Surgical Correction of Juvenile Bunion ## DEFINITION Adolescent bunion is a multifactorial, complex deformity consisting of medial deviation of the first metatarsal (metatarsus primus varus), lateral deviation of the great toe through the firstmetatarsophalangeal joint (hallux valgus), and enlarged medial eminence of the distal first metatarsal. 2, 3, 4, 6Other findings include contracted lateral and lax medial soft tissues of the first metatarsophalangeal joint, lateral subluxation of the sesamoids, pronation of the great toe, plantar subluxation of the abductor hallucis muscle, and generalized ligamentous laxity, flexible pes planus, and gastrocnemius contracture. ## ANATOMY Metatarsus primus varus resulting in increased intermetatarsal (IM) angle 2, 3Obliquity of the medial cuneiform-first metatarsal joint 2, 3Medial prominence of the first metatarsal headValgus angulation through the first metatarsophalangeal joint 2, 3 Minimal or no deformity through the first interphalangeal joint Lateral translation of sesamoidsPlantar-lateral positioning of the abductor hallucis with unopposed pull of the adductor hallucis muscle Lateral subluxation of the extensor hallucis longus and flexor hallucis longus tendonsPronation (internal rotation) of the first toe Differs from an adult bunionPhysis of the first metatarsal and proximal phalanx are located proximally (this limits ability to perform proximal osteotomies in skeletally immature patients).The first metatarsophalangeal joint does not have osteoarthrosis.The medial eminence is less prominent in adolescent bunions than in adult bunions. ## PATHOGENESIS Multiple theories exist; it is difficult to differentiate primary findings from secondary ones. 2, 3, 6Extrinsic and intrinsic factors contribute to formation of adolescent bunions. IntrinsicMetatarsus primus varusObliquity of the medial cuneiform-first metatarsal joint Long first metatarsalLigamentous laxityHeel cord contracture causes foot pronation, which in turn places a valgus force on the hallux while walking ExtrinsicShoe wear, particularly those with a narrow toe and elevated heel ## NATURAL HISTORY Natural history is believed to be favorable. Most patients with adolescent bunions can be treated nonoperatively. 2, 5 ## PATIENT HISTORY AND PHYSICAL FINDINGS Patients typically present in late childhood or adolescence. 2, 3Complaints about appearance of footComplaints of pain over the medial exostosis or about the first metatarsophalangeal joint Pain is exacerbated by shoe wear.Complaints about finding shoes that are comfortable Physical examination 2, 3Areas of tenderness: first metatarsophalangeal joint, medial prominence Alignment when standing and walkingMobility of first metatarsophalangeal jointSkin condition: the clinician should search for calluses, areas of irritation Foot and ankle range of motionCareful neurologic examination ## IMAGING AND OTHER DIAGNOSTIC STUDIES Standing anteroposterior (AP), lateral, and oblique radiographs should be obtained if surgical correction is being contemplated. 1, 2Measurements on the AP radiograph 1, 2 ( FIG 1)IM angle: Normal is 9 degrees or less.IM angle usually is 12 to 18 degrees in adolescent bunion.Hallux valgus angle: Normal is 16 degrees or less.Less than 25 degrees indicates mild deformity. Twenty-five to 40 degrees is moderate deformity. More than 40 degrees is severe.Most adolescent bunions are mild to moderate.Distal metatarsal articular angle: Normal is 15 degrees or less.Proximal phalangeal articular angle: Normal is 5 degrees of valgus. ## DIFFERENTIAL DIAGNOSIS Hallux valgus interphalangeus ## NONOPERATIVE MANAGEMENT Initial treatment is nonoperative. 2, 4Proper-fitting shoesAchilles tendon/calf muscle stretching if there is a heel cord/gastrocnemius contracture Orthotics may be useful when there is also ligamentous laxity and pes planus.
