Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows, to the operating theater. Today, we embark on a comprehensive, rigorous journey through the essential surgical approaches to the shoulder and humerus. As orthopedic surgeons, our ability to effectively and safely navigate the complex three-dimensional anatomy of the shoulder girdle dictates our clinical success. Our goal is not merely to understand the rudimentary mechanics of an approach, but to master the underlying philosophy of why we select a specific trajectory, how to execute each maneuver with absolute precision, and how to proactively anticipate the anatomical pitfalls that lead to catastrophic complications. Scrub in, let's begin.
The patho-epidemiology of shoulder disorders necessitates a profound understanding of both anterior and anterosuperior surgical corridors. We frequently encounter an aging demographic presenting with degenerative conditions such as primary glenohumeral osteoarthritis, massive irrepairable rotator cuff tears leading to cuff tear arthropathy, and complex proximal humerus fractures resulting from low-energy falls. Simultaneously, our younger athletic population presents with recurrent anterior glenohumeral instability, labral pathology, and high-energy traumatic injuries. The incidence of total shoulder arthroplasty (TSA) and reverse total shoulder arthroplasty (rTSA) has grown exponentially over the last two decades, elevating the deltopectoral approach from a standard exposure to an indispensable, high-frequency requisite in the orthopedic armamentarium.
Surgical approaches to the shoulder are fundamentally divided by their relationship to the surrounding musculature, specifically whether they exploit an internervous plane or require an intramuscular split. The classic anterior deltopectoral approach is the quintessential internervous plane, exploiting the embryological and neurovascular boundary between the axillary nerve-innervated deltoid and the pectoral nerve-innervated pectoralis major. This preserves dynamic muscle function, which is critical for post-operative rehabilitation. Conversely, the anterosuperior approach utilizes an intramuscular split through the anterior deltoid. While it does not offer an internervous plane, it provides unparalleled, direct orthogonal access to the greater tuberosity and the supraspinatus footprint, making it invaluable for specific rotator cuff pathologies and antegrade intramedullary nailing of the humerus.
This chapter will serve as your definitive intraoperative guide. We will dissect the granular details of surgical anatomy, outline exhaustive indications, discuss rigorous pre-operative planning, and provide a step-by-step masterclass on the execution of these approaches. Furthermore, we will critically evaluate the potential complications, their respective incidence rates, and the salvage maneuvers required when the anatomy deviates from the textbook norm. Mastery of these approaches is the absolute foundation upon which successful shoulder surgery is built.
Detailed Surgical Anatomy and Biomechanics
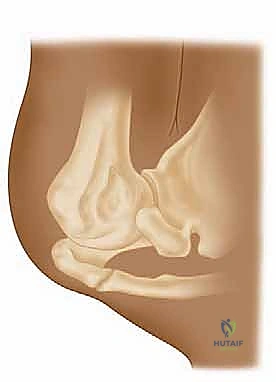
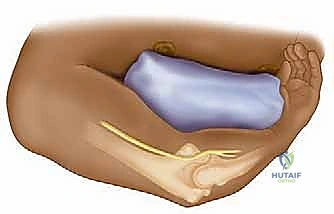
Before a scalpel ever touches the skin, the operating surgeon must possess a three-dimensional, high-fidelity mental model of the underlying anatomy. The shoulder is an inherently unstable joint, relying heavily on a complex interplay of static ligamentous restraints and dynamic muscular forces. The osteology of the proximal humerus features the greater and lesser tuberosities, separated by the bicipital groove, which houses the long head of the biceps tendon. The coracoid process, projecting anteriorly from the scapula, serves as the "lighthouse" of the anterior shoulder, functioning as the origin for the conjoined tendon (short head of the biceps and coracobrachialis) and the insertion site for the pectoralis minor.

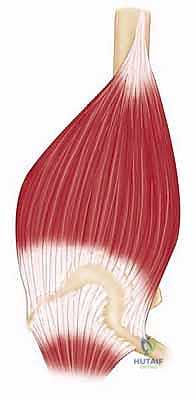
The muscular intervals define our surgical corridors. The anterior approach primarily utilizes the deltopectoral interval, a natural cleavage plane between two major muscles. Laterally lies the deltoid muscle, supplied by the axillary nerve (C5-C6), which wraps transversely around the surgical neck of the humerus. Medially lies the pectoralis major muscle, supplied by the medial and lateral pectoral nerves (C5-T1). In contrast, the anterosuperior approach utilizes a split through the deltoid fibers. Because the deltoid is detached proximal to its nerve supply, there is no true internervous plane with this approach, making a thorough understanding of the axillary nerve's trajectory absolutely paramount to avoid denervating the anterior deltoid.
