Surgery of the
Thoracolumbar Spine
Thoracic spine
Lumbar spine
43
53
Viva questions
60
Daniel P Ahern, Joseph S Butler, Matthew Shaw and Sean Molloy
Thoracic spine
Posterior thoracic surgery
Scoliosis correction
Choice of approach
1. There is an increasing trend towards posterior-only surgery. However, much depends on the characteristics of the curve and on the surgeon’s training and preference.
2. Thorough discectomy is only possible with an anterior approach; thus very stiff curves may benefit from anterior release prior to posterior surgery.
3. Thoracolumbar/lumbar curves are often treated with anterior instrumentation, especially if there is no thoracic curve.
4. Posterior instrumentation allows fixation to the pelvis – an advantage in long fusions in the elderly and in non-walking patients with neuromuscular-type curves.
Indications
5. Severe deformity
6. Curve progression
7. Radicular pain or neurological deficit (degenerative cases)
8. Back pain failing conservative measurement (rare)
Risks
9. Mortality 0.03%
10. Respiratory dysfunction
11. Neurological deficit: complete 0.03%; incomplete 1.5%
12. Revision surgery 5%
13. Failure to achieve complete curve correction
14. Damage to sympathetic chain, major vessels
15. Infection 1%–2%
16. Blood loss







Figure 4.1 A thoracic flexion compression fracture with kyphosis.
17. Scar
18. Imbalance, shoulder height discrepancy
19. Back pain
20. Blindness 0.028%–0.2%
Operative planning
21. Full history and examination
22. Full spine radiographs including bending films:
1. Bending films to assess flexibility of spine
2. Identifying the correct level in the thoracic spine is more of a challenge as the reference points of the sacrum or C2 are not available. Therefore, it is important to check the number of ribs a patient has on plain X-ray, as these can be used to mark the skin using fluoroscopy prior to incision
23. Whole spine MRI
24. Multidisciplinary team involvement
25. Anaesthetic and medical workup
26. Lung function tests, chest radiograph, electrocardiogram (ECG)
27. Cord monitoring arrangement
28. Intensive care unit (ICU) bed arranged

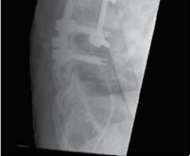


Figure 4.2 Thoracic vertebrectomy with posterior stabilisation for a solitary metastasis.
Surgical procedure
29. General anaesthesia
30. Prone positioning:
1. Montreal mattress, Jackson table, four-post frame or similar
2. Arms can be placed by the patient’s side or out in front (depending on the level of surgery and the need to use X-ray)
31. Protect pressure areas, eyes:
1. It is important that the shoulders are not hyperflexed or abducted and there is no pressure on the axilla, which could cause a nerve palsy
2. Padding is used under the patient’s elbows to avoid an ulnar nerve palsy
3. No pressure on the eyes
4. Table should be slightly head up to decrease central venous pressure
32. Mechanical deep vein thrombosis prophylaxis
33. X-rays on display
34. Incision:
1. Skin:
1. Note the pedicle entry point will be above the spinous process of the vertebra counted and therefore the skin incision should allow for this
35. Dissection:
1. Subcutaneous fat and fascia
2. Spinous process identified and subperiosteal dissection:
1. Ensure haemostasis – diathermy, gauze packing
3. Dissection to identify transverse processes, medial and lateral borders of the facet joints, and the pars
36. Pedicle screw insertion:
1. In general, at the junction of the medial two-thirds and lateral one-third of the facet joint
37. Decortication of facets and lamina
38. Reduction
39. Rod insertion
• +/− Cross-links
40. Closure in layers
• +/− Drain insertion
Postoperative care
41. Neurovascular observations and analgesia
42. Postoperative haemoglobin and renal function
43. No spinal precautions – mobilise as pain allows
44. Postoperative full spine X-rays
Posterior thoracic decompression and fusion
Indications
45. Unstable thoracic fracture
46. Posterior cord compression from a tumour or degenerative process
47. Palliative procedure from an anterior compressive pathology
1. Where patient condition does not allow for anterior approach
48. Disc pathology as part of costotransversectomy
49. Coronal or sagittal deformity correction
Risks
50. Mortality
51. Infection: 2%
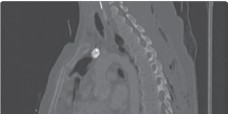
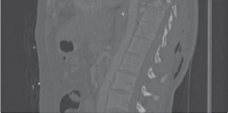


