Wrist arthroscopy
Preoperative planning
Indications
Assessment and treatment of radiocarpal and mid-carpal joint problems to include:
1. Chondral surfaces and debridement of lesions
2. Triangular fibrocartilage complex (TFCC) assessment and treatment
3. Assessment and assistance of fracture reduction (distal radius, scaphoid)
4. Carpal instability diagnosis and treatment
5. Kienbock’s disease assessment and treatment
6. Dorsal wrist ganglion excision
7. Septic arthritis irrigation and debridement
8. Removal of loose bodies
9. Synovectomy
Contraindications
10. Persistent infection of overlying skin
11. Lack of appropriate instrumentation
12. Caution in cases where shoulder or elbow stiffness is present
Operative planning
History, clinical examination and recent radiology investigations should guide the clinical questions and indications. Appropriate equipment must be available, usually a 2.4–3 mm,
30°-angled arthroscope, a traction tower or similar device and any specific additional procedure-specific equipment.
Consent and risks
1. Nerve injury – superficial radial nerve branches, dorsal cutaneous branch of ulnar nerve
2. Infection
3. Haematoma
4. Vascular injury (usually dorsal venous branches)
5. Extensor tendon injury
6. Postoperative stiffness
Anaesthesia and positioning
Anaesthesia is general or regional in a supine position. An above-elbow tourniquet is recommended and inflated to 250 mm Hg. The shoulder is abducted to 90°, placing the arm on a side extension. Ideally a wrist arthroscopy traction tower is used. Finger traps are applied to the index and middle fingers. The arm is anchored to the base of the tower by means of a strap attached proximal to the elbow. The elbow joint is flexed to 90° and traction of up to 4.5 kg is applied through the finger traps (Figure** 8.1).

Figure 8.1 Wrist arthroscopy patient setup.
Landmarks and surgical technique
Marking the tips of the radial and ulnar styloids allows initial referencing and rough approximation of radiocarpal and mid-carpal joint levels. Saline is injected to distend the joint capsule although the procedure can be performed dry. The site or method of saline injection corresponds to the method of portal placement. The arthroscopic portals are named according to the wrist extensor compartments they lie between.
The 1–2 portal lies between the abductor pollicis longus (APL) and extensor carpi radialis brevis (ECRB) tendons. This portal is used less often due to the increased risk of injury to the radial artery and branches of the superficial radial nerve.
Lister’s tubercle is the landmark for the 3–4 viewing portal which is usually placed first. The tubercle is palpated with the thumb which is then gently rolled distally, over the distal rim of the radius and into a soft spot between the extensor pollicis longus (EPL) tendon and the radial border of the fourth compartment. This point corresponds with the level of the scapholunate joint. A 1 or 2 mm incision is made in the skin only – deeper passage of the knife may risk injury to cutaneous nerves or underlying tendons. A blunt trocar or small curved haemostat is used to access the joint by applying gentle pressure and puncturing the dorsal capsule. The surgeon must account for the volar inclination of the radius in order to access the joint with minimal trauma. After placement of the 3–4 viewing portal, all subsequent portals are placed under direct vision. To facilitate ideal incision placement, a needle is placed intra-articularly in the proposed portal location before the skin incision is made.
The distal radio ulnar joint (DRUJ) is usually easily identified by palpation alone, but the joint line can be confirmed by dorsal/volar translation of the ulna respective to the radius. The tendon of extensor digiti minimi (EDM) overlies the joint, making the DRUJ a useful reference point for the 4–5 portal.
The ulnar head and base of the ulnar styloid are used to reference the level of the ulnocarpal joint. The extensor carpi ulnaris (ECU) can be palpated along the radial border of the styloid allowing placement of the 6R portal. The author’s preference is to use the 6R portal for initial saline injection as the space between the triquetrum and the distal ulna is often easier to initially access. In-flow is simply established using a large syringe and simple tubing connected to the viewing portal. An assistant can apply gentle pressure and maintain a sufficient volume of fluid within the joint to maintain a good view. The surgeon must be mindful that in the presence of tears affecting the deep attachment of the TFCC, excessive volumes of fluid can transfer into the tissues of the distal forearm. Similarly, the use of high pressure during saline in-flow can cause swelling of the subcutaneous tissues around the portal sites thus hampering insertion of instruments. The 6U portal can be placed ulnar to the ECU tendon. Care must be taken to avoid iatrogenic injury to the TFCC or to the dorsal sensory branch of the ulnar nerve during placement of ulnar-sided portals.
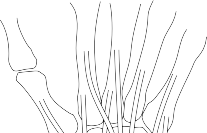
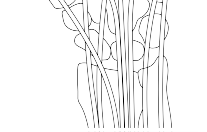
There are two mid-carpal (MC) portals. The radial MC portal lies 2 cm distal to the 3–4 portal and can often be palpated as a soft spot. The ulnar MC portal lies 2 cm distal to the 4–5 portal, again palpable as a soft spot. Due to the oblique inclination of the scapho-capitate joint, the ulnar MC portal is often easier to access first. The radial MC portal can be placed under accurate direct visualisation (Figure** 8.2).
TH
STT
1–2
3–4
6U
Radial mid-carpal
Ulnar
mid-carpal
6R
4–5





























Procedure
Figure 8.2 Radiocarpal and mid-carpal portals.
The procedure is dependent on the indication. As always, a reproducible, structured approach ensures that all essential structures are adequately visualised and relevant pathology is readily identified.
Closure
Steri-Strips are sufficient to close the skin defects, and a compression bandage is then applied.
Postoperative care and instructions
The patient is usually advised to mobilise as pain allows; however, this will be dependent on the underlying pathology treated.
Recommended
Scientific References
-
Ahsan ZS, Yao J. Complications of wrist arthroscopy. _Arthroscopy_. 2012;28(6):855–859. Michelotti B, Chung K. Diagnostic wrist arthroscopy. _Hand Clin_. 2017;33(4):571–583.
Wagner J, Ipaktchi K, Livermore M, Banegas R. Current indications for and the technique of wrist arthroscopy. _Orthopedics_. 2014;37(4):251–256.
Wolf JM, Dukas A, Pensak M. Advances in wrist arthroscopy. _J Am Acad Orthop Surg_. 2012;20(11):725–734.
