
Surgery of the Peripheral Nerve
Carpal tunnel decompression
Ulnar nerve decompression at the wrist
Ulnar nerve decompression at the elbow
63
Principles of surgery on peripheral nerves
Principles of brachial plexus surgery
Viva questions
76
68
72
80
84
Carpal tunnel decompression
Preoperative planning
Indications
1. Median nerve compression neuropathy at the wrist
2. As part of a fasciotomy for compartment syndrome/decompression after distal radial fracture
3. Drainage of sepsis
Contraindications
4. Active overlying skin infection
5. Uncertainty over diagnosis – may warrant further investigation before proceeding
Consent and risks
1. Nerve injury : Median nerve injury less than 1%; palmar cutaneous nerve injury less than 1%
2. Radial artery injury : Less than 1%
3. Failure to relieve symptoms : 1%–10%; the incidence is highest in heavy/repetitive manual workers
4. Pillar pain : Quoted at up to 10%; this is tenderness around the site of ligament release
5. Scar tenderness : The incidence is reduced by massage in the postoperative period
6. Complex regional pain syndrome (rare)
7. Infection
Operative planning
History and clinical examination remain the mainstay of diagnosis. It is essential to examine the entire limb as well as the cervical spine to exclude a ‘double-crush’ lesion. Nerve conduction studies are useful and should be available on the day of surgery. They are considered essential in cases of recurrent carpal tunnel syndrome and complex upper limb lesions. Prolonged sensory latency is the earliest and most reliable nerve conduction abnormality. Magnetic resonance imaging (MRI) is rarely indicated, unless there is clinical evidence of a space-occupying lesion causing the symptoms. Conventional radiography is not generally indicated. Consideration should be given to extraneous causes such as diabetes mellitus, rheumatoid and other arthritides, amyloidosis and thyroid dysfunction; where appropriate these may also require investigation prior to operation.
Anaesthesia and positioning
Theproceduremaybecarriedout under local, regionalor generalanaesthesia. Most primary decompressions are performed under local anaesthesia. A local anaesthetic consisting of 1% lidocaine and 0.5% bupivacaine in a 1:1 mixture is infiltrated into the wound prior to surgical draping. General anaesthesia is usually reserved for revision procedures.
The patient is positioned supine on an operating table and the arm is positioned on an arm table in supination, with a padded lead hand used to maintain finger extension. A tourniquet is inflated to 250 mm Hg. In obese patients, a forearm tourniquet is recommended.
Surgical technique
Landmarks
The tendon of palmaris longus (absent in about 10%) is easily seen and palpated by opposing the thumb and little finger and then flexing the wrist to around 30°. The distal end of the tendon bisects the anterior surface of the carpal tunnel. Other useful landmarks include the thenar skin crease (running at the base of the thenar eminence) and the transverse skin crease of the wrist joint (running parallel to the joint line). The transverse wrist crease marks the proximal border of the flexor retinaculum. If the thumb is outstretched to 90°, a parallel line drawn across the palm in line with its distal border represents the surface marking of the superficial palmar arch: this is known as Kaplan’s cardinal line (Figure 5.1). Incision The incision runs a few millimetres to the ulnar side of the thenar skin crease, in the line of the long axis of the ring finger. This ensures that any scarring is well away from the median nerve and ensures that proximal extension avoids the palmar cutaneous branch of the median nerve. The extent is from the distal volar wrist up to a few millimetres proximal to the superficial palmar arch. In revision surgery, the proximal extent is increased: this is curved to run along the ulnar side of the palmaris longus tendon (Figure 5.2). This avoids crossing the wrist joint crease at a right angle and, once again, minimises any damage to the palmar cutaneous branch of the median nerve. PCN
R
FRC
M
PL
U
K
H





Figure 5.1 Surface anatomy of the wrist and hand. (FCR, flexor carpi radialis tendon; H, hook of hamate; K, Kaplan’s cardinal line; M, median nerve; PCN, palmar cutaneous nerve; PL, palmaris longus tendon; R, recurrent motor branch; U, ulnar nerve.)
Motor branch of medial nerve
Palmar cutaneous branch of median nerve
Palmaris longus
Median nerve










Figure 5.2 Extended incision for revision/complex carpal tunnel decompression.