Figure 4.3 A fracture dislocation of the thoracic spine stabilised with posterior thoracic rods and screws.
52. Neurological injury
1. Higher rate in the thoracic spine as canal dimensions smaller
53. Wrong level surgery
1. Higher rate in thoracic spine – reference points of C2 and sacrum not available
54. Blindness 0.02%–0.2%
55. Thromboembolism
56. Respiratory infection
57. Failure/fracture of fixation
Operative planning
58. Full history and examination
59. Radiographs/computed tomography (CT)/magnetic resonance imaging (MRI)
60. Anaesthetic and medical workup/optimisation as appropriate
Surgical procedure
61. General anaesthesia
62. Prone positioning
1. Montreal mattress, Jackson table, four-post frame or similar
63. Arm positioning
1. May be placed on patient’s side or out in front
1. Dependent on level of surgery and use of intraoperative imaging
2. Beware not to hyperflex or abduct when position arms overhead (less than 45° abducted and less than 90° hyperflexed)
64. Pressure area padding
65. Midline incision
66. Dissection
1. Skin, fat and fascia with haemostasis control
67. Paraspinal musculature stripped from spine
68. Dissection for landmark identification
1. Transverse processes, medial and lateral borders of the facet joints and the pars
T2/3 T3/4
T4/5
T2 T3
T5
T7
T2 Superior border of scapula. T2/3 Suprasternal notch.
T3 Medial end of spine of scapula. Spine of T3 is posterior end of oblique fissure lung.
T3/4 Top of arch of aorta.
T4 End of arch of aorta. Azygos vein enters SVC.
T4/5 Manubriosternal junction. (Angle of Louis.) Start of arch of aorta. T5 Thoracic duct crosses midline.
T7 Inferior angle of scapula.
T8 Caval opening in diaphragm. (IVC & right prenic nerve.) Left phrenic
T8
T10 T12
pierces diaphragm. Hemi-azygos veins cross to left.
T10
Oesophageal opening in diaphragm (oesophagus, branches of left
gastric vessels, vagus nerves).
T12 Aortic opening in diaphragm. (Aorta, azygos vein, hemi-azygos vein, thoracic duct.) Coeliac axis.
Splanchic nerves pierce crura. Sympathetic trunk passes behind medial arcuate ligament. Subscostal bundle passes behind lateral arcuate ligament.








Figure 4.4 Thoracic structures corresponding to various vertebral levels.
Pleura over oesophagus
Pleura over azygos vein
Pleura over intercostal
vein
Incision in pleura
Intercostal
muscle
Pleura over medial end of rib
Pleura over paravertebral ganglion
External suface of retracted rib