 ---
---
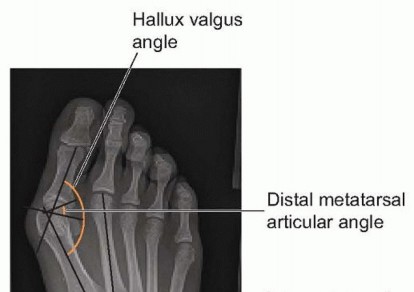
 ### FIG 1 • Measurements made on the AP radiograph.
### FIG 1 • Measurements made on the AP radiograph.
SURGICAL MANAGEMENT Surgery should be reserved for patients with persistent symptoms despite adequate nonoperative care. 2, 3, 4, 5Goals are to decrease pain and to restore the alignment of the first ray, with respect to both the second ray and the joints of the ray itself. 2, 3, 4, 5If feasible, surgery is delayed until early adolescence, as recurrence rates are higher in younger children.Patients and their families should be carefully counseled regarding postoperative expectations, particularly the risk of recurrence.The surgical plan needs to factor in the age of the patient and address the unique characteristics of each deformity.Multiple procedures have been described, including hemiepiphysiodesis of the lateral first metatarsal physis, distal osteotomies, scarf osteotomies, and proximal osteotomies. 2, 3, 4, 5For “typical” adolescent bunion (IM angle 12 to 18 degrees, hallux valgus angle <40 degrees), surgery generally consists of a distal soft tissue procedure, excision of the medial prominence, and corrective osteotomy.In older adolescents, where the physis of the first metatarsal is closed, the corrective osteotomy can be performed proximally.If the physis of the first metatarsal is open, a first metatarsal neck osteotomy has been described (Mitchell procedure). ## Preoperative Planning The surgeon should review the patient's radiographs to determine IM angle and hallux valgus angle. 2, 3, 4 ## Positioning The patient is positioned supine. A tourniquet is used. ## Approach A dorsomedial incision is made starting just distal to the first metatarsophalangeal joint and extending proximally for 5 to 6 cm.The surgeon should avoid injury to the dorsal medial sensory nerve. ## TECHNIQUES
-
Mitchell Bunionectomy (Stevens Modification)Expose the medial first metatarsophalangeal joint.Make a distally based Y-shaped incision in the capsule and periosteum. The stem of the Y is over the metatarsal, whereas the upper portion of the Y is formed distally.The joint and medial eminence are then exposed.A medial release of the first metatarsophalangeal joint is performed. Leave the lateral portion of the joint intact to avoid disrupting the blood supply to the head of the first metatarsal.The first cut involves removing the prominent medial eminence with an osteotome, starting distally at the sagittal groove (groove of Clark).The second cut is made at the distal metaphyseal-diaphyseal junction of the first metatarsal. This should be perpendicular to the shaft of the first metatarsal and extend two-thirds the width of the shaft of the first metatarsal ( TECH FIG 1A).The third, proximal cut is made about 2 to 3 mm proximal to the first cut and is created completely across the first metatarsal. The cut is oriented perpendicular to the shaft of the second metatarsal when viewed from the dorsum of the foot and is angled (when viewed from the medial aspect of the first metatarsal) to create a small plantar-based wedge ( TECH FIG 1B). This ensures that the distal fragment does not dorsiflex during reduction of the osteotomy.The interposed bone is removed.The osteotomy is reduced and pinned with two smooth 0.062-inch Kirschner wires ( TECH FIG 1C).The prominence of the distal portion of the metatarsal shaft is smoothed off with a rongeur, and a capsulorrhaphy is performed with absorbable sutures.Sterile dressings are applied, and the toe is splinted in neutral to slight plantarflexion. A short-leg cast is usually applied over the dressing for additional protection.