Dissection
Structures at risk
1. Palmar cutaneous branch of the median nerve is at risk if the skin incision is angled to the radial side of the forearm
2. Deep motor branch of the median nerve (due to variation in its course) – staying on the
ulnar side of the median nerve minimises the risk of damaging the structure
3. Superficial palmar arch
4. Median nerve
The exposure continues in line with the skin incision until the superficial palmar fascia is exposed deep to subcutaneous fat. Occasionally, the belly of flexor pollicis brevis (FPB) is superficial to the fascia and is divided. The fibres of the superficial palmar fascia are incised in the same line. Retraction of the skin flaps will reveal the insertion of palmaris longus into the flexor retinaculum. If it is in the way, it can be retracted to the radial side: this exposes the median nerve. Careful dissection through the flexor retinaculum is recommended until the nerve is visualised. A McDonald tissue dissector is passed between the plane of the flexor retinaculum and the median nerve. The dissector must be used with caution and should elevate the retinaculum and not press down on the nerve. The flexor retinaculum is incised with a scalpel, cutting down onto the McDonald tissue dissector, which lies over the nerve and protects it (Figure 5.3). Transverse carpal ligament
Median nerve






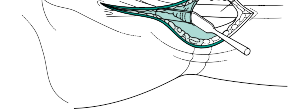
Figure 5.3 Release of the flexor retinaculum.
The nerve is released from proximal to distal. In revision surgery, the nerve should be dissected out proximal to the wrist crease. The perivascular fat pad is the distal border of
the flexor retinaculum. This must be retracted to visualise the distal end of the ligament to ensure complete decompression. The proximal end of the wound should also be retracted to ensure complete release under direct vision with either tenotomy scissors or a blade.
The deep motor branch of the median nerve can have a variable course. Usually, it arises on the radial side of the median nerve as the nerve exits the carpal tunnel. The nerve continues radially, entering the thenar muscles between abductor pollicis brevis and FPB. However, variations may include a motor branch arising from the median nerve within the carpal tunnel, running distally to pierce the retinaculum supplying the thenar muscles. Bearing this in mind during the dissection, it is prudent to stay on the ulnar side of the median nerve to prevent damage to the motor branch.
External neurolysis need only be performed if the nerve is adherent to adjacent structures. Internal neurolysis is not performed.
The tourniquet should be released prior to wound closure. It is important to check for reperfusion of the nerve and to ensure adequate haemostasis before skin closure.
Extensile measures
These are generally not necessary for standard carpal tunnel surgery and are reserved for specific indications.
Proximal
The approach may be extended proximally to expose the median nerve in the forearm. This may be required in cases of fracture fixation with concomitant carpal tunnel decompression. Extension is gained between the tendons of flexor carpi radialis and palmaris longus. The nerve lies on the deep surface of flexor digitorum superficialis in the forearm. The median nerve is retracted to the ulnar side and pronator quadratus incised to access the distal radius.
Distal
The incision may be extended distally with a zigzag incision (Brunner incision) to access any digit, providing a complete palmar exposure. This is useful in procedures requiring the drainage of sepsis.
Closure
Skin closure is performed with 4-0 interrupted nylon sutures. An occlusive dressing is applied, followed by a compressive hand dressing. The compression dressing should allow immediate mobilisation of the fingers and wrist and should not be excessively bulky.
Endoscopic decompression
Endoscopic decompression may be performed through the Brown two-portal or the Agee single-portal technique. The main proven benefits of the endoscopic procedure are restoration of normal grip and absence of a painful scar in the early postoperative period. The procedure, however, has a steep learning curve with complications ranging from nerve injury and an inability to see anatomical variations to incomplete release.
Postoperative care and instructions
The bandage is removed 3–7 days following surgery. The sutures are removed and advice on scar massage given 10–14 days postoperatively. It is imperative that patients are encouraged to mobilise their fingers from day 3 onwards. They should also be counselled that it takes 6 weeks to regain their pinch grip and 3 months to achieve a power grip.
Recommended
Scientific References
-
Cobb T, Dalley B, Posteraro R et al. Anatomy of the flexor retinaculum. _J Hand Surg Am_. 1993;18:91–99. Graham B. The value added by electrodiagnostic testing in the diagnosis of carpal tunnel syndrome.
_J Bone Joint Surg Am_. 2008;90:2587–2593.
Green DP. _Green’s Operative Hand Surgery_ , 7th ed. Philadelphia, PA: Elsevier, 2017.