[First extensor compartment (De Quervain’s) release](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark16)
[Preoperative planning](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark16)
_Indications_
- 1. Stenosing tenovaginitis of the APL and extensor pollicis brevis (EPB) in the first extensor compartment [View Source / PubMed]
- 2. Failure of conservative measures _Contraindications_ [View Source / PubMed]
- 3. Infection of overlying skin or inadequate skin cover _Consent and risks_ [View Source / PubMed]
- 1. Nerve injury and/or neuroma formation: Superficial radial nerve branches [View Source / PubMed]
- 2. Failure of symptomatic relief [View Source / PubMed]
- 3. Tendon instability, subluxation or adhesions _Operative planning_ Confirmation of the diagnosis and exclusion of other sources of pain are essential. Other conditions that may mimic De Quervain’s include the following: [View Source / PubMed]
- 4. Flexor carpi radialis (FCR) tenosynovitis [View Source / PubMed]
- 5. Trapezio-metacarpal joint injury, synovitis or degeneration [View Source / PubMed]
- 6. Radioscaphoid impingement or degeneration [View Source / PubMed]
- 7. Second or third compartment tenosynovitis [View Source / PubMed]
- 8. Intersection syndrome – inflammation between the intersection of the first dorsal compartment (APL and EPB) and second dorsal compartment (extensor carpi radialis longus and extensor carpi radialis brevis). [Anatomic variations in this compartment are common, and this may play a major role in the disease process. Knowledge of this variability is important for adequate surgical decompression and prevention of postoperative complications (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark31)**[Figure** ](#bookmark31)**8.3**). Abductor pollicis longus tendon usually inserts on the base of the first metacarpal Often the abductor pollicis longus has an additional insertion Extensor pollicis brevis tendon with a separate tendon           Figure 8.3 First dorsal compartment anatomy. _Anaesthesia and positioning_ General, regional or local anaesthesia can be used. A bloodless field is recommended in order to adequately visualise the structures at risk and to readily identify anatomic variants. Local anaesthesia with adrenaline can be used as an alternative to use of a tourniquet. The supine position is used with a hand table. Surgical technique _Landmarks_ [View Source / PubMed]
- 9. Bone: Radial styloid, Lister’s tubercle [View Source / PubMed]
- 10. Tendon: APL and EPB – lie over the lateral aspect of the distal radius; represent the radial border of the anatomic snuffbox _Incision_ Longitudinal: 2–3 cm incision based over the radial styloid and in line with the first metacarpal. A degree of obliquity can be incorporated in order to provide adequate exposure along the direction of the tendons. This can be extended proximally or distally if required. A transverse incision can be used, but this is associated with a higher rate of iatrogenic nerve injury and extension of the incision is more difficult. _Dissection_ _Structures at risk_ [View Source / PubMed]
- 1. Branches of superficial radial nerve (SRN) [View Source / PubMed]
- 2. Superficial veins In most cases, a branch of the SRN lies immediately under the skin within the subcutaneous fat. Therefore, careful skin incision and meticulous dissection technique are required to identify and protect the nerve. Care must be taken and use of retractors with sharp hooks or teeth should be avoided if possible. Any dorsal vein branches are mobilised and retracted. _Procedure_ Identification of the extensor retinaculum is made easier by use of a sweeping motion with a wet swab. Passive movement of the thumb and first metacarpal will help identify the first extensor compartment and the boundary of the second compartment located dorsally. The proximal and distal margins of the retinaculum should be identified, but clear visualization can sometimes be made difficult due to adjacent connective tissue. A longitudinal incision is then made in a dorsal position along the first compartment, and the retinaculum is opened leaving a volar flap of retinaculum to prevent subluxation. The compartment is carefully explored for the single tendon of the EPB, and the multiple tendon slips of the APL. The fibro-osseous canal is then examined for septation and extra or aberrant tendons. If present, an intracompartmental septum containing additional tendon slips is usually located on the volar aspect of the compartment and must also be released. Failure to recognise and decompress this sub-sheath is a common cause of persistent pain after surgery. [If the procedure is done under local anaesthesia, the tendons are replaced and the patient asked to move the thumb to demonstrate adequate decompression and independent movement. Instability is checked for and corrected, if necessary, by loosely opposing the edges of the tendon sheath (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark32)**[Figure** ](#bookmark32)**8.4**). First dorsal compartment     Figure 8.4 First dorsal compartment. _Closure_ The tourniquet is deflated, and haemostasis is obtained. The skin is closed with a subcuticular suture. Bulky compressive dressing is applied. No splint is used for immobilisation, and early motion is encouraged. _Postoperative care and instructions_ The pressure dressing is removed after 48 hours. Thumb and hand movements are initiated and increased according to comfort. Hand therapy is occasionally needed and recommended on an as-needed basis. Recommended references Adams J, Habbu R. Tendinopathies of the hand and wrist. _J Am Acad Orthop Surg_. 2015;23(12):741–750. Gundes H, Tosun B. Longitudinal incision in surgical release of de Quervain disease. _Tech Hand Up Extrem_ _Surg. 2005;9(3):149–152._ Scheller A, Schuh R, Hönle W, Schuh A. Long-term results of surgical release of de Quervain’s stenosing tenosynovitis. _Int Orthop_. 2008;33(5):1301–1303. [Ganglion excision at the ](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark17)[wrist](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark17) A ganglion is a mucin-filled cyst which may be uni- or multi-lobulated. It is the most common soft tissue tumour of the hand, representing up to 70% of all such lesions. Dorsal wrist ganglia represent over 70% of all ganglia and most frequently arise from the scapholunate ligament (SLL). Volar wrist ganglia account for up to 20% of all ganglia and commonly arise from the scapho-trapezial joint. Many ganglia are asymptomatic and are incidental findings at the time of magnetic resonance imaging (MRI) or ultrasound investigation. Others however are symptomatic, especially dorsal scapholunate ganglia that typically cause dorsal impingement pain when weightbearing through the extended wrist. Preoperative planning _Indications_ [View Source / PubMed]
- 11. Pain [View Source / PubMed]
- 12. Interference with activity [View Source / PubMed]
- 13. Nerve compression [View Source / PubMed]
- 14. Enlarging [View Source / PubMed]
- 15. Failed aspiration (success rate approximately 50% with needle aspiration) _Consent and risks_ [View Source / PubMed]
- 1. Numbness and scar sensitivity [View Source / PubMed]
- 2. Recurrence [View Source / PubMed]
- 3. Nerve injury and neuroma formation: Superficial branch of radial nerve in dorsal ganglia [View Source / PubMed]
- 4. Vascular injury: Radial artery injury requiring repair with volar ganglia [View Source / PubMed]
- 5. Postoperative stiffness [View Source / PubMed]
- 6. Scapholunate instability: Rare _Anaesthesia and positioning_ General anaesthesia, regional anaesthesia or wide awake local anaesthesia no tourniquet (WALANT) are preferred. Local anaesthesia without adrenaline or tourniquet is possible, but a bloodless field is preferred and allows accurate visualisation of the neck of the ganglion and structures at risk. The patient is positioned supine and the hand positioned on a hand table. Surgical technique The technique described is dorsal scapholunate ganglion excision. Arthroscopic excision and open excision have similar recurrence rates. However, arthroscopic resection can be technically more challenging and requires the surgeon to be comfortable with arthroscopic procedures. However, it can lead to a quicker postoperative recovery. Both techniques aim to excise the neck or the origin of the ganglion as it arises from the dorsal ligament fibres and adjacent capsular attachment. Arthroscopically it is performed according to the techniques described earlier by excising the dorsal capsule overlying the scapholunate articulation with use of an arthroscopic shaver. An open excision is more often used. _Incision_ [A transverse or longitudinal incision can be used. Transverse incisions can be placed along Langer’s lines or existing skin creases, but care must be taken to avoid injury to dorsal nerves, veins and tendons. Longitudinal incisions can be more easily extended but perhaps less cosmetic (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark34)**[Figure** ](#bookmark34)**8.5**).      Figure 8.5 Skin incision for dorsal ganglion excision. _Structures at risk_ [View Source / PubMed]
- 1. Dorsal sensory branches of radial (or ulnar) nerve – these must be identified and protected [View Source / PubMed]
- 2. Dorsal veins [View Source / PubMed]