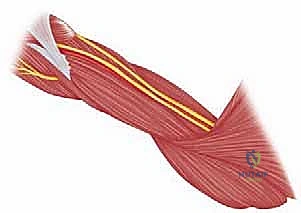
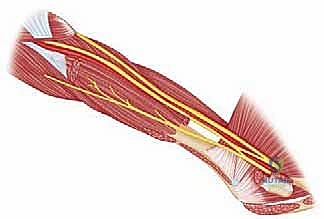
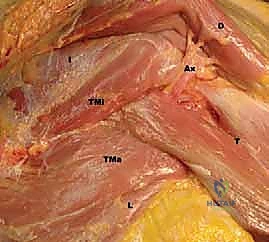
Neurovascular structures dictate the safety boundaries of our dissection. In the anterior approach, the cephalic vein typically resides within the deltopectoral groove, serving as a crucial superficial landmark. Deep to the interval, the musculocutaneous nerve (C5-C7) is a significant concern; it typically pierces the coracobrachialis muscle approximately 5 to 8 cm distal to the coracoid tip. Overly aggressive medial retraction of the conjoined tendon can easily cause a traction neurapraxia. The axillary nerve, while less directly exposed initially, becomes critical when working inferiorly along the subscapularis border or when detaching the deltoid. It runs along the inferior border of the subscapularis as it exits the quadrangular space.
As we approach the inferior border of the subscapularis during the deltopectoral approach, we will encounter the "three sisters." These are three small, transversely running vessels—branches from the anterior humeral circumflex artery and its venae comitantes. They require meticulous identification and ligation or bipolar cauterization to prevent obscuring the surgical field with hemorrhage. In the anterosuperior approach, the critical structure is the axillary nerve itself, which crosses the deep surface of the deltoid approximately 5 to 7 cm distal to the lateral edge of the acromion. Any deltoid split extending beyond this 5 cm safe zone risks catastrophic denervation of the anterior deltoid, leading to profound functional loss.
Exhaustive Indications and Contraindications
The selection of a surgical approach is a nuanced decision predicated on the specific pathology, the required exposure, the patient's physiological status, and the surgeon's familiarity with the regional anatomy. The anterior deltopectoral approach is the absolute workhorse of shoulder surgery. Its versatility and excellent, expansile exposure make it our preferred gateway for a multitude of procedures. It is the gold standard for anatomic total shoulder arthroplasty and hemiarthroplasty, providing direct access to the glenohumeral joint after subscapularis mobilization. It is also the primary approach for open surgical stabilization of recurrent anterior glenohumeral dislocations (e.g., Latarjet procedure, open Bankart repair).
Furthermore, the deltopectoral approach is highly indicated for the internal fixation of complex proximal humerus fractures, particularly those involving the surgical neck or lesser tuberosity, where medial calcar visualization is critical. It is also utilized for the repair of isolated subscapularis muscle tears and primary biceps tenodesis. Conversely, the anterosuperior (deltoid split) approach provides superior, direct orthogonal access to the superior and lateral aspects of the proximal humerus. It is highly indicated for open or mini-open rotator cuff repairs (specifically supraspinatus and infraspinatus), subacromial decompression, and the fixation of isolated greater tuberosity fractures.
Contraindications to these approaches must be strictly respected. Absolute contraindications for either approach include active, untreated local soft tissue infection or osteomyelitis, unless the approach is being utilized explicitly for radical debridement and irrigation. Relative contraindications for the deltopectoral approach include previous extensive surgical scarring that obliterates the internervous plane, or a pre-existing axillary nerve palsy where further manipulation might compromise any remaining deltoid function. For the anterosuperior approach, a relative contraindication is a pathology requiring extensive inferior glenoid exposure, as the distal extension of this approach is strictly limited by the axillary nerve.