Hankins CL, Brown MG, Lopez RA et al. A 12-year experience using the brown two-portal endoscopic procedure of transverse carpal ligament release in 14,722 patients: Defining a new paradigm in the treatment of carpal tunnel syndrome. _Plast Reconstr Surg_. 2007;120:1911–1921.
Mintalucci DJ, Leinberry CF. Open versus endoscopic carpal tunnel release. _Orthop Clin North Am_.
2012;43**(4)** :431–437.
Rotman MB, Donovan JP. Practical anatomy of the carpal tunnel. _Hand Clin_. 2002;18:219–230.
Smit A, Hooper G. Elective hand surgery in patients taking warfarin. _J Hand Surg Br_. 2004;29:206–207. Steinberg DR. Surgical release of the carpal tunnel. _Hand Clin_. 2002;18:291–298.
Upton AR, McComas AJ. The double crush in nerve entrapment syndromes. _Lancet_. 1973;2(**7825**): 359–362.
[Ulnar nerve decompression at the wrist](file:///C:/Users/DELL/Desktop/hip/quick%20fact/5.%20Surgery%20of%20the%20Peripheral%20Nerve_Converted.html#bookmark9)
Preoperative planning
Decompression of the ulnar nerve at the wrist is a relatively uncommon procedure. Nerve compression may be associated with space-occupying lesions, anomalous muscles or trauma. It is imperative that the patient is examined from the cervical spine downwards, and clinical findings should be correlated with neurophysiology.
_Indications_
- 1. Decompression of the canal of Guyon [View Source / PubMed]
- 2. Ulnar nerve repair at the wrist (e.g. laceration) _Contraindication_ Active overlying skin infection. _Consent and risks_ [View Source / PubMed]
- 1. Nerve injury [View Source / PubMed]
- 2. Vascular injury [View Source / PubMed]
- 3. Infection [View Source / PubMed]
- 4. Failure to relieve symptoms [View Source / PubMed]
- 5. Stiffness [View Source / PubMed]
- 6. Scar tenderness and hypersensitivity _Anaesthesia and positioning_ The procedure may be carried out under local, regional or general anaesthesia. A local anaesthetic consisting of 1% lidocaine and 0.5% bupivacaine in a 1:1 mixture is infiltrated into the wound prior to surgical draping. There should be a low threshold for general anaesthesia if more than a simple exploration is being considered. The patient is positioned supine on an operating table and the arm is positioned on an arm table in supination, with a padded lead hand used to maintain finger extension. A tourniquet is inflated to 250 mm Hg. Surgical technique _Landmarks_ [The hypothenar eminence and transverse wrist skin crease are important surface landmarks. The bony landmarks of Guyon’s canal (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/5.%20Surgery%20of%20the%20Peripheral%20Nerve_Converted.html#bookmark18)_[Table _ ](#bookmark18) _5.1_) are palpated and marked; the hook of hamate lies 1 cm radial and distal to the pisiform, which is easily palpated at the base of the hypothenar eminence. _Table 5.1 Boundaries of Guyon’s canal_ Floor | Pisohamate and pisometacarpal ligaments, flexor retinaculum and opponens digiti minimi | ---|---| Roof | Volar carpal ligament and palmaris brevis Medial wall | Pisiform, flexor carpi ulnaris and abductor digiti minimi Lateral wall | Flexor digiti minimi, hook of hamate and flexor retinaculum Proximal extent | Flexor retinaculum Distal extent | Fibrous arch of the hypothenar muscles _Incision_ [The incision lies in between the two landmarks (hook of hamate and pisiform) and runs distally for approximately 4 cm and proximally for 3 cm (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/5.%20Surgery%20of%20the%20Peripheral%20Nerve_Converted.html#bookmark19)[Figure ](#bookmark19)5.5). It is curved to the ulnar side, on crossing the wrist flexor crease, to overlie the tendon of flexor carpi ulnaris (FCU). _Superficial dissection_ _Structure at risk_ A crossing cutaneous nerve between the ulnar nerve and the skin exists in 15% of cases and must be protected. The subcutaneous fat is incised to the deep fascia of the forearm. The tendon of FCU is identified, and the fascia is incised on its radial border. The FCU tendon is retracted to the ulnar side revealing the ulnar nerve and artery (the artery lies radial to the nerve). If necessary, the incision is followed proximally to release the distal aspect of the antebrachial fascia. Ulnar proper digital nerve to the small finger Hypothenar muscle 4th common digital nerve Thenar muscle Deep motor branch of the ulnar nerve Pisohamate ligament Pisiform Ulnar Ulnar nerve artery Palmar carpal ligament              Figure 5.4 The relations of Guyon’s canal. Ulnar nerve Flexor carpi ulnaris Ulnar artery      Figure 5.5 The incision for ulnar nerve decompression at the wrist. _Deep dissection_ [Once the nerve and artery are identified proximally, they are traced distally where they enter Guyon’s canal. The volar carpal ligament is incised taking care not to damage the nerve or artery (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/5.