- 3. EPL and extensor digitorum communis (EDC) tendons _Procedure_ [The cyst usually lies between the third and fourth extensor compartments but variability exists. Large ganglia will grow between extensor tendons and herniate through the extensor retinaculum to lie under the skin. Their position relative to the boundaries of the retinaculum must be appreciated as a retinacular release is often needed to visualise the neck. Care must be taken to identify the EPL tendon to avoid iatrogenic injury. The EPL and ECRB tendons are retracted radially and EDC tendons retracted ulnarly. Careful deep dissection around the borders of the ganglion will allow location of its neck. The ganglion must be resected at its base from the level of the capsule. A small capsular resection at this site will allow for visualisation of the dorsal SLL which is then gently curettaged. Again, care must be taken not to damage ligament fibres during the resection (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark35)**[Figure** ](#bookmark35)**8.6**). _Closure_ Avoid closure of the capsule to prevent joint stiffness. Haemostasis is achieved after tourniquet release. Vicryl is used to close the retinaculum and subcuticular suture to close the skin. A volar splint is applied in neutral.            Figure 8.6 Excision of the ganglion and its stalk from the scapholunate ligament. Surgical technique – ganglion of the scapho-trapezial joint _Structures at risk_ [View Source / PubMed]
- 1. The palmar cutaneous branch of the median nerve [View Source / PubMed]
- 2. The radial artery: Identification and mobilisation are vital; ganglion and artery are often closely associated _Landmarks_ [View Source / PubMed]
- 16. Scaphoid tubercle [View Source / PubMed]
- 17. Flexor carpi radialis tendon [View Source / PubMed]
- 18. Radial artery _Incision_ A longitudinal incision is created over the ganglion. _Dissection and procedure_ The radial artery and vein are identified and retracted radially, taking care to cauterise any small side branches. If needed the FCR can be mobilised and retracted in an ulnar direction. The ganglion is dissected down to its origin (usually the scapho-trapezial joint) and is excised with a small portion of surrounding capsule which is left open. Recommended references Angelides AC, Wallace PF. The dorsal ganglion of the wrist: Its pathogenesis, gross and microscopic anatomy, and surgical treatment. _J Hand Surg Am_. 1976;1:228–235. Finsen V, Håberg O, Borchgrevink GE. Surgery for wrist ganglia: One-hundred and twenty-two patients reviewed 8 years after operation. _Orthop Rev_. 2014;6(1):5162. Lidder S, Ranawat V, Ahrens P. Surgical excision of wrist ganglia; literature review and nine-year retrospective study of recurrence and patient satisfaction. _Orthop Rev_. 2009;1(1):e5. Mathoulin C, Mathilde Gras M. Arthroscopic management of dorsal and volar wrist ganglion. _Hand Clin_. 2017;33(4):769–777. [Wrist arthrodesis](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark20) Preoperative planning _Indications_ [View Source / PubMed]
- 19. Osteoarthritis [View Source / PubMed]
- 20. Rheumatoid or inflammatory arthritis [View Source / PubMed]
- 21. Joint destruction secondary to infection or tumour resection [View Source / PubMed]
- 22. Failed arthroplasty or limited fusion [View Source / PubMed]
- 23. Neuromuscular flexion contracture [View Source / PubMed]
- 24. Kienbock’s disease and pancarpal arthritis _Cautions and contraindications_ [View Source / PubMed]
- 25. Skeletal immaturity (open distal radius physis) [View Source / PubMed]
- 26. Relative contraindication where the contralateral wrist has already been fused [View Source / PubMed]
- 27. Caution advised in heavy smokers or those with multiple comorbidities that may hinder fusion _Consent and risks_ [View Source / PubMed]
- 1. Residual pain [View Source / PubMed]
- 2. Non-union [View Source / PubMed]
- 3. Extensor tenosynovitis [View Source / PubMed]
- 4. Loss of grip strength [View Source / PubMed]
- 5. Subsequent re-operation [View Source / PubMed]
- 6. Complex regional pain syndrome [View Source / PubMed]
- 7. Nerve injury and neuroma formation [View Source / PubMed]
- 8. DRUJ pain [View Source / PubMed]
- 9. Carpal tunnel syndrome [View Source / PubMed]
- 10. Ulnar abutment _Operative planning_ The surgeon must decide between full and partial wrist fusion based on the pathology and pattern of degeneration. Partial fusions such as radioscapholunate or a ‘four-corner’ arthrodesis may be good motion-preserving options, but each has specific procedural indications and technique. A ‘standard’ total wrist fusion includes radiocarpal, mid-carpal and carpometacarpal arthrodesis using an implant spanning the distal radius, across the carpus and fixed to the third metacarpal. Consider the need for bone grafting – autologous bone from the distal radius is not usually possible due to the necessity for placement of the plate over the site of harvest. Iliac crest harvest can be used if necessary and is usually sufficient unless there is severe bone loss. The pathologic process necessitating wrist arthrodesis may have resulted in distal radius or carpal collapse and resultant ulnocarpal impaction. This should be addressed at the time of operation in order to avoid ongoing causes of pain. Management options include a restoration of length or, more feasibly, an ulna resection or shortening osteotomy (described later). The position of fusion is 10°–20° of dorsiflexion and 0–10° of ulna deviation. This allows for functionality and preservation of grip strength. Maximum grip is generated in 35° of dorsiflexion, but this is less functional. In rheumatoid arthritis, a more neutral position may be preferred depending on how the disease process has affected the metacarpophalangeal joints. Bilateral wrist fusions should be considered very carefully due to the accompanying restrictions in function. In cases where one wrist has already been fused, a motion-preserving procedure is often preferred for the contralateral side. This may be in the form of a partial wrist fusion or a total wrist arthroplasty. If bilateral wrist fusions are to be undertaken, both wrists can be fixed in neutral or alternatively one in slight flexion and the other in slight extension depending on functional requirements. The choice of implant is dependent on patient anatomy, pathology and surgeon preference. Many manufacturers now provide a range of options including [View Source / PubMed]
- 28. Radiocarpal fusion with no additional metacarpal fixation [View Source / PubMed]
- 29. Radio-carpo-metacarpal fixation to either second or third metacarpals [View Source / PubMed]
- 30. Neutral or extended positions [View Source / PubMed]
- 31. Short and long bends to accommodate anatomy [View Source / PubMed]
- 32. Variable screw diameters to accommodate smaller metacarpal bones [View Source / PubMed]
- 33. Locking and non-locking screw options _Anaesthesia and positioning_ Anaesthesia is general or regional, and the supine position is used; a hand table, tourniquet and image intensifier are also required for the procedure. Surgical technique – dorsal approach to the wrist _Landmarks_ [View Source / PubMed]
- 34. Radial styloid process [View Source / PubMed]
- 35. Lister’s tubercle [View Source / PubMed]
- 36. DRUJ [View Source / PubMed]
- 37. Third metacarpal _Incision_ [This surgical approach can be applied to a multitude of procedures. For the purposes of a wrist fusion, it can be extended distally to allow for adequate exposure of the metacarpal if desired. A dorsal longitudinal incision (or ‘lazy S’) is used in line with the third metacarpal, Lister’s tubercle and distal radius (](#bookmark37)**Figure 8.7**). _Dissection_ Proximally, full-thickness skin flaps are raised allowing exposure of the underlying extensor retinaculum. Distal to the retinaculum the extensor tendons of the third and    Figure 8.7 Dorsal skin incision for wrist arthrodesis. fourth compartments (EPL and EDC) are identified. Several methods of negotiating the extensor retinaculum have been described and can be utilised including the following: [View Source / PubMed]
- 38. A longitudinal incision overlying the fourth compartment, elevation of the retinaculum and sequential releases of adjacent septations between compartments with retraction of tendons. Two flaps are created on either side of the fourth compartment for later repair. These can be elevated radially and ulnarly as far as necessary for adequate exposure. [View Source / PubMed]
- 39. An incision over EPL that exposes the tendon and allows it to be retracted. Subperiosteal resection of second and fourth compartments starting from the floor of the third allows them to remain unbreached within their retinacular sleeves. [View Source / PubMed]
- 40. A radially based retinacular flap extending from the second to fifth compartments which gives good exposure of radial and ulnar sides of the distal radius. [View Source / PubMed]
- 41. [A step-cut incision that allows for lengthening if needed at the time of closure. Alternatively, one of the transverse limbs can be used to cover a dorsally placed implant, thus protecting the overlying extensor tendons (](#bookmark38)**Figure 8.8**). Carpal bones Ulna Radius (a) (b)         Figure 8.8 (a) Approach to the wrist joint. (b) Axial view showing the approach between the third and fourth compartments. _Structures at risk_ [View Source / PubMed]