Figure 4.5 The selection of rib level in anterior scoliosis surgery.
69. Pedicle screw insertion
1. Medial and lateral borders of the facet joints give the medial and lateral starting points for the pedicle screws
2. In craniocaudal direction, pedicle screw direction is approximately 90° to the translamina line
70. Decompression
1. After instrumentation gives more protection to the neural elements than during instrumentation
• +/− Drain insertion
71. Closure in layers
Postoperative care
72. Adequate analgesia
73. Neurological observations including formal postoperative neurological examination
74. No spinal precautions – patient allowed to sit to any angle and mobilise as pain allows
75. Postoperative radiographs
Anterior thoracic surgery Scoliosis (anterior release)__Indications
76. Same as posterior procedure
1. Severe deformity
2. Curve progression
3. Radicular pain or neurological deficit (degenerative cases)
4. Back pain failing conservative measurement (rare)
Risks
77. Mortality 0.03%
78. Respiratory dysfunction
79. Neurological deficit: complete 0.03%; incomplete 1.5%
80. Revision surgery 5%
81. Failure to achieve complete curve correction
82. Damage to sympathetic chain, major vessels, thoracic duct
83. Infection 1%–2%
84. Blood loss
85. Scar
86. Imbalance, shoulder height discrepancy
87. Back pain
Operative planning
88. Full history and examination
89. Full spine radiographs including bending films
1. Bending films to assess flexibility of spine
90. Whole spine MRI
91. Multidisciplinary team involvement
92. Anaesthetic and medical workup
93. Lung function tests, chest radiograph, ECG
94. Cord monitoring arrangement
95. ICU bed booked
Surgical procedure
96. General anaesthetic
97. Lateral position
1. Convexity of the curve facing upwards
98. Pressure areas padded
99. Incision
1. In line with proposed rib
2. Note that rib level to be entered should be two levels above the superior vertebra being instrumented due to downward slope of ribs
100. Dissection
1. Skin, fat and muscle are incised in line with the rib
2. Maintain haemostasis
101. Periosteum stripped off the rib as far posteriorly as possible
102. Anteriorly, rib is exposed to costochondral junction, then cut and removed
103. Expose and carefully incise pleura and expose lung
104. Retract lung superiorly using wet packs
105. Posterior pleura is then incised
106. Beware underlying segmental vessels
107. If procedure is to cross the thoracolumbar junction, the diaphragm will need to be taken down
1. Before or after entering pleural cavity, costal cartilage is incised
2. Abdominal musculature is divided inferomedially – Beware risk of damage to peritoneum
3. Retroperitoneal fat entered deep to the costal cartilage
4. Peritoneum is reflected anteriorly using blunt finger dissection/gauze swabs
5. Dissection is carried down to the spine, anterior to the psoas muscle
6. Diaphragm is divided (with electrocautery) – A 2 cm peripheral cuff is left for repair
7. Great vessels and viscera are carefully reflected anteriorly and protected with blunt retractors throughout procedure
108. Once exposure is complete, individual segmental vessels can be tied, cauterised or preserved
109. Disc material is removed piecemeal until posterior longitudinal ligament is visualised
110. Cartilaginous end plates are removed using a Cobb, osteotome or curette
1. Ideally, bony end plates should not be breached as this markedly increases blood loss
111. Instrumentation
1. Important to appreciate rotation of the curve and relationship of vertebral body to spinal canal
2. Achieving a ‘cadence’ of screw insertion with the apical screw being most posterior will assist in de-rotation of the spine
3. Bicortical fixation aids stability
112. Following screw insertion, a rod is applied
113. Reduction
114. Screw and rods are applied to the convexity of the curve; therefore, compression between individual screws aids reduction
115. Closure
1. Posterior pleura may be left open or closed – surgeon preference
2. Diaphragmatic repair
3. Chest wall closed in layers
4. Chest drain inserted
5. Superficial closure
Postoperative care
116. Neurovascular observations and analgesia
117. Postoperative haemoglobin and renal function
118. No spinal precautions – mobilise as pain allows
119. Postoperative full spine X-rays
Thoracic discectomy+ /− corpectomy
Indications
120. Disc prolapse
121. Other compressive pathologies
1. Fracture
2. Tumour
Risks
122. Mortality less than 1%
123. Respiratory infection