| Approach Type | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Anterior (Deltopectoral) | Total Shoulder Arthroplasty, Hemiarthroplasty, Open Anterior Stabilization (Latarjet/Bankart), Proximal Humerus ORIF, Subscapularis Repair. | Active local infection (unless for I&D), Uncorrectable coagulopathy. | Severe prior scarring obliterating the interval, Pre-existing axillary nerve palsy, Need for posterior glenoid access. |
| Anterosuperior (Deltoid Split) | Open/Mini-open Rotator Cuff Repair, Greater Tuberosity ORIF, Antegrade IM Nailing of Humerus, Subacromial Decompression. | Active local infection (unless for I&D), Uncorrectable coagulopathy. | Pathology requiring inferior glenoid access, Need for distal humeral shaft exposure (due to axillary nerve limit). |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the hallmark of a master surgeon. Advanced imaging is no longer optional; it is mandatory. For arthroplasty and complex fracture cases, a high-resolution, fine-cut computed tomography (CT) scan with 3D reconstruction is essential. This allows for precise evaluation of glenoid version, vault bone stock, and tuberosity displacement. We utilize digital templating software to anticipate component sizing, screw trajectory, and the necessity for bone grafting. For soft tissue pathology, a high-field magnetic resonance imaging (MRI) scan is scrutinized to assess rotator cuff integrity, muscle atrophy, and fatty infiltration (Goutallier classification), which directly influences the repairability and approach selection.

Patient positioning is paramount for optimal exposure, intraoperative safety, and anesthetic management. We exclusively utilize the beach chair position for these approaches. This position allows for excellent, unhindered access to the anterior and superior shoulder, facilitates intraoperative fluoroscopy without moving the patient, and allows for dynamic manipulation of the arm through a full range of motion. The patient's torso is elevated to approximately 45 to 60 degrees. It is critical to coordinate with the anesthesia team regarding hemodynamic management; the beach chair position can induce cerebral hypoperfusion due to gravity-dependent venous pooling, necessitating meticulous blood pressure monitoring, often via an arterial line in high-risk patients.
The head must be secured in a neutral position using a dedicated head positioner to prevent cervical spine hyperextension, hyperflexion, or excessive rotation, which could compromise the cervical nerve roots or carotid/vertebral blood flow. The operative arm is prepped and draped free. We highly recommend the use of a sterile mechanical arm positioner (e.g., Spider arm or TRIMANO device) to reliably hold the arm in varying degrees of flexion, abduction, and rotation, reducing the physical burden on the surgical assistant and ensuring stable exposure during critical steps like glenoid preparation.
Fluoroscopy setup must be finalized before the sterile drape is applied. The C-arm should be brought in from the contralateral side or from the head of the bed, depending on the specific OR footprint. The surgeon must verify that perfect anteroposterior (AP), true scapular Y, and axillary lateral views of the shoulder can be obtained seamlessly without requiring repositioning of the patient or major adjustments to the C-arm base. Ensure adequate, thick padding is placed at all pressure points, specifically the sacrum, the contralateral heel, and the ulnar nerve at the cubital tunnel to prevent perioperative neuropraxias.
Step-by-Step Surgical Approach and Fixation Technique
The Anterior Deltopectoral Approach
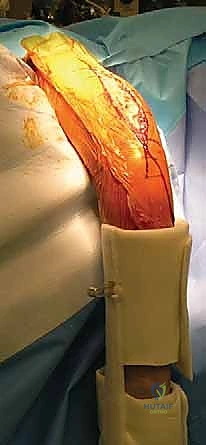
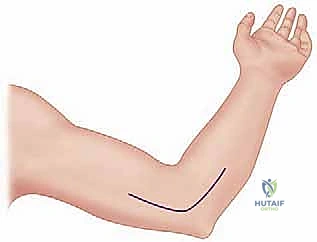
We begin with the skin incision. The choice of incision is dictated by the extent of exposure required and the patient's cosmetic concerns. The standard anterior deltopectoral incision is initiated with a #10 blade. We make a precise 10 to 15-cm curvilinear incision beginning just superior to the tip of the coracoid process. The incision curves distally and laterally, following the natural skin lines and the trajectory of the deltopectoral interval, progressing towards the deltoid tuberosity on the lateral humerus.

Alternatively, for more limited exposures, particularly for specific capsular repairs or cosmetic anterior instability procedures, an axillary incision may be selected. This 8 to 10 cm vertical incision is positioned more inferiorly, beginning below the coracoid tip and extending towards the anterior axillary fold. While cosmetically superior, it restricts proximal extension if the pathology is more complex than anticipated.