- 1. Dorsal veins [View Source / PubMed]
- 2. Superficial nerves – superficial radial nerve and dorsal cutaneous branch of ulnar nerve [View Source / PubMed]
- 3. Posterior interosseous nerve – see later With any of these approaches, the dorsal surface of the distal radius must be adequately exposed at both its radial and ulnar margins. Lister’s tubercle is excised (a rongeur is sufficient) to allow flat plate apposition. The posterior interosseous nerve is identified just proximal to the extensor retinaculum as it enters the radial side of the fourth compartment (it sits just ulnar to Lister’s tubercle), and a 2 cm segment is excised and the ends diathermied. The ECRB tendon may need to be released off the third metacarpal for plate apposition. To access the carpus, several capsulotomies have been described. For the purposes of a wrist fusion, these do not need to be anatomic (i.e. there is no ambition to mobilise the wrist and therefore anatomic repair of wrist ligaments or capsule is not necessary). Options for capsulotomy include the following: [View Source / PubMed]
- 42. A simple midline capsulotomy with elevation of radial and ulnar flaps. [View Source / PubMed]
- 43. A ‘Mayo’ capsulotomy – this is a ligament-preserving radially based flap with extensions along the dorsal radiocarpal and dorsal intercarpal ligaments. Provides good exposure and is easy to close. Care must be taken when exposing the ulnar aspect of the joint not to injure the dorsal limb of the TFCC. [View Source / PubMed]
- 44. A distally based flap initially elevating the capsule off the radiocarpal joint and extending distally – this is a good flap to consider when undertaking carpal surgery, but a further central split would need to be undertaken to accommodate plate placement. _Arthrodesis procedure_ After inspecting for arthritic lesions and making an assessment of the extent of their effects, the surgeon can sequentially perform the following: [View Source / PubMed]
- 45. Excision of the cartilage and the subchondral bone in the radioscaphoid and radiolunate joints and the intercarpal joints (scaphocapitate, lunocapitate and triquetrohamate) until the cancellous bone of each carpal bone is reached. To achieve this, a small burr (with irrigation), rongeur, curette or osteotome is sufficient. [View Source / PubMed]
- 46. Temporary fixation using K-wires, trying if possible to align the central axis between radius, lunate, capitate and third metacarpal. [View Source / PubMed]
- 47. Filling of any gaps or defects with bone graft of adequate quality and size. Bone from the distal radius may possibly be used but is often insufficient in terms of volume, and harvest may create a cortical defect that interferes with plate fixation. [View Source / PubMed]
- 48. The third carpometacarpal joint must be considered. Ideally, this should also be at least partially excised and grafted so as to remove any movement and provide a continuous bridge of bone across the fusion mass. In this case, a precontoured plate is applied, and an intraoperative decision can be made regarding size, length or bend. Most modern plates have oval hole options that allow initial plate adjustment as well as a later option to apply compression. The distal end of the plate [should reach the mid-shaft or two-thirds of the metacarpal (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark39)**[Figure** ](#bookmark39)**8.9**[). After placing two bicortical non-locking screws proximally and distally to secure the plate, a combination of screws can be used according to requirements including the option of fixation into the carpus. If possible, compression of the fusion mass should be incorporated to promote union. Specific attention should be paid to the relationship between the implant and the extensor tendons as this is a well-recognised cause of postoperative morbidity and re-operation (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark40)**[Figure** ](#bookmark40)**8.10**).  Figure 8.9 AO Wrist fusion plates.    _Closure_ Figure 8.10 Radiographic views of the AO wrist fusion plate. The capsule is approximated as far as possible and closed with an absorbable suture. The extensor retinaculum is closed over the plate if possible – but is not essential. Here, use of the step-cut retinacular exposure is useful. Bowstringing of the extensor tendons due to deficiency in the retinaculum should not be problematic as the wrist is now fixed in a static position. A volar splint is used for 2–6 weeks. Union is usually achieved by 3 months. Surgical technique – partial fusion The ‘four-corner’ fusion (capitate–hamate–triquetrum–lunate fusion) is indicated in scapholunate advanced collapse (SLAC) wrist, scaphoid non-union advanced collapse (SNAC) wrist or mid-carpal instability. The procedure includes a scaphoidectomy and a fusion of the capitate, lunate, hamate and triquetrum. It is vital that the radiolunate joint remains in good condition and capable of function without pain. This should be carefully evaluated preoperatively either radiographically or using wrist arthroscopy. The landmarks, basic approach and structures at risk are similar to those of full wrist fusion. _Incision_ A straight or ‘lazy S’ incision is made over the dorsum of the wrist, again using Lister’s tubercle and the third metacarpal as reference points, although the length of the incision is shorter than that required for a total wrist arthrodesis. _Dissection_ [The extensor retinaculum is exposed in the same way as described for total wrist arthrodesis. Capsulotomy again should allow for visualisation of the radial and ulnar sides of the carpus. A radially or distally based capsulotomy will work well (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark41)**[Figure** ](#bookmark41)**8.11**).                 _Procedure_ Figure 8.11 Exposure of the carpal bones. The soft tissue attachments to the scaphoid are first divided using sharp dissection. The scaphoid is very well attached to soft tissue on its volar and distal aspect. It may be possible to access this from a dorsal approach and undertake a piecemeal scaphoid excision using a joystick K-wire, osteotome and rongeurs. However, a small volar hockey stick incision based over the scaphoid tubercle can facilitate excision of the distal pole and often saves time. Preservation of the excised scaphoid for use as bone graft is possible, but in many cases, the scaphoid is in poor condition and does not provide good quality graft material. The mid-carpal joint is exposed by flexing the wrist, and all cartilage surfaces and sclerotic bone are debrided until healthy cancellous bone is seen. Again, the need for bone graft must be considered especially if a significant resection is needed and there is a risk of reducing the carpal height excessively. Excision of the scaphoid renders the remaining components of the carpus unstable, most notably the mid-carpal joint. There may well also be a degree of pre-existing carpal malalignment. The lunate and mid-carpal joint can be reduced to neutral position using temporary K-wires to maintain the corrected position until definitive fixation is achieved. A range of fixation methods have been described including multiple K-wires and compression staples, but the two most commonly used forms of fixation are either dorsal ‘spider’ plates or intramedullary headless compression screws placed centrally along the axes of the luno-capitate and triquetro-hamate joints. [If a spider plate is being used, the four bones are reduced with temporary wires, and a reamer is used to create a dorsal trough in which the plate will sit and be recessed so as not to cause impingement. Cortical and/or locking screws are used to create compression and stable fixation of the four bones. If headless screws are being used, the mid-carpal joint must be denuded of all articular cartilage until bleeding cancellous bone is seen. Strong ligamentous attachments between capitate and hamate mean that this joint does not necessarily need preparation or stabilization with an implant. If the lunotriquetral ligament remains intact, the same rationale can be applied. Bone graft can be used to fill defects and to maintain carpal height. Again, temporary K-wire stabilization allows placement of guide wires along the central axes of the two columns. Note must be taken of the obliquity of the triquetro-hamate joint in relation to the more horizontally orientated luno-capitate joint. Screw lengths are determined ensuring that the heads are sufficiently buried so as not to cause injury to the surfaces of the lunate fossa or TFCC (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark42)**[Figure** ](#bookmark42)**8.12**).     Figure 8.12 A spider plate. _Closure_ See ‘Surgical technique – full fusion’. _Postoperative care and instructions_ [View Source / PubMed]
- 1. Below-elbow cast immobilisation is recommended for 6 weeks following partial and total wrist fusion. [View Source / PubMed]
- 2. Hand therapy and finger exercises are commenced 1 week after surgery. [View Source / PubMed]