%20Surgery%20of%20the%20Peripheral%20Nerve_Converted.html#bookmark20)[Figure ](#bookmark20)5.6). The hook of hamate is then identified. Incising the edge of the hypothenar muscles reveals the deep motor branch as it continues around the hook of hamate. Flexor carpi ulnaris Volar carpal ligament Ulnar nerve and artery          Figure 5.6 Incision of the volar carpal ligament. Incising the volar carpal ligament, the palmaris brevis muscle and the hypothenar fibrous tissue will decompress the ulnar nerve within Guyon’s canal. The nerve need not be completely circumferentially dissected out as this may devascularize it. Distally, the interval between the pisohamate and pisometacarpal ligaments is explored for any masses, fibrous bands or fracture fragments. The superficial branch passes superficial to the fibrous arch of the hypothenar muscles. The ulnar artery must be examined at this point to ensure that it is free of aneurysm or thrombus – it should be smooth and not tortuous. Despite the ability to accurately diagnose the site of compression, surgical decompression should involve exposure of the nerve from the distal forearm to the hand distal to the bifurcation. The most common causes of compression are ganglia, other space-occupying lesions, fracture fragments and a thrombosed ulnar artery. The tourniquet should be deflated to ensure that there is no iatropathic injury of the ulnar artery and to achieve haemostasis. _Extensile measures_ The incision may be extended proximally to the forearm. The deep fascia is incised on the radial border of FCU. A plane is developed between the FCU and the flexor digitorum superficialis (FDS), retracting the FCU to the ulnar side, revealing the ulnar nerve. _Closure_ Skin closure is performed with 4-0 interrupted nylon sutures and a bulky, compressive hand dressing is applied. Postoperative care and instructions The bandage is removed 3–7 days following surgery, and active finger motion is encouraged at all times. Sutures are removed at 10–14 days postoperatively. Recommended references Chen SH, Tsai TM. Ulnar tunnel syndrome. _J Hand Sur_. 2014;39**(3)** :571–579. Green DP. _Green’s Operative Hand Surgery_ , 7th ed. Philadelphia, PA: Elsevier, 2017. Polatsch DB, Melone CP, Beldner S et al. Ulnar nerve anatomy. _Hand Clin_. 2007;23:283–289. [Ulnar nerve decompression at the elbow](file:///C:/Users/DELL/Desktop/hip/quick%20fact/5.%20Surgery%20of%20the%20Peripheral%20Nerve_Converted.html#bookmark11) Preoperative planning _Indications_ [View Source / PubMed]
- 1. Ulnar nerve compression with or without recurrent subluxation of the nerve [View Source / PubMed]
- 2. Exploration of the ulnar nerve in trauma _Contraindication_ Active overlying skin infection. _Consent and risks_ [View Source / PubMed]
- 1. Nerve injury to the ulna, median or medial antebrachial nerve (the most common at 4%) [View Source / PubMed]
- 2. Medial elbow tenderness: 10% [View Source / PubMed]
- 3. Failure to relieve symptoms and recurrence: 10% [View Source / PubMed]
- 4. Elbow stiffness: 5%–10% [View Source / PubMed]
- 5. Elbow instability associated with medial epicondylectomy: 1%–5% _Operative planning_ A full neurological examination of the upper limb must take place. This should include an examination of the cervical spine as well as eliciting Tinel’s sign at the elbow and wrist. Unlike in carpal tunnel disease, neurophysiological examination should be performed in almost all cases. It istheauthors’ preferredchoicetomanagethemajorityofcaseswithsimpledecompression. Other options include partial medial epicondylectomy or nerve transposition procedures (which can be subcutaneous or submuscular). Partial medial epicondylectomy can be useful where there is significant extrinsic pressure on the nerve (e.g. an osteophyte). Transposition remains controversial because of an increased incidence of haematoma and infection without convincing improvements in results. _Anaesthesia and positioning_ The procedure may be carried out under regional or general anaesthesia. The authors prefer a medial approach as this avoids incision directly over the nerve. It also allows early visualisation of the medial antebrachial cutaneous nerve of the forearm. The patient is positioned supine on an operating table and the arm is positioned on a padded arm table, in supination, with the shoulder externally rotated. If a posterior approach is used, the patient is positioned in the lateral decubitus position with the arm placed in front of the chest, resting on a padded arm gutter. If a tourniquet is used it is inflated to 250 mm Hg. The authors do not routinely use a tourniquet, as pre-infiltration with local anaesthetic mixed with adrenaline provides excellent postoperative analgesia as well as a clear field for surgical dissection. Surgical technique _Landmarks_ [The olecranon can easily be palpated posteriorly as it is a subcutaneous structure. Similarly the medial epicondyle is easily palpated. The nerve runs between these two structures and is at its most superficial at this point.](file:///C:/Users/DELL/Desktop/hip/quick%20fact/5.