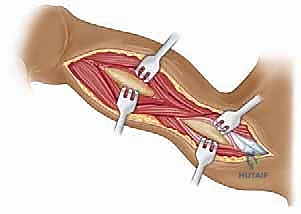
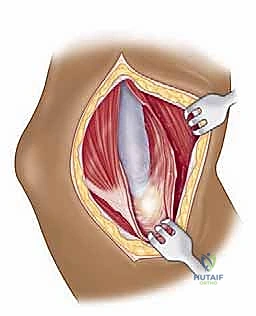
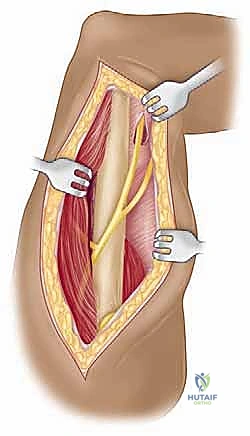
Following the incision, we deepen our dissection through the subcutaneous tissue, maintaining strict hemostasis with electrocautery. We carefully raise thick subcutaneous flaps medially and laterally to expose the underlying deltopectoral fascia. The critical superficial landmark, the cephalic vein, must be identified within the fat of the deltopectoral groove. Our preference is to mobilize the cephalic vein laterally with the deltoid muscle. The majority of the venous tributaries enter from the deltoid; therefore, lateral retraction typically results in fewer avulsed tributaries, less venous bleeding, and preserves the vein for potential future vascular access or minimizes post-operative edema.
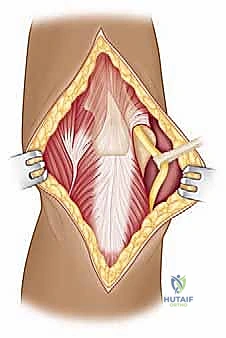
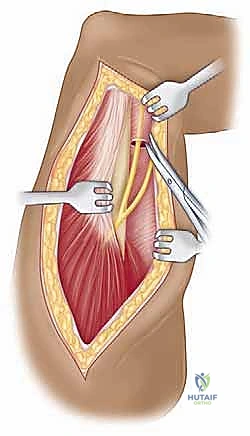
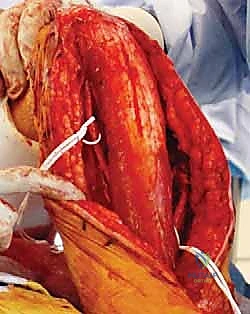
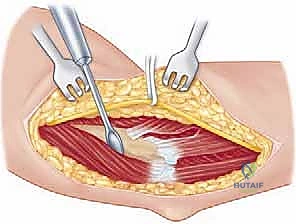
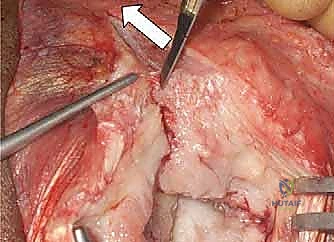
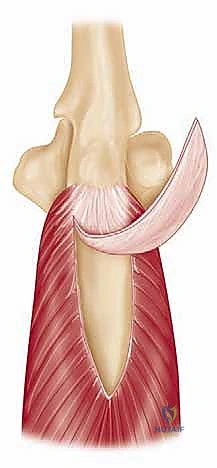
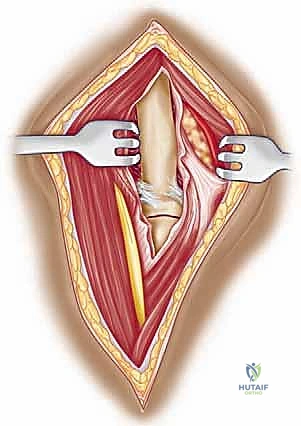
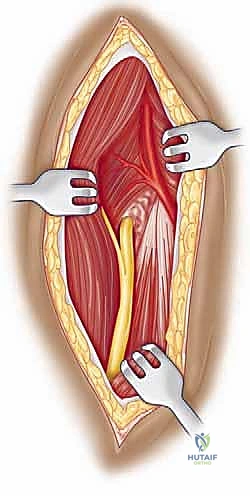
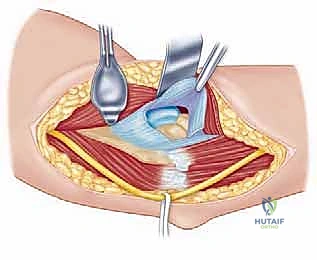
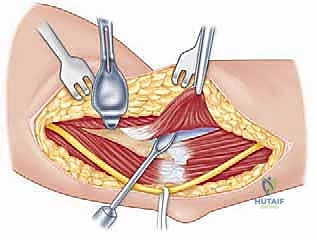
We then bluntly develop the internervous plane between the deltoid (axillary nerve) and the pectoralis major (pectoral nerves). Retractors are placed to maintain this interval. Deep in the wound, we identify the clavipectoral fascia, which is incised vertically lateral to the conjoined tendon. The conjoined tendon is then gently retracted medially. It is here that we must exercise extreme caution regarding the musculocutaneous nerve, which enters the medial aspect of the coracobrachialis 5-8 cm distal to the coracoid. Retraction must be gentle, intermittent, and strictly limited to the necessary exposure to prevent traction neurapraxia.