- 3. Union is usually achieved by 3 months. Initially, active mobilisation is undertaken under supervision only. When movement has maximised, strengthening exercises can begin. Recommended references Hooved P. Intercarpal fusions: Indications, treatment options and techniques. _EFORT Open Rev_. 2016;1:45–51. Stewart DT, Froelich JM, Shin AY. Intercarpal arthrodeses. _J Hand Surg Am_. 2014;39(2):373–377. Trail IA, Murali R, Stanley JK et al. The long-term outcome of four-corner fusion. _J Wrist Surg_. 2015;4(2):128–133. [Total wrist arthroplasty](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark21) Total wrist arthroplasty (TWA) is a motion-preserving treatment for pancarpal wrist arthritis. Modern fourth-generation TWA designs are modular, cementless and preserve bone stock with semi-constrained or constrained geometry. _Indications_ [View Source / PubMed]
- 4. Rheumatoid or inflammatory arthritis [View Source / PubMed]
- 5. Osteoarthritis _Contraindications_ [View Source / PubMed]
- 6. Active infection [View Source / PubMed]
- 7. Young, high-demand patients Preoperative planning Plain radiographs including AP and lateral views to assess the wrist. A computed tomography scan is useful for quantifying the bone stock available, the calibre of the metacarpal shafts and the overall alignment of the radial-carpal-metacarpal axis. _Consent and risks_ [View Source / PubMed]
- 1. Periprosthetic fractures [View Source / PubMed]
- 2. Loosening [View Source / PubMed]
- 3. Osteolysis (subsequent requirement for revision) [View Source / PubMed]
- 4. Infection [View Source / PubMed]
- 5. Subluxation/dislocation [View Source / PubMed]
- 6. Complex regional pain syndrome _Anaesthesia and positioning_ General anaesthesia is used. Patient is supine on a radiolucent arm table with application of a tourniquet. Antibiotic prophylaxis is administered. An image intensifier is used. Surgical technique _Incision_ A dorsal longitudinal skin incision is preferred, and the approach to the carpus is in the same manner as described for wrist arthrodesis. _Procedure_ [The specific procedure performed is dependent on the implant design and can be variable, however there are some common principles. The proximal row is excised and the surfaces of the distal radius and distal row are prepared. Surfaces are resected using jigs and cutting blocks based on guide wires placed along the axis of the distal radius and on the opposite side, along the second or third metacarpals. The implant is fixed distally with screws into the carpus and metacarpals. Proximally a press-fit porous coated implant is seated. A polyethylene bearing surface is then implanted forming a semi-constrained, ellipsoidal articulation. Alternative constrained designs are based on intramedullary hydroxyapatite stems in the radius and in the capitate/third metacarpal. These are then connected via a metal on metal bearing surface. In rheumatoid patients, consideration must again be given to the position of the ulna in relation to the carpus and the DRUJ – a distal ulna resection procedure may be required (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark44)**[Figure** ](#bookmark44)**8.13**).       Figure 8.13 Postoperative radiographs of a total wrist arthroplasty. _Closure_ The capsular flap is closed, and the extensor retinaculum is repaired. The image intensifier is used to confirm the position implants. The skin is closed with a subcuticular absorbable monofilament suture. Postoperative care and instructions The wrist is initially splinted for comfort, but the aim should be to commence active movements under the supervision of a hand therapist as soon as pain or soft tissue healing allow. Recommended reference Halim A, Weiss A-P. Total wrist arthroplasty. _J Hand Surg Am_. 2017;42(3):198–209. [Proximal row carpectomy](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark22) Proximal row carpectomy is a salvage procedure for degenerative conditions affecting the radiocarpal joint such as SNAC and SLAC. It involves excision of the proximal row of the carpus – the scaphoid, lunate and triquetrum. The capitate then moves proximally to articulate in the lunate fossa on the distal radius. It has the advantage of being motion sparing, and its success does not rely on the fusion of carpal bones. Its main disadvantages relate to the loss of carpal height which in turn leads to a reduction in grip strength. Also, the radii of curvature of the proximal capitate and proximal lunate are not the same. Therefore, late-stage radiocapitate arthritis is a potential hazard. Prerequisites for this procedure are intact cartilage surfaces of the proximal capitate and lunate fossa of the distal radius. However, if there is doubt regarding the quality of the articular surface, the capsulotomy can be modified to allow for placement of a capsular interposition graft within the lunate fossa. _Indications_ [View Source / PubMed]
- 8. SNAC [View Source / PubMed]
- 9. SLAC [View Source / PubMed]
- 10. Kienbock’s disease (contraindicated if the proximal capitate or lunate fossa are affected by significant degenerative change) _Contraindications_ [View Source / PubMed]
- 11. Active infection [View Source / PubMed]
- 12. Presence of advanced degenerative changes in the lunate fossa or on the proximal pole of capitate Preoperative planning Plain radiographs aretaken including AP and lateral views to assess thejoint surfaces. Magnetic resonance imaging and computed tomography are helpful, but arthroscopic assessment of the wrist provides the most definitive information. Depending on the indication, patient factors and pattern of wear inside the wrist, radioscapholunate fusion and scaphoidectomy with four-corner fusion may also be considered as part of preoperative planning. _Consent and risks_ [View Source / PubMed]
- 1. Injury to superficial radial nerve and dorsal cutaneous branches of the ulnar nerve [View Source / PubMed]
- 2. Loss of grip strength [View Source / PubMed]
- 3. Stiffness and loss of range of movement [View Source / PubMed]
- 4. Arthritis of the capitate and/or lunate fossa of the distal radius _Anaesthesia and positioning_ General anaesthesia is used. Patient is supine on a radiolucent arm table with application of a tourniquet. Antibiotic prophylaxis is administered. An image intensifier is used. Surgical technique _Incision and surgical approach_ The approach is the same as per total wrist fusion. _Procedure_ [When the carpus has been adequately exposed, any remnants of the scapholunate and lunotriquetral ligaments are divided allowing the bones of the proximal row to dissociate from one another. While excising each bone, care must be taken to preserve the volar extrinsic ligaments, and in particular the radioscaphocapitate ligament. This will minimise the risk of ulnar drift of the capitate. Furthermore, iatrogenic injury to the cartilage of the proximal capitate and distal radius must be avoided. The pisiform is not removed. The capitate is guided into its new position in the lunate fossa, and the capsule is closed and tensioned accordingly (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark46)**[Figure** ](#bookmark46)**8.14**).    Figure 8.14 Postoperative radiographs of a proximal row carpectomy showing docking of the capitate into the lunate fossa of the distal radius. Postoperative care and instructions The wrist is immobilised in a cast for 3–4 weeks. A further 2 weeks of immobilisation in a removable thermoplastic splint are recommended, and subsequent range of motion exercises are supervised by a hand therapist. Recommended references Berkhout MJL, Bachour Y, Zheng KH, Mullender MG, Strackee SD, Ritt MJPF. Four-corner arthrodesis versus proximal row carpectomy: A retrospective study with a mean follow-up of 17 years. _J Hand Surg Am_. 2015;40(7):1349–1354. Green DP, Perreira AC, Longhofer LK. Proximal row carpectomy. _J Hand Surg Am_. 2015;40(8):1672–1676. [Excision of the distal ulna](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark23) _Indications_ Pain arising from the DRUJ as a result of [View Source / PubMed]
- 13. Malunion of distal radius or ulna [View Source / PubMed]
- 14. Ulnocarpal impaction [View Source / PubMed]
- 15. Rheumatoid or osteoarthritis affecting the DRUJ [View Source / PubMed]
- 16. Salvage procedure following previously failed DRUJ operative interventions [View Source / PubMed]
- 17. Reserved for patients with low functional demands _Contraindications_ [View Source / PubMed]
- 18. Younger and high-demand patients Distal ulna excision can take one of three different forms: [View Source / PubMed]
- 1. Distal ulna resection (Darrach’s procedure) [View Source / PubMed]
- 2. DRUJ arthrodesis (Sauve-Kapandji procedure) [View Source / PubMed]
- 3. [Distal ulna hemi-resection (Bowers’ procedure) (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark48)**[Figure** ](#bookmark48)**8.15**) (a) (b) (c)  Figure 8.15 Distal ulna excision procedures: (a) Darrach’s procedure, (b) Sauve-Kapandji procedure and (c) Bowers’ procedure. Preoperative planning _Consent and risks_ [View Source / PubMed]
- 1. Outcomes are dependent on primary pathology and operative indication [View Source / PubMed]
- 2. Radioulnar impingement [View Source / PubMed]
- 3. Reduced grip strength [View Source / PubMed]
- 4. Non-union [View Source / PubMed]
- 5. Residual symptoms of pain _Surgical approach to the distal ulna and distal radio ulnar joint_ _Structures at risk_ [View Source / PubMed]
- 1. Dorsal sensory branch of ulnar nerve [View Source / PubMed]
- 2. Ulnar artery and nerve Several approaches to the DRUJ and distal ulna have been proposed. The one described later has the following advantages: [View Source / PubMed]