%20Surgery%20of%20the%20Peripheral%20Nerve_Converted.html#bookmark22)[Figure ](#bookmark22)5.7 shows the relations of the ulnar nerve at the elbow. Biceps muscle Brachial artery Brachial nerve Flexor-pronator mass Triceps muscle Arcade of Struthers Flexor carpi ulnaris muscle Medial intermuscular septum Ulnar nerve Medial epicondyle Osborne’s fascia Articular branch Olecranon Motor branch to FCU Cubital tunnel retinaculum (Osborne’s ligament)          _Medial approach_ Figure 5.7 The relations of the ulnar nerve. The medial incision starts 5 cm proximal to the medial epicondyle and extends distally to lie medial to the ulna distal to the elbow joint. It is advisable to place the skin incision anterior to the medial epicondyle so that the nerve does not lie directly under the skin wound. This prevents scarring directly over the nerve, and the medial cutaneous nerve of the forearm branch can be visualised. It is also less likely that a painful medial pressure area will occur. Subcutaneous tissues are reflected proximally and distally exposing the cubital tunnel retinaculum. _Posterior approach_ This is recommended for the identification of the nerve in complex elbow trauma. A longitudinal incision is made in the midline approximately 5 cm above the olecranon. The incision is curved laterally around the lateral side of the olecranon process and then curved medially so that the incision lies over the middle of the ulna distally. Curving the incision laterally moves the suture line away from the midline and avoids any potential pressure area over the olecranon process. The subcutaneous tissues are then dissected medially to expose the medial epicondyle. The advantage of the posterior approach is that frequently patients may have other elbow disorders requiring surgery (e.g. rheumatoid arthritis) and further incisions may be performed through the same scar. The disadvantage is that considerable dissection is necessary to expose the medial side adequately. _Deep dissection_ The ulnar nerve is identified proximal to the cubital tunnel by blunt dissection. It is first released at the arcade of Struthers (the hiatus in the medial intermuscular septum through which the ulnar nerve enters the posterior compartment). The roof of the cubital tunnel is Osborne’s ligament (the cubital tunnel retinaculum) proximally and Osborne’s fascia (the deep component of the aponeurosis of the two heads of FCU) distally. The nerve is followed distally and Osborne’s ligament is incised from proximal to distal. The veins lying on the dorsal surface of the medial intramuscular septum should be identified and coagulated. The nerve is traced into the two heads of the FCU to ensure release distally. At this stage it is important to identify and protect the motor branch to the FCU. The nerve should not be dissected from its groove as this may lead to subluxation and devascularisation. After release, the elbow is moved through its full range; the nerve should be lax in full extension and should remain in the groove in full flexion. Residual adherent structures should be released and if subluxation is a problem then medial epicondylectomy or subcutaneous transposition should be considered. _Medial epicondylectomy_ This procedure is useful in patients with a medial epicondyle fracture non-union or space-occupying lesions within the cubital tunnel (e.g. medial osteophyte, exostosis or ganglion). Routine decompression is performed, after which the common flexor origin is elevated off the medial epicondyle in a subperiosteal manner. A sleeve is left around the bone to ensure smooth closure and haemostasis. A partial medial epicondylectomy is performed with a narrow osteotome; bone wax can be placed on the exposed cancellous bone. The periosteal sleeve is closed over the epicondyle stump with a heavy Vicryl suture; this should be done in full extension so that an extension lag is avoided. The anteroinferior medial collateral ligaments must be avoided and no more than 20% of the depth of the epicondyle should be excised to prevent elbow instability. _Subcutaneous transposition_ The theory behind transposing