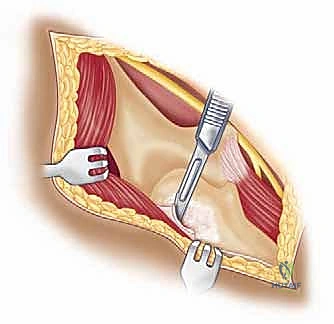
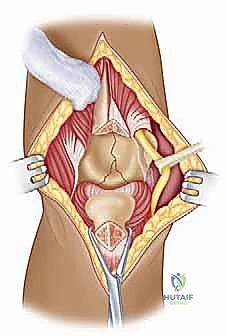
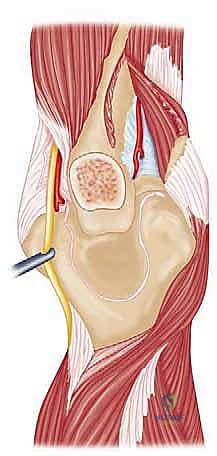
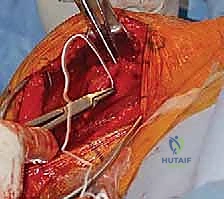
With the conjoined tendon retracted medially and the arm externally rotated, the subscapularis muscle comes into full view. External rotation is a critical maneuver; it delivers the lesser tuberosity into the wound and, crucially, increases the distance between the inferior border of the subscapularis and the axillary nerve, pulling the nerve away from our operative field. We identify the "three sisters" at the inferior border of the subscapularis and meticulously ligate them. Heavy non-absorbable stay sutures (e.g., #2 FiberWire) are placed at the superior and inferior borders of the subscapularis tendon. Depending on the pathology, we either perform a vertical tenotomy 1 cm medial to the lesser tuberosity or a lesser tuberosity osteotomy to reflect the subscapularis and expose the underlying anterior joint capsule.
The Anterosuperior Deltoid Split Approach
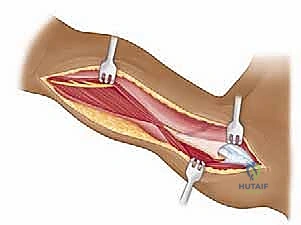
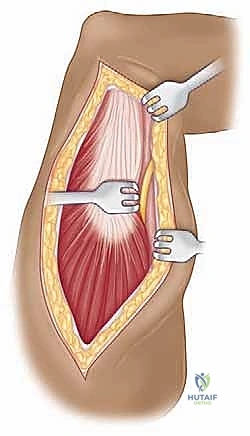
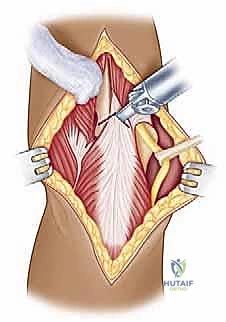
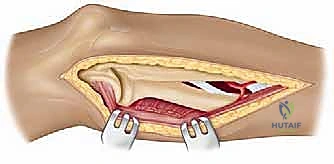
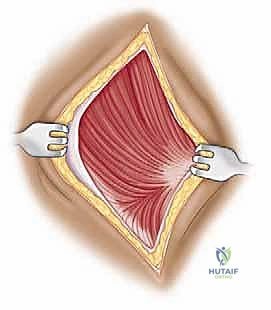
For pathologies requiring direct superior access, we employ the anterosuperior deltoid split. The incision begins at the anterolateral corner of the acromion and extends distally for approximately 4 to 5 cm parallel to the deltoid fibers. Subcutaneous flaps are minimized to maintain the vascularity of the skin edges. We identify the deep fascia covering the anterior deltoid and incise it in line with the skin incision.