- 19. Allows minor modifications that preserve the radioulnar ligaments and minimise the risk of TFCC injury [View Source / PubMed]
- 20. Allows good visualisation of the sigmoid notch of the distal radius and thus the DRUJ [View Source / PubMed]
- 21. Allows a DRUJ capsular flap to be raised that can later be used for closure, stabilisation or interposition [View Source / PubMed]
- 22. Preserves the attachment of the ECU subsheath, minimising the risk of instability [View Source / PubMed]
- 23. Provides an exposure suitable for most DRUJ or distal ulna procedures [Patients were placed in a supine position with the limb on a hand table. An above-elbow tourniquet is used. A longitudinal dorsal incision is made between the fifth (EDM) and sixth (ECU) extensor compartments. As the superficial dissection is undertaken, care must be taken not to injure the dorsal sensory branch of the ulnar nerve. The fifth extensor compartment is opened, and the tendon of EDM is retracted. The exposure can be extended by dividing the septa separating the fourth and sixth compartments. This allows the extensor retinaculum to be elevated in both directions, thus exposing the DRUJ capsule and ulnar head below. The capsule is opened by creating a capsular flap that is ulnar based, radially based or oblique. Care must be taken when creating the distal limb of either flap as the dorsal radioulnar ligament and TFCC are at risk (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark49)**[Figure** ](#bookmark49)**8.16**).     Figure 8.16 Approach to the distal ulna. Darrach’s procedure A radially based capsular flap should be used with subperiosteal dissection to expose the ulnar head. The base of the ulnar styloid is osteotomised to allow preservation of the attachment of the TFCC and the dorsal radioulnar ligament. The ulna is osteotomised at its neck and the head excised. The remnant capsule and soft tissues around the distal ulna can then be utilised to stabilise the shaft by use of drill holes or suture anchors. The overlying retinaculum is then closed, but consideration must be made to the tendon of ECU. It may be inherently unstable now that the subsheath is no longer attached to the ulnar head. If this is the case, a slip of extensor retinaculum can be used to fashion a sling, keeping the ECU tendon located dorsally. Postoperative care and instructions Postoperative immobilisation with a wrist splint is maintained for 6 weeks. Early active exercises are encouraged at 2 weeks. Recommended references Darrach W. Partial excision of lower shaft of ulna for deformity following Colles fracture. _Ann Surg_. 1913;57:764–765. De Witte PB, Wujffels M, Jupiter JB, Ring D. The Darrach procedure for post-traumatic reconstruction. _Acta Orthop Belg. 2009;75(3):316–322._ Grawe B, Heincelman C, Stern P. Functional results of the Darrach procedure: A long-term outcome study. _J Hand Surg Am. 2012;37(12):2475–2480._ Mansat P, Bonnevialle N, Ayel J et al. Long-term outcome of distal ulna resection-stabilisation procedures in post-traumatic radio-ulnar joint disorders. _Orthop Traumatol Surg Res_. 2010;96(3):216–221. [Distal radio ulnar joint arthrodesis (Sauve-Kapandji ](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark15)[procedure)](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark15) _Indications_ These are the same as per Darrach’s procedure. Surgical technique The DRUJ is exposed in the same way as previously described via the fifth compartment. Here, exposure of the fourth compartment and retraction of the tendons may facilitate a better view of the sigmoid notch of the distal radius. Also, the ulnar dissection need not be as extensive. And in particular, the TFCC and subsheath attachment of ECU to the ulnar head should be preserved. A capsulotomy is made as before, and the ulnar head is delivered to allow preparation of the articular surfaces. Chondral surfaces are debrided. Use of a small power burr ensures accurate excision of cartilage while preserving bone stock – care must be taken not to over-resect the underlying cancellous bone from both surfaces which may necessitate additional bone grafting. Ensure debris is washed out from the joint surfaces. Under fluoroscopy, compress the prepared ulnar head into the sigmoid notch, and from the lateral subcutaneous border of the ulna pass two percutaneous guide wires for either partially threaded cannulated screws or headless compression screws (of approximately 3 mm diameter). Measure and insert the screws maintaining neutral rotation and good compression of the surfaces. Next, expose the ulnar neck and resect approximately 1 cm of the subcapital bone using an oscillating saw. Protect the surrounding soft tissues throughout. The resulting pseudarthrosis will allow rotational movements to occur below the level of the arthrodesis so that pronation and supination are maintained. Persistent instability of the ulnar shaft is a recognised complication. Several additional procedures have been described that can be undertaken at the same sitting or as late-stage procedures if required. These include stabilising the shaft using a section of mobilised pronator quadratus muscle attached by an anchor or by using a distally based strip of flexor carpi ulnaris tendon that is passed through a drill hole in the shaft and secured. The capsulotomy and retinaculum are closed. The tendon of EDM can be left outside of the retinaculum if the capsule is thin and there is a risk of impingement against the arthrodesis. Postoperative care Keep in an above-elbow cast in neutral rotation for 6 weeks and then in a below-elbow cast until union is achieved. [Distal ulna hemi-resection (Bowers’ procedure)](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark18) _[Indications_ ](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark18) These are the same as discussed earlier. Surgical technique Expose the DRUJ and ulnar head via the floor of the fifth extensor compartment as described earlier. Again, care must be taken to preserve the attachment of ECU, the dorsal limb of the radioulnar ligament and the attachments of the TFCC to the fovea of the distal ulna. An oblique resection of the articular portion of the ulnar head is made, extending from the medial aspect of the head towards the base of the styloid which should be preserved. The edges of the resected ulna should be beveled and smoothed off. The ulnar-based capsular flap can again be sutured to the volar aspect of the sigmoid notch using bone anchors, thus creating a sling that can reduce subsequent ulnar instability. Equally, pronator quadratus can be mobilised from its ulnar insertion and used as an interposition. Wound closure is as previously discussed. Postoperative care Place in an above-elbow cast for 3 weeks in neutral rotation followed by a further 3 weeks in a below-elbow cast before mobilising. [Ulnar shortening osteotomy](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark19) Preoperative planning _Indications_ Ulnar positive variance [View Source / PubMed]
- 24. Acquired [View Source / PubMed]
- 1. Distal radial fracture [View Source / PubMed]
- 2. Essex-Lopresti-type injury [View Source / PubMed]
- 3. Traumatic distal radial growth arrest [View Source / PubMed]
- 4. Congenital [View Source / PubMed]
- 1. Idiopathic ulnar impaction syndrome [View Source / PubMed]
- 2. Madelung deformity (often in conjunction with other procedures) [View Source / PubMed]
- 3. Development of degenerative changes in the TFCC, DRUJ, ulnar head and articular surfaces of the lunate and triquetrum owing to ulnar abutment _Cautions and contraindications_ [View Source / PubMed]
- 25. Malalignment with respect to ulnar inclination and the sigmoid notch [View Source / PubMed]
- 26. DRUJ dysplasia [View Source / PubMed]
- 27. Advanced osteoarthritis or significant malalignment of the DRUJ [View Source / PubMed]
- 28. Smokers (higher incidence of delayed union and non-union) _Consent and risks_ [View Source / PubMed]
- 1. Non-union [View Source / PubMed]
- 2. Delayed union [View Source / PubMed]
- 3. Prominent metalwork and tendonitis from hardware irritation necessitating removal [View Source / PubMed]
- 4. Reduced grip strength: Variable depending on the primary pathology [View Source / PubMed]
- 5. Nerve injury, commonly dorsal sensory branch of the ulnar nerve [View Source / PubMed]
- 6. Compartment syndrome Preoperative planning ‘90/90’ radiographs are obtained (an AP and lateral wrist X-ray taken with the shoulder in 90° abduction and the elbow in 90° flexion). This allows the most accurate estimation of true radioulnar variance. Usually the contralateral side is referred to for comparison. A measurement is made to indicate the amount of shortening required to achieve a final ulnar variance of neutral or −1 mm. A wrist arthroscopy may be performed before an ulnar shortening osteotomy to identify chondral lesions on the proximal lunate or TFCC tears that may benefit from debridement or may guide postoperative recovery. _Anaesthesia and positioning_ Anaesthesia can be general or regional. Use of a tourniquet is recommended. Intravenous antibiotics are administered on induction of anaesthesia. The patient is positioned supine, with a hand table. An image intensifier is used. Surgical technique _Incision_ A longitudinal incision is made along the subcutaneous ulnar border of the ulna starting 3–4 cm proximal to the ulnar styloid. This is extended proximally for approximately 10 cm. _Structures at risk_ [View Source / PubMed]