the nerve is to reduce tensile stress on the nerve. This occurs during traction on the nerve in flexion and leads to an increased intraneural pressure and flattening of the nerve around the medial epicondyle. This increased pressure may cause temporary ischaemia. The medial intramuscular septum must be divided to ensure tension-free transposition. It is essential that the longitudinal vascular supply of branches are protected and allowed to move with the main body of the nerve. Once the nerve is decompressed and easily transposable anterior to the medial epicondyle, a subcutaneous fascial flap is elevated with a scalpel. The nerve is placed anterior to the deep surface of the flap and the distal flap edges are sutured to deep dermal tissue with an absorbable 3-0 Vicryl suture. The wound is then closed as normal. _Closure_ The wound is closed with interrupted 2-0 Vicryl sutures for the subcutaneous layer and a running subcuticular monofilament suture for skin. If a tourniquet has been used it should be released and followed by meticulous haemostasis. A sterile dressing should be applied and then a compressive dressing over it. Postoperative care and instructions Dressings are removed at 3–4 days. Range-of-motion exercises within the limits of comfort should be started at the same stage. Active hand and wrist motion is encouraged at all times. The wound should be checked at 2 weeks and the patient advised on appropriate care of the scar. Heavy lifting should be avoided for 1 month. It is important to counsel the patient that not all symptoms may be relieved by the surgery and that recovery may take up to 6 months. Recommended references Catalano LW, Barron OA. Anterior subcutaneous transposition of the ulnar nerve. _Hand Clin_. 2007;23:339–344. Macadam SA, Gandhi R, Bezuhly M, Lefaivre KA. Simple decompression versus anterior subcutaneous and submuscular transposition of the ulnar nerve for cubital tunnel syndrome: A meta-analysis. _J Hand Surg Am_. 2008;33**(8)** :1314.e1–1314.e12. Mowlavi A, Andrews K, Lille S et al. The management of cubital tunnel syndrome: A meta-analysis of clinical studies. _Plast Reconstr Surg_. 2000;106:327–334. O’Driscoll SW, Jaloszynski R, Morrey BF et al. Origin of the medial ulnar collateral ligament. _J Hand Surg Am_. 1992;17:164–168. Osterman AL, Spiess AM. Medial epicondylectomy. _Hand Clin_. 2007;23:329–337. Staples JR, Calfee R. Cubital tunnel syndrome. _J Am Acad Orthop Surg_. 2017;25**(10)** :e215–e224. Waugh RP, Zlotolow DA. _In situ_ decompression of the ulnar nerve at the cubital tunnel. _Hand Clin_. 2007;23:319–327. [Principles of surgery on peripheral nerves](file:///C:/Users/DELL/Desktop/hip/quick%20fact/5.%20Surgery%20of%20the%20Peripheral%20Nerve_Converted.html#bookmark8) Preoperative planning The aims of surgery are [View Source / PubMed]
- 1. To confirm a diagnosis and establish prognosis [View Source / PubMed]
- 2. To restore function [View Source / PubMed]
- 3. To relieve pain _Indications_ [View Source / PubMed]
- 4. Closed traction injury of the brachial plexus leading to severe paralysis [View Source / PubMed]
- 5. Associated nerve and vascular injury [View Source / PubMed]
- 6. Nerve injury with an associated fracture requiring early internal fixation [View Source / PubMed]
- 7. Increasing progression of a neurological injury or an entrapment neuropathy [View Source / PubMed]
- 8. Failure of recovery of a lesion within an expected time frame [View Source / PubMed]
- 9. Failure of recovery in conduction block within 6 weeks of injury [View Source / PubMed]
- 10. Persistent pain following injury [View Source / PubMed]
- 11. Severe paralysis of a nerve following blunt trauma _Contraindications_ [View Source / PubMed]
- 12. Active infection [View Source / PubMed]
- 13. Function unaffected by nerve injury _Consent and risks_ [View Source / PubMed]
- 1. Infection [View Source / PubMed]
- 2. Nerve damage/failure of repair [View Source / PubMed]
- 3. Vascular injury [View Source / PubMed]