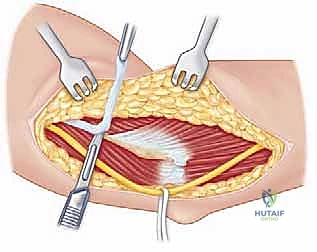
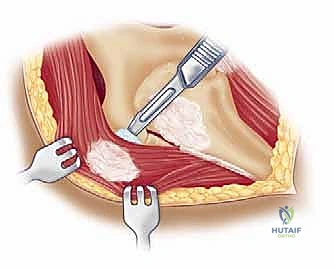
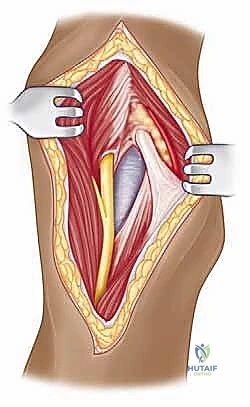
The critical step is the intramuscular split. We identify the raphe between the anterior and middle heads of the deltoid, which is often marked by a small fat stripe and a descending branch of the thoracoacromial artery. We bluntly split the deltoid fibers using a periosteal elevator or a closed Mayo scissor. To absolutely prevent catastrophic injury to the axillary nerve, the split must never extend further than 5 cm distal to the lateral edge of the acromion. We place a heavy, non-absorbable stay suture at the inferior apex of the split to physically block any inadvertent distal propagation during retraction.
Deep to the deltoid, we encounter the subacromial bursa, which is often thickened and inflamed. A subtotal bursectomy is performed using electrocautery to reveal the underlying rotator cuff (supraspinatus and infraspinatus tendons) and the greater tuberosity. If an acromioplasty is required, the approach can be extended proximally by subperiosteally elevating the anterior deltoid off the anterior acromion, taking care to achieve hemostasis from the acromial branch of the coracoacromial artery.
Once the pathology is addressed—whether it be placing suture anchors for a rotator cuff repair or inserting an intramedullary nail for a proximal humerus fracture—the closure must be meticulous. For the anterosuperior approach, the split deltoid fibers are loosely approximated with absorbable sutures, ensuring no tension is placed on the muscle belly. If the deltoid was elevated off the acromion, a robust transosseous repair is mandatory to prevent postoperative deltoid dehiscence, a devastating complication.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, complications can and do occur. A profound understanding of these risks allows the surgeon to diagnose them early and initiate appropriate salvage management. Neurologic injuries are among the most feared complications. In the anterior approach, the musculocutaneous nerve is the most frequently injured, with traction neurapraxia occurring in up to 2-8% of complex cases involving heavy medial retraction. This usually presents as transient weakness in elbow flexion and altered sensation in the lateral forearm. It is typically managed expectantly with observation and physical therapy, with recovery expected within 3 to 6 months.
Injury to the axillary nerve is a more severe complication, risking permanent deltoid dysfunction. In the anterosuperior approach, splitting the deltoid beyond the 5 cm safe zone can directly transect the nerve. In the anterior approach, aggressive inferior capsular release or errant retractor placement inferior to the glenoid can compress or stretch the nerve. Incidence is roughly 1-2%. If a direct transection is recognized intraoperatively, primary microsurgical repair or nerve grafting is mandated. If diagnosed post-operatively (manifesting as inability to abduct the arm and lateral shoulder numbness), an EMG is obtained at 3-4 weeks. Lack of recovery by 3-6 months may necessitate nerve transfer procedures (e.g., radial nerve branch to axillary nerve).
Vascular complications, though rare, can be life-threatening. The axillary artery and vein lie medial to the coracoid and can be injured by aberrant retractor placement or during revision surgery with distorted anatomy. Immediate vascular surgery consultation, proximal control, and primary repair or grafting are required. More commonly, the cephalic vein may be lacerated or thrombosed. While generally well-tolerated due to collateral venous drainage, it can lead to increased post-operative upper extremity edema. If torn intraoperatively, it should be cleanly ligated rather than repaired.