 ---
---

 TECH FIG 1 • A. Bone cuts required to perform a modified Mitchell osteotomy. The medial prominence isexcised first (
cut 1
). The first cut of the osteotomy is performed two-thirds of the way through the firstmetatarsal at the junction of the metaphysis and diaphysis and is oriented perpendicular to the long axis of the first metatarsal (
cut 2
). The second bone cut (
cut 3
) is made completely through the bone and completes the osteotomy. It should be made 2 to 4 mm proximal to the first cut and is perpendicular to the long axis of the second metatarsal. B. When seen from the medial side, the osteotomy should be oriented so that a small plantar-based wedge is produced. This helps avoid dorsiflexion of the distal fragment when the osteotomy is reduced. C,D. The osteotomy is reduced and stabilized with a 0.062-inch smooth Kirschner wire.Approach
1.
The surgeon should identify and protect the dorsal sensory nerve.Osteotomy
1.
The surgeon should avoid resecting more than about 3 mm of bone to preventshortening of the first metatarsal.Proximalosteotomy
1.
It should create a slight plantar-based wedge with the distal cut to avoiddorsiflexion of the osteotomy. ## PEARLS AND PITFALLS
TECH FIG 1 • A. Bone cuts required to perform a modified Mitchell osteotomy. The medial prominence isexcised first (
cut 1
). The first cut of the osteotomy is performed two-thirds of the way through the firstmetatarsal at the junction of the metaphysis and diaphysis and is oriented perpendicular to the long axis of the first metatarsal (
cut 2
). The second bone cut (
cut 3
) is made completely through the bone and completes the osteotomy. It should be made 2 to 4 mm proximal to the first cut and is perpendicular to the long axis of the second metatarsal. B. When seen from the medial side, the osteotomy should be oriented so that a small plantar-based wedge is produced. This helps avoid dorsiflexion of the distal fragment when the osteotomy is reduced. C,D. The osteotomy is reduced and stabilized with a 0.062-inch smooth Kirschner wire.Approach
1.
The surgeon should identify and protect the dorsal sensory nerve.Osteotomy
1.
The surgeon should avoid resecting more than about 3 mm of bone to preventshortening of the first metatarsal.Proximalosteotomy
1.
It should create a slight plantar-based wedge with the distal cut to avoiddorsiflexion of the osteotomy. ## PEARLS AND PITFALLS
POSTOPERATIVE CARE The toe is splinted in slight flexion. The dressing is covered with a cast. Weight bearing is allowed as tolerated.Pins are removed in 6 weeks. ## OUTCOMES Most studies report 65% to 85% good to excellent results with the Mitchell osteotomy. 1, 2, 3, 4The modified Mitchell osteotomy (described earlier) produces 81% satisfactory results, with no cases of malunion, nonunion, avascular necrosis of the first metatarsal head, infection, or transfer metatarsalgia. 3,4Sixty percent good to excellent results are reported in younger patients. ## COMPLICATIONS Infection Neurovascular injuryInadequate fixation of the osteotomyMalunion or nonunion of the osteotomy Avascular necrosis of the first metatarsal head
Transfer metatarsalgia RecurrenceStiffness of the first metatarsophalangeal joint Hallux varus (overcorrection)Pronation Pain ## REFERENCES
1. Davids JR, McBrayer D, Blackhurst DW. Juvenile hallux valgus deformity: surgical management by lateral hemiepiphyseodesis of the great toe metatarsal. J Pediatr Orthop 2007;27:826-830.
2.
Farrar NG, Duncan N, Ahmed N, et al. Scarf osteotomy in the management of symptomatic adolescent hallux valgus. J Child Orthop 2012;6:153-157.
3.
Kuo CH, Huang PJ, Cheng YM, et al. Modified Mitchell osteotomy for hallux valgus. Foot Ankle Int 1998;19:585-589.
4.
McDonald MG, Stevens DB. Modified Mitchell bunionectomy for management of adolescent hallux valgus. Clin Orthop Relat Res 1996;(332):163-169.
5.
Mitchell CL, Fleming JL, Allen R, et al. Osteotomy-bunionectomy for hallux valgus. J Bone Joint Surg Am 1958;40-A(1):41-58.
6.
Weiner BK, Weiner DS, Mirkopulos N. Mitchell osteotomy for adolescent hallux valgus. J Pediatr Orthop 1997;17:781-784.