- 4. Specific to the site of operation, e.g. local structures at risk _Operative planning_ Earlier surgery following nerve injury permits easier identification of tissues (due to less scar tissue) and therefore any repair is easier as it is possible to visualise and match the arrangement of the cut ends of the nerve fascicles. The results of prompt repair are also markedly better due to the favourable biological environment for nerve healing. A nerve stimulator should be available. Magnification of at least three times with loupes is helpful. If nerve grafting is likely to be performed, a suitable donor graft should be identified preoperatively and the patient made aware of the need. _Anaesthesia and positioning_ Surgical procedures involving the exploration or repair of peripheral nerves should be performed under general anaesthesia, with antibiotic cover to minimise the chance of any postoperative infection. Where possible, a tourniquet is used to achieve a completely bloodless field, facilitating ease of identification of structures. Remember that after approximately 15 minutes of ischaemia, nerve conduction becomes abnormal so any tourniquet should be released when stimulating a nerve. Surgical technique _Incision_ The course of cutaneous nerves should always be remembered when planning a skin incision. A painful neuroma may result from a transected cutaneous nerve and lead to considerable morbidity to the patient. _Nerve assessment_ When nerves have been damaged and surgery has been delayed, a neuroma will have formed. The consistency of a neuroma is important when assessing nerve injury, as a hard neuroma may represent an abundance of connective tissue and little in the way of nerve tissue. Making an incision through the damaged epineurium permits visualisation of any nerve bundles present, and stimulation of the nerve proximally. This may give some indication as to likely recovery. Stimulating the nerve proximally and recording from the nerve distally give the best guide for recovery. An absence of recording distally is a relative indication to resect and repair the nerve, depending on the macroscopic fascicular structure seen. Care should be taken not to undertake excessive mobilisation, as this may lead to devascularisation of a nerve. Bipolar diathermy should be used at all times when coagulating blood vessels around nerves. Methods of repair _Primary repair_ The ends of an injured nerve are cut back progressively until the cut surfaces show bulging healthy nerve bundles. An end-to-end anastomosis is performed, which is possible if the resection gap has been small, little mobilisation of the nerve has been necessary, and the nerve is not under tension. Flexing a nearby joint reduces tension on a nerve, and extra length can be gained by transposition (e.g. anterior transposition of the ulnar nerve) of a nerve. The two principal types of primary repair are _epineural_ repair and _fascicular_[repair. Epineural repair is technically less demanding and faster to complete. Fascicular repair (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/5.%20Surgery%20of%20the%20Peripheral%20Nerve_Converted.html#bookmark24)**[Figure** ](#bookmark24)**5.8**[) is performed if there has been a clean transection of a nerve trunk (e.g. in the brachial plexus). In each method of repair, the true epineurium is exposed. In a fascicular repair, the matched bundles are opposed and sutured with perineurial 11-0 nylon sutures, and then 10-0 nylon sutures are passed through the perineurium and epineurium. This is done circumferentially to complete the repair. In an epineurial repair (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/5.%20Surgery%20of%20the%20Peripheral%20Nerve_Converted.html#bookmark25)**[Figure** ](#bookmark25)**5.9**), the fascicular groups in the nerve ends are matched as closely as possible and the ends are then sutured with 10-0 nylon sutures through the epineurium. An initial suture is placed at each of the lateral ends of the nerve, with interrupted sutures subsequently placed on the anterior and posterior aspect of the nerve to complete the repair.       Figure 5.8 Fascicular nerve repair.                            Figure 5.9 Epineural repair. _Nerve grafiing_ [Cable grafts (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/5.%20Surgery%20of%20the%20Peripheral%20Nerve_Converted.html#bookmark26)[Figure ](#bookmark26)5.10) are the gold standard for bridging gaps between two cut ends of a nerve where primary repair is not possible. Nerve bundles are matched to bundles; this is achieved by viewing and matching the nerve ends either using loupes or a microscope, using magnification to get the best possible match. Cable grafts consist of multiple cutaneous nerve strands from a donor nerve. The most common donor nerves used are the medial cutaneous nerve of the forearm and the sural nerve in the lower limb. As many grafts as required are used to give good coverage of the cut face of the nerve. The length of the graft should be approximately 15% longer than the gap to be bridged. The grafts can either be fixed with a tissue glue or sutured in place. If a gap to be bridged is greater than 10 cm, grafting is unlikely to be of great benefit.                       