Biomechanical failures of the soft tissue repair are a significant source of postoperative morbidity. Failure of the subscapularis repair following a deltopectoral approach for arthroplasty occurs in 2-5% of cases and presents with increased passive external rotation, weakness in internal rotation (positive belly-press or bear-hug tests), and potential anterior instability of the prosthesis. Salvage may require revision open repair, Achilles tendon allograft reconstruction, or conversion to a reverse total shoulder arthroplasty if the patient is older and the cuff is deemed irreparable. Deltoid dehiscence following an anterosuperior approach is a catastrophic failure of the proximal repair, leading to a profound inability to elevate the arm. Salvage is extraordinarily difficult, often requiring complex rotational flaps or accepting the functional deficit.
| Complication | Estimated Incidence | Etiology / Mechanism | Salvage / Management Strategy |
|---|---|---|---|
| Musculocutaneous Neurapraxia | 2% - 8% | Excessive, prolonged medial retraction of the conjoined tendon. | Expectant management, physical therapy. Most recover in 3-6 months. |
| Axillary Nerve Injury | 1% - 2% | Deltoid split >5cm (Anterosuperior), aggressive inferior dissection (Anterior). | Intra-op: Microsurgical repair. Post-op: EMG at 4 weeks, consider nerve transfer if no recovery by 6 months. |
| Subscapularis Failure | 2% - 5% | Poor tissue quality, over-tensioning, non-compliance with rehab post-TSA. | Revision repair, allograft reconstruction, or conversion to rTSA. |
| Deltoid Dehiscence | < 1% | Failure of transosseous repair at the acromion (Anterosuperior extension). | Extremely difficult salvage. Attempt revision transosseous repair with heavy non-absorbable sutures/anchors; potential flap coverage. |
Phased Post-Operative Rehabilitation Protocols
The surgical approach is only the first half of the therapeutic equation; a meticulously phased, biologically respectful rehabilitation protocol is mandatory for optimal outcomes. The rehabilitation phases are dictated by the specific tissues incised and repaired during the approach. For the anterior deltopectoral approach involving a subscapularis tenotomy and repair, the primary goal in Phase I (Weeks 0-4) is the absolute protection of the anterior soft tissue envelope. The patient is placed in a standardized shoulder immobilizer or sling. Passive range of motion (PROM) is initiated immediately but is strictly limited in external rotation—typically capped at 30 degrees, or whatever safe tension limit was determined intraoperatively by the surgeon.
Phase II (Weeks 4-8) marks the transition to active-assisted range of motion (AAROM) and the gradual weaning of the sling. As the subscapularis repair achieves early biological healing, external rotation limits are slowly advanced. The focus shifts to restoring normal scapulothoracic rhythm and preventing adhesive capsulitis. Pulley exercises, wand exercises, and supine forward elevation are introduced. Active internal rotation behind the back is still restricted to prevent excessive stress on the healing subscapularis tendon.
Phase III (Weeks 8-12) introduces early strengthening. Assuming clinical and radiographic evidence of healing (if osteotomies were performed), isometric exercises progress to light isotonic resistance. Rotator cuff and periscapular strengthening become the primary focus, utilizing elastic bands and light free weights. For patients who underwent an anterosuperior approach with a deltoid split, anterior deltoid strengthening is initiated carefully, ensuring no pain at the proximal acromial origin if it was elevated.
Phase IV (Months 3-6 and beyond) is the advanced strengthening and return-to-activity phase. The goal is to maximize dynamic stability and muscular endurance. Plyometric exercises, proprioceptive neuromuscular facilitation (PNF) patterns, and sport-specific or work-specific drills are incorporated. Full clearance for heavy lifting or contact sports is rarely granted before the 6-month mark, and only when the patient demonstrates symmetrical strength, full functional range of motion, and an absence of scapulothoracic dyskinesia.
Summary of Landmark Literature and Clinical Guidelines
Our current understanding and execution of these surgical approaches are built upon decades of rigorous anatomical studies and clinical outcomes research. Historically, Charles Neer's seminal work in the 1970s and 1980s popularized the deltopectoral approach as the gold standard for proximal humerus fracture fixation and shoulder arthroplasty. His detailed descriptions of the intern
Clinical & Radiographic Imaging Archive