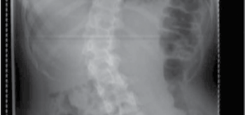

Figure 4.6 Anterior scoliosis correction.
124. Anterior chest wall pain
125. Major vessel damage 2%–15%
126. Neurological compromise
127. Cosmesis of scar
128. Thromboembolism less than 1%
129. Back pain
130. Wrong level surgery
Operative planning
131. Full history and physical examination
132. Imaging – radiographs, CT, MRI
133. Anaesthetic and medical workup/optimisation
134. Appropriate cardiothoracic/vascular backup available
Surgical procedure
135. General anaesthesia
136. Lateral position
1. Sand or bean bag commonly placed underneath operative site to aid exposure and open disc spaces
2. Pressure areas padded
137. Incision
1. In line with proposed rib
2. Note that rib level to be entered should be two levels above the superior vertebra being instrumented due to downward slope of ribs
138. Dissection
1. Skin, fat and muscle are incised in line with the rib
2. Maintain haemostasis
139. Periosteum is dissected off the rib and rib freed circumferentially from underlying soft tissue
140. Rib cutters are used to remove the rib
141. Underlying pleura carefully incised and lung protected with a chest pack
142. Rib spreader is positioned to optimise exposure
143. Posterior pleura incised and plane developed between segmental blood supply







Figure 4.7 Posterior scoliosis correction.
144. Segmental blood vessels may be tied, cauterised or preserved
145. Discs are incised and removed piecemeal
146. Cartilaginous end plates are removed (aiding fusion)
147. Thoracic corpectomy
1. Discs above and below the vertebra in question are removed
2. Vertebral body is cut and removed piecemeal
3. Implant positioning
148. Closure
1. Chest drain insertion
2. Chest wall closed in layers
3. Superficial closure
Postoperative care
149. Neurovascular observations and analgesia
150. Postoperative haemoglobin and renal function
151. No spinal precautions – mobilise as pain allows
152. Postoperative chest and spine X-rays
Lumbar spine
Posterior lumbar surgery Microdiscectomy Indications
153. Acute disc prolapse symptomatic following 6 weeks non-operative measures
154. Earlier surgery if
1. Features of cauda equina syndrome
2. Neurological deficit
3. Intractable pain
Risks
155. Nerve root injury: 1%
156. Epidural haematoma
157. Dural tear: 5%
158. Infection: 1%–2%
159. Wrong level surgery: Less than 1%
160. Cauda equina: 0.01%
161. Dural tear
162. Ongoing pain
163. Post-discectomy instability leading to lower back pain
164. Blindness
Operative planning
165. Full history and physical examination
166. MRI lumbar spine
167. Plain X-ray lumbar spine
1. Useful for assessing transition levels in lumbar sacral spine
T3
T7
L4 S2




Figure 4.8 Anatomical levels in the lumbar spine.
Surgical procedure
168. General anaesthesia
169. Positioning
1. Prone on Montreal mattress, Wilson frame, or Jackson table
2. ‘Knees-to-chest’ prone position
170. Skin prep
171. Level check
1. Needle into estimated level
2. Cross-table lateral radiograph
3. Needle adjusted until inserted onto spinous process of correct level
172. Midline incision
173. Dissection
1. Fat, fascia
2. Diathermy used to dissect the musculature off the posterior elements of the spine
3. Soft tissue swept laterally using a Cobb elevator
174. Identification of landmarks
1. Lamina of vertebra above
2. Inferior edge delineated
175. Ligamentum flavum identified and incised
176. Level check recommended
177. Development of interlaminar window
1. Important not to remove more than one-third of facet so as not to develop instability
178. Careful exposure of dura
179. Identification and protection of nerve root
1. Using nerve root retractors
180. Incision of posterior longitudinal ligament
1. If intact; with large disc prolapses, disc will have ‘broken through’ this layer
181. Incision of disc and piecemeal removal
182. Washout with saline
183. Closure in layers
184. Skin closure
Postoperative care
185. Adequate analgesia
186. No spinal precautions
187. Postoperative neurological examination
Posterior lumbar decompression+ /− fusion
Indications
188. Lumbar spine trauma
189. Spondylolisthesis
190. Spinal stenosis
191. Degenerative deformities
Risks
192. Nerve injury: 1%
193. Cauda equina injury: 0.1%
194. Infection 1%–2%
195. Venous thromboembolism: 1%
196. Persistence/worsening of symptoms: 5%–10%
197. Non-union: 5%
198. Dural tear
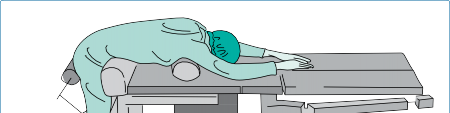