Figure 5.10 Cable nerve grafting. If a nerve has been severely damaged to the extent that repair and grafting are not possible, nerve transfer (neurotisation) is performed: a distal nerve is reinnervated using an intact donor proximal nerve. _Nerve transfer_ Nerve transfers where a nerve, serving a less important function or where the structure innervated by a nerve is damaged beyond repair, is used as a donor to restore a more useful function are an alternative to nerve repair and grafting. These are particularly useful where nerves are injured proximally and need a lengthy period of regeneration following proximal repair or where proximal repair is not possible in cases of brachial plexus avulsions. By anastomosing the donor to the recipient stump closer to the innervation point, the time to regeneration is shortened and also need for a graft is avoided. The technique of anastomosis is similar to that of primary repair. Surgical loupes, meticulous dissection, knowledge of fascicular anatomy of the nerve, and the use of intraoperative nerve stimulators are essential to isolate motor nerve fascicles from the main nerve. Unlike tendon transfers, motor nerve transfers, when successful, restore a more natural function, but they need to be performed before degeneration of the end target taking into account the time taken for the nerve to regrow across the anastomosis to the end target. Common nerve transfers include spinal accessory nerve transfer to the suprascapular nerve in cases of C5 avulsion/injury to restore posterosuperior shoulder cuff function, Somsak procedure where a branch of the radial to one of the heads of triceps is anastomosed to the anterior motor branch of the axillary nerve to restore deltoid function, and modified Oberlin procedure where the ulnar nerve and/or the median nerve fascicle innervating a wrist flexor is divided at the level of mid arm and anastomosed to the motor fascicle of the musculocutaneous nerve innervating biceps and/or brachialis. Anterior interosseous nerve transfer to the ulnar nerve motor fascicle at the wrist helps restore function of hand intrinsics in cases of high ulnar nerve lesions or injury to the lower trunk of the brachial plexus. Nerve transfers have also been shown to improve function in spinal cord injury and by targeted muscle innervation increase the range of movements in amputation prosthesis. Postoperative care and instructions After nerve decompression, patients are told to leave their bulky dressings in place until they have a wound inspection 2 weeks postoperatively. Instruction to begin early hand and finger mobilisation is encouraged in upper limb surgery. After nerve repair and grafting, the limb is generally protected in a plaster with a sling (or crutches in the lower limb) for a period of between 3 and 6 weeks. Either outpatient or inpatient therapy (as in the case of a brachial plexus repair) is required to overcome any residual stiffness and deformity. This may include appropriate splintage and is often multidisciplinary, with occupational therapy, physiotherapy and pain team input. [Principles of brachial plexus surgery](file:///C:/Users/DELL/Desktop/hip/quick%20fact/5.%20Surgery%20of%20the%20Peripheral%20Nerve_Converted.html#bookmark10) Preoperative planning The principles of brachial plexus surgery are similar to those of other peripheral nerve operations (see previous section). The five roots of the brachial plexus lie in the posterior triangle of the neck between scalenus anterior and scalenus medius muscles. Injuries between the posterior root ganglion and the spinal cord are termed _preganglionic_. The three trunks of the brachial plexus lie in front of one another and in the posterior triangle of the neck. The divisions of the plexus lie posterior to the clavicle. The medial, lateral and posterior cords of the plexus are related to the second part of the axillary artery deep to pectoralis minor. _Indications_ [View Source / PubMed]
- 1. Section/rupture/avulsion of the plexus [View Source / PubMed]
- 2. Associated vascular and nerve injuries [View Source / PubMed]
- 3. Open wounds [View Source / PubMed]
- 4. Compressive neuropathy _Anaesthesia and positioning_ The procedure is performed under general anaesthesia, with the patient supine and the head elevated to approximately 30°. Supraclavicular approach to the brachial plexus [View Source / PubMed]
- 5. Cervical and brachial plexus (root/trunk) surgery [View Source / PubMed]
- 6. Spinal accessory nerve surgery [View Source / PubMed]
- 7. Suprascapular nerve surgery [View Source / PubMed]
- 8. Sympathetic chain surgery _Landmarks_ The landmarks for the supraclavicular approach are those of the posterior triangle of the neck. The base is formed by the clavicle, the medial border is formed by the medial border of the sternocleidomastoid