- 1. The dorsal sensory branch of the ulnar nerve is present at the distal extent of the incision. _Dissection_ [The fascia and muscle fibres of flexor carpi ulnaris (FCU) and ECU blend over the subcutaneous border of the ulna. This interval is incised, and a subperiosteal elevation is undertaken, predominantly on the volar side to mobilise FCU and expose the ulnar shaft. Care must be taken as the ulnar neurovascular bundle lies on the radial side of the tendon and is at risk. Hohmann retractors are placed around the ulna to retract the muscle of FCU and expose the volar side of the ulnar shaft. This will allow placement of the plate on the flat surface of the ulnar shaft and ensure that it remains flush with the lateral border of the bone. The plate will sit under the muscle of FCU, and the likelihood of painful metalwork prominence will be reduced (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark53)**[Figure** ](#bookmark53)**8.17**).              Figure 8.17 Approach between the extensor carpi ulnaris and flexor carpi ulnaris. _Procedure_ Numerous ulnar shortening systems are available. Each manufacturer and implant has a recommended technique, but they share common principles. The ulnar plate is positioned, initial screw holes are drilled and cortical screws are used to secure the plate to the bone. A cutting block is then applied through which an initial oblique cut is made with an oscillating saw while the plate remains _in situ_[. This ensures that control and stability of the bone can be maintained throughout the procedure. The cutting block can then be accurately advanced by a predetermined distance according to the length of resection required. A second parallel bone cut is made, and a wedge of ulnar shaft is excised. Care must be taken to protect the soft tissues when using the saw. Copious irrigation must also be used to reduce the risk of thermal injury to the bone surfaces. The osteotomy system will then allow the gap to be closed and the ends of the bone compressed. An oblique lag screw and additional shaft screws ensure compression and rigid fixation (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark54)**[Figure** ](#bookmark54)**8.18**). (a) (b) (c)                    Figure 8.18 Surgical technique for ulnar shortening using a dynamic compression plate. _Closure_ Avoid a tight closure of the fascia overlying the flexor compartment. Standard closure of the skin in layers is undertaken. A cast is not required but may be applied for comfort. Postoperative care and instructions The fixation is strong enough to support early active movement within the limits of the patient’s comfort with no specific restrictions in terms of forearm rotation or wrist or elbow movement. Recommended references Chen NC, Wolfe SW. Ulna shortening osteotomy using a compression device. _J Hand Surg Am_. 2003;28:88. Chun S, Palmer AK. The ulnar impaction syndrome: Follow up note of ulnar shortening osteotomy. _J Hand_ _Surg Am. 1993;18:46–53._ Fulton C, Grewal R, Faber KJ, Roth J, Gan BS. Outcome analysis of ulnar shortening osteotomy for ulnar impaction syndrome. _Can J Plast Surg_. 2012;20(1):e1–e5. Nagy L, Jungwirth-Weinberger A, Campbell D, Pino JG. The AO ulnar shortening osteotomy system indications and surgical technique. _J Wrist Surg_. 2014;3(2):91–97. Tatebe M, Nishizuka T, Hirata H, Nakamura R. Ulnar shortening osteotomy for ulnar-sided wrist pain. _J Wrist Surg. 2014:3(2):77–84._ [Trapeziectomy](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark24) The first carpometacarpal joint (CMCJ) is a biconcave saddle joint and can be considered to be composed of several joints forming a complex articulation – the trapezium-metacarpal, trapezium-trapezoid and scapho-trapezium-trapezoid (STT) joints. Basilar thumb arthritis is common and is thought to be caused by a combination of anatomic and biologic factors. Trapeziectomy is a well-described procedure that is essentially an excision arthroplasty. The trapezium in its entirety may be excised leading to an improvement in pain. There is no single best technique, and a multitude of variations have been proposed. The greatest controversy surrounds the use of additional procedures to augment the stability of the first metacarpal. These ‘ligament reconstruction’ procedures aim to restore the subluxed and adducted first metacarpal to a more functional position after the trapezium has been excised. In theory, they also aim to provide a greater restraint to axial loading of the first metacarpal. However, their effectiveness is much debated. The following description is an overview of a simple trapeziectomy undertaken through a dorsal approach. A volar approach has also been described and may be used, again with a multitude of variations. _Indications_ [View Source / PubMed]
- 1. Severe CMCJ arthritis [View Source / PubMed]
- 2. Pain refractory to analgesics, corticosteroid injections, hand therapy and splintage _Contraindications_ [View Source / PubMed]
- 3. Active infection [View Source / PubMed]
- 4. Uncertain diagnosis – consider other causes of radial-sided wrist/hand pain including de Quervain’s tenosynovitis Preoperative planning Clinical examination demonstrates CMCJ swelling, crepitus on movement and first metacarpal adduction with compensatory development of metacarpophalangeal joint hyperextension resulting in a Z-thumb posture. In cases where there is pan-trapezial arthritis and STT involvement, residual pain from the arthritic scapho-trapezial joint may persist after the trapezium has been excised. _Consent and risks_ [View Source / PubMed]
- 1. Superficial radial nerve injury [View Source / PubMed]
- 2. Radial artery injury [View Source / PubMed]
- 3. Flexor carpi radialis tendon injury [View Source / PubMed]
- 4. Shortening of the thumb [View Source / PubMed]
- 5. Infection [View Source / PubMed]
- 6. Persistent pain [View Source / PubMed]
- 7. Loss of grip strength _Anaesthesia and positioning_ General or regional anaesthesia is used. The patient should be in supine position, hand placed on an arm extension with application of an above-elbow tourniquet. Surgical technique Landmarks for the dorsal approach are identified. The subluxed base of the first metacarpal is often easily identified, especially when passively moved. However, the metacarpal base overhangs the trapezium which is not readily palpated. The next identifiable bony structure is the tip of the radial styloid. The tendons of the first extensor compartment may be palpable between the two. A skin incision is made centered over the trapezium. Branches of the superficial radial nerve are identified, mobilised and protected throughout. The APL and EPB tendons are mobilised and retracted. At this stage the surgeon may choose to identify and protect the radial artery to avoid injury during further exposure of the joint. This lies dorsally and may be retracted with use of a vessel loop taking care to cauterise any side branches. The presence of significant degenerative change may hamper easy identification of the trapezio-metacarpal joint. One way to overcome this is to apply axial traction to the metacarpal in order to correct the subluxation and uncover the joint that may be obscured by the metacarpal base. Again, a multitude of capsulotomies have been described, but a simple longitudinal capsulotomy is described here. Begin the capsulotomy with subperiosteal dissection at the metacarpal base – this will allow easier confirmation of the joint location. Continue the longitudinal capsulotomy to the level of the scapho-trapezial joint so that the proximal and distal margins of the trapezium are under direct vision. A combination of sharp dissection and the use of a periosteal elevator can allow for capsular flaps to be raised on either side of the arthritic joint. In order to aid this, a K-wire or corkscrew device may be placed into the trapezium in order to allow it mobilisation and retraction. The FCR tendon is well attached to the trapezium as it passed through a fibro-osseous tunnel on its volar aspect. Care must be taken during the dissection and during trapezial excision not to injure the FCR. The trapezium may be excised as a single piece or more commonly piecemeal by fracturing it into halves or thirds with an osteotome. It is particularly important to remove the dorsal osteophyte between the first and second metacarpals. This may not be readily visible within the wound and so the surgeon must take steps to identify and excise this fully. The stability of the first metacarpal may then be assessed. Many ligament reconstruction techniques utilise the nearby tendons of FCR or APL which can be easily harvested. Increasingly, synthetic tape, bone anchors, biotenodesis screws or tightrope devices are also used in the ligament reconstruction or ‘suspensionplasty’ process. Wound washout is important to ensure that joint debris is not retained. The capsule is closed and a final check is made of the radial artery and its branches. Postoperative care and instructions Immobilise the wrist in a thumb spica for 2–4 weeks. The patient may benefit from further support in a thermoplastic splint as range of motion exercises are commenced under the supervision of a hand therapist. Recommended references Croog A, Rettig M. Newest advances in the operative treatment of basal joint arthritis. _Bull NYU Hosp Jt Dis_. 2007;65(1):78–86. Gangopadhyay S, McKenna H, Burke FD, Davis TRC. Five- to 18-year follow-up for treatment of trapeziometacarpal osteoarthritis: A prospective comparison of excision, tendon interposition, and ligament reconstruction and tendon interposition. _J Hand Surg Am_. 2012;37(3):411–417. Vermeulen GM, Slijper H, Feitz R, Hovius SER, Moojen TM, Selles RW. Surgical management of primary thumb carpometacarpal osteoarthritis: A systematic review. _J Hand Surg Am_. 2011;36(1):157–169. [Surgery for scaphoid ](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark25)[non-union](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark25) The scaphoid is particularly susceptible to fracture and subsequent non-union due to a range of biologic and anatomic factors. Fractures of the scaphoid waist are most common and therefore waist non-union is the most prevalent. However, proximal pole fractures although seen less commonly have a higher incidence of progression to non-union. This section focuses on the surgical treatment of a recognised, established scaphoid non-union using non-vascularised bone graft. _Indications_ [View Source / PubMed]
