury. J Bone Joint Surg Am 2007;89(8):1802-1809.
- Larson AN, Morrey BF. Interposition arthroplasty with an Achilles tendon allograft as a salvage procedure for the elbow. J Bone Joint Surg Am 2008;90(12):2714-2723.
- Morrey BF. Interposition arthroplasty. In: Morrey BF, Sanchez-Sotelo J, eds. The Elbow and Its Disorders, ed 4. Philadelphia: Saunders Elsevier, 2009:935-948.
- Morrey BF. Post-traumatic contracture of the elbow. Operative treatment, including distraction arthroplasty. J Bone Joint Surg Am 1990;72(4):601-618.
- Morrey BF, Askew LJ, Chao EY. A biomechanical study of normal functional elbow motion. J Bone Joint Surg Am 1981;63(6):872-877.
- Morrey BF, Morrey MC. Exposure of the elbow. In: Morrey BF, Morrey MC, eds. Masters Techniques in Orthopaedic Surgery: Relevant Surgical Exposures. Totowa, NJ: Lippincott Williams & Wilkins, 2008.
- Nolla J, Ring D, Lozano-Calderon S, et al. Interposition arthroplasty of the elbow with hinged external fixation for post-traumatic arthritis. J Shoulder Elbow Surg 2008;17(3):459-464.