Figure 4.9 The knees-to-chest position for lumbar discectomy.
Operative planning
199. Full history and physical examination
200. Plain X-rays
1. Deformity evaluation
2. Baseline for levels intraoperatively
201. MRI lumbar spine
202. Single-photon emission computed tomography lumbar spine
203. Anaesthetic and medical optimisation
Surgical procedure
204. General anaesthesia
205. Prone position
1. Montreal mattress or Jackson frame
2. Pressure area padding
206. Skin prep
207. Level check
1. Needle into estimated level
2. Cross-table lateral radiograph
3. Needle adjusted until inserted onto spinous process of correct level
208. Midline incision
209. Dissection
1. Fat, fascia
2. Diathermy used to dissect the musculature off the posterior elements of the spine
3. Soft tissue swept laterally using a Cobb elevator
210. Identification of landmarks for instrumentation/pedicle entry points
1. Pars
2. Junction of the transverse process and facet
3. Continue soft tissue dissection until transverse process clearly seen
211. Level check
212. Pedicle screw insertion
1. At the confluence of the pars, transverse process and facet
213. Rod application
214. Decompression
1. Laminectomy
2. Burr and osteotome
3. Nerve roots identified and explored
4. Undercutting facetectomy
1. Ensure nerves are decompressed both in lateral recesses and foramen
215. If dural leak occurs (5%)
1. Repair using 5.0 Prolene
2. Blood, fascia or fat patches
3. Dural ‘glues’
4. Maintain supine for 48 hours postoperatively
216. Closure in layers
Postoperative care
217. Adequate analgesia
218. Neurological observations and formal neurological assessment
219. No spinal precautions
Transforaminal lumbar interbody fusion and posterior lumbar interbody fusion
Indications
220. Isthmic and degenerative spondylolisthesis
221. Discogenic back pain
222. Post-discectomy pain syndromes failing conservative management
Risks
223. Nerve injury
224. Infection
225. Pseudarthrosis
226. Persistence of symptoms following non-operative management
Operative planning
227. Full history and physical examination
228. X-ray
229. MRI
Surgical procedure
230. General anaesthesia
231. Prone position
232. Montreal mattress, Jackson table, four-poster frame
233. Midline incision
234. Dissection
1. Fat, fascia
2. Diathermy used to dissect the musculature off the posterior elements of the spine
3. Soft tissue swept laterally using a Cobb elevator
1. Unilaterally – transforaminal lumbar interbody fusion (TLIF)
2. Bilaterally – posterior lumbar interbody fusion (PLIF)
235. Identification of landmarks
1. Transverse processes
236. Pedicle screw insertion
237. Resection of superior and inferior articular processes of identified facet joint (TLIF) or laminotomy (PLIF)
238. Exposure of disc
1. Ensure haemostasis of epidural veins running superior to the pedicle in the neuroforamen
239. Piecemeal disc removal
240. Cartilaginous endplate removal
241. Cage insertion +/– bone graft
242. Rod application (under slight compression)
243. Closure in layers
Postoperative care
244. Adequate analgesia
245. Neurological observations and formal neurological assessment
246. Postoperative X-rays
247. No spinal precautions
Minimally invasive spinal surgery
New, less invasive techniques have and are continually developed in relation to the above procedures due to technological advances in access instrumentation and visualisation, as well as a desire to reduce approach-related comorbidities.
Indications
248. Degenerative disc diseases
249. Spinal stenosis
250. Trauma
251. Curvatures
252. Pseudoarthrosis
253. Tumour
Risks
254. Increased operative length
Operative planning
255. Full history and physical examination
256. Spinal imaging
1. Plain X-rays
2. CT spine
3. MRI spine
Surgical procedure
257. General anaesthetic
258. Prone position
259. Sterile prep and drape with fluoroscopy/navigation system
260. Approach consists of multiple
1. Stab incision at desired angle from midline
2. Guidewire to posterior elements of spine
3. Sequential dilators or pedicle screw guide
1. Guidewire removed after first dilator to prevent advancement
4. Dilated retractor allows adequate visualisation of bony elements for decompression, discectomy, etc.
Anterior lumbar surgery Anterior lumbar interbody fusion Indications
261. Degenerative disk disease
262. Discogenic disk disease
263. Revision of failed posterior fusion
Risks
264. Approach-related complications
1. Retrograde ejaculation
2. Vascular injury
3. Visceral injury
265. Infection
266. Persistent pain
Operative planning
267. Full history and examination
268. Comprehensive surgical history (previous abdominal surgery)
269. Plain X-rays
270. MRI
Surgical procedure
271. General anaesthetic
272. Supine position
273. Incision
1. Pfannenstiel
2. Paramedian
3. Lower midline
Ascending articular process
Descending
articular process of proximal vertebra
Cauda equina
Spinal nerve
Herniated disc
Posterior longitudinal ligament
(with overlying veins)