- 5. Established scaphoid non-union recalcitrant to non-operative treatments [View Source / PubMed]
- 6. Lack of radiographic union after 6 months’ post-fixation _Contraindications_ [View Source / PubMed]
- 7. Development of SNAC wrist and widespread arthritis [View Source / PubMed]
- 8. Non-reconstructable scaphoid Preoperative planning History and clinical examination will lead the surgeon to suspect a scaphoid fracture or non-union, but confirmation of the diagnosis will come from imaging. Scaphoid series X-rays are an essential starting point. However, CT and MRI can provide additional information. The surgical plan will be affected by several key factors. Distal pole fractures are best approached from the volar side. If a tubercle fracture remains non-united it may be excised, whereas larger distal fragments may be fixed internally. In the acute setting, scaphoid waist fractures may be approached from either a volar or dorsal approach. However, when considering non-union surgery, a volar approach is recommended. The classic ‘humpback’ deformity occurs as the non-united scaphoid fragments flex and collapse. This is often associated with osteolysis and cavitation on the volar surface that will need to be adequately visualised and corrected – something that is rarely possible from a dorsal approach. _Consent and risks_ [View Source / PubMed]
- 1. Delayed union [View Source / PubMed]
- 2. Persistent non-union [View Source / PubMed]
- 3. Wrist stiffness and loss of range of movement [View Source / PubMed]
- 4. Vascular injury – radial artery [View Source / PubMed]
- 5. Neurologic injury – palmar cutaneous branch of the median nerve (runs along the ulnar side of FCR) _Anaesthesia and positioning_ General or regional anaesthesia is used. Patient is supine on a radiolucent arm table with application of a tourniquet. Antibiotic prophylaxis is administered. An image intensifier is used. Surgical technique _Landmarks_ [View Source / PubMed]
- 9. Scaphoid tubercle [View Source / PubMed]
- 10. Tendon of FCR _Incision_ A hockey stick incision is made centred on the scaphoid tubercle. Proximally the incision follows the line of the FCR tendon. On reaching the tubercle it is angled along the line of the first metacarpal. If a distal radius bone graft is planned, the proximal limb is lengthened. _Procedure_ Develop an interval between the FCR tendon the radial artery. Retract the FCR in an ulnar direction and the artery radially. Incise the floor of the sheath. Identify the tubercle again and expose the radioscaphocapitate (RSC) and long radiolunate (LR) ligaments. These are essentially condensations in the fibres of the volar capsule. Distally, origins of thenar muscle can be divided to allow exposure of the scapho-trapezial joint. This must be adequately exposed to allow for accurate placement of the guidewire for headless screw fixation. In this ‘ligament splitting’ technique, the volar capsule and hence the RSC and LR ligaments are divided longitudinally. More recently, ligament-preserving techniques have also been described that essentially take a zigzag path across these structures to expose the volar scaphoid. The scaphoid non-union is identified and cleared of fibrous tissue. Numerous techniques have been described for volar wedge grafting of a non-united scaphoid, but they all share common themes. Sclerotic bone must be excised, cavitation must be curettaged and debridement must be taken back until healthy punctate bleeding points are seen within the bone. The length and alignment of the scaphoid are restored – either joystick K-wires or a small laminar spreader are used to maintain the corrected position and an estimation is made of the size of graft required. The most common donor sites are the distal radius and iliac crest. If the distal radius is to be used, the dissection between FCR and the radial artery is continued proximally, and the pronator quadratus is elevated off the volar surface of the radius. Four points of a square or rectangle matching the shape of the graft required are marked on the volar radius. Each of these points is then drilled using a small-diameter drill bit or a K-wire to prevent crack propagation. A fine sagittal saw or small sharp osteotome is used to fracture the volar cortex. If care is taken, a cortico-cancellous wedge can be removed as a single piece. Using a gauge, additional cancellous bone can be harvested. Cavities in either end of the scaphoid are packed with graft, and the cortico-cancellous wedge is impacted into the central defect. A trough is made in the volar aspect of the trapezium at the level of the scapho-trapezial joint. This will allow better exposure of the central point of the distal scaphoid that marks the ideal entry point for the guide wire. The wire is passed along the central axis of the scaphoid and checked with fluoroscopy. This is measured and a screw inserted. As a rule of thumb, the length of screw used is approximately 4 mm shorter than the length measured. This allows for the screw to be buried under articular cartilage, accounts for a degree of compression and minimises the chance of screw prominence. _Closure_ Haemostasis is achieved after tourniquet release and closure of the volar capsule using interrupted Vicryl sutures. The skin is closed with a subcuticular absorbable monofilament suture. Postoperative care and instructions The wrist is immobilised in a cast, with or without thumb spica for 6–8 weeks. Follow-up radiographs or CT are used to assess progression of healing. Recommended references Moon ES, Dy CJ, Derman P, Vance MC, Carlson MG. Management of nonunion following surgical management of scaphoid fractures: Current concepts. _J Am Acad Orthop Surg_. 2013;21(9):548–557. Pinder RM, Brkljac M, Rix L, Muir L, Brewster M. Treatment of scaphoid nonunion: A systematic review of the existing evidence. _J Hand Surg Am_. 2015;40(9):1797–1805.e3. _[Viva questions_ ](file:///C:/Users/DELL/Desktop/hip/quick%20fact/8.%20Surgery%20of%20the%20Wrist_Converted.html#bookmark26) [View Source / PubMed]
- 1. Give a histologic definition of a cyst. [View Source / PubMed]
- 2. What are the other sites for cystic swellings in the wrist and hand? [View Source / PubMed]
- 3. Talk through an excision of a ganglion cyst. [View Source / PubMed]
- 4. What is the risk of recurrence post-excision? [View Source / PubMed]
- 5. How many dorsal compartments are found at the wrist and what are their contents? [View Source / PubMed]
- 6. Which nerve and artery are at risk during surgical release of the first dorsal compartment? [View Source / PubMed]
- 7. What is the optimal position for wrist arthrodesis? [View Source / PubMed]
- 8. Between which dorsal wrist compartments do you classically approach through to access the wrist joint? [View Source / PubMed]
- 9. What is a ‘four-corner’ fusion? [View Source / PubMed]
- 10. Name and describe the common wrist arthroscopy portals. [View Source / PubMed]
- 11. Dorsal wrist ganglions usually arise from which ligament? [View Source / PubMed]
- 12. Describe the radiographic features of a wrist with scapholunate advanced collapse. [View Source / PubMed]
- 13. What is the non-union rate in total wrist fusions? [View Source / PubMed]
- 14. What are the main functional disadvantages with Darrach’s procedure? [View Source / PubMed]
- 15. What alternatives are there to Darrach’s procedure in younger and higher-demand patients? [View Source / PubMed]
- 16. What is complex regional pain syndrome? What is the incidence after wrist or hand procedures? [View Source / PubMed]
- 17. When should an ulnar shortening osteotomy not be performed? [View Source / PubMed]
- 1. What is the most significant factor influencing the rate of non-union in an ulnar shortening osteotomy? [View Source / PubMed]
- 2. What is the significance of the posterior interosseous nerve in wrist procedures? [View Source / PubMed]
- 3. Where is the posterior interosseous nerve identified at the wrist? [View Source / PubMed]
- 4. What is a proximal row carpectomy? [View Source / PubMed]
- 5. What is the pathophysiology of CMCJ arthritis? [View Source / PubMed]
- 6. Describe the volar approach to the scaphoid. [View Source / PubMed]