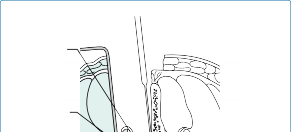

Figure 4.10 The operative view in lumbar discectomy.
274. Retroperitoneal dissection
275. Identification of
1. Iliac arteries and veins
2. Aortic bifurcation
3. Vena cava
276. Mobilisation of great vessels
1. Allows greater exposure of disc space
277. Ligation of midline tributaries
1. L4-L5 – iliolumbar and segmental vessels
2. L5-S1 – midline sacral vessels
278. Débridement of anterior longitudinal ligament at desired level and exposure of disc space
279. Incision into disc with subsequent discectomy
280. Exposure to ventral dura
281. Interbody cage insertion +/− bone graft
282. Closure in layers
Postoperative care
283. Adequate analgesia
284. Neurological observations
285. Postoperative X-rays
286. No spinal precautions – sit to any angle and mobilise as tolerated
_Viva questions_
1. Describe the relevant surgical landmarks when planning an anterior approach to the T10 vertebral body.
- What are the indications for performing an anterior approach to the spine?
- Describe where the segmental blood supply of the vertebral body lies in relation to the disc.
- At what level of the thoracic spine does the inferior border of the scapula lie when the arms are by the sides? Where, in relation to the spinous process, does the corresponding pedicle of the same vertebra lie?
- Describe what steps you would take to minimise wrong level surgery in the thoracic spine.
6. What role do chest drains have in thoracic spinal surgery?
- What factors are involved in selecting patients for scoliosis surgery?
- Give a brief account of the preoperative management of a patient due to undergo scoliosis surgery.
- Describe the positioning and the peripheral nerves at risk from prone positioning of a patient.
- Which nerve runs in the lateral recess at the L5-S1 level?
- Describe your intraoperative and postoperative management of a dural tear.
- What might be the presentation and management of an acute epidural haematoma?
- Describe the approach for a lumbar discectomy.
4. What nerve root would be compressed by an L4-L5 far lateral disc?
5. An L4-L5 left-sided paracentral disc protrusion will impinge on which nerve root?
- What is the incidence of nerve root injury with a discectomy?
- Describe the orientation of the facet joints at different levels of the spine.
8. Following temporary success of facet blocks, which other radiological procedure can be performed with potential for longer-lasting benefit?
9. Which nerve root leaves the spinal canal via the L4-L5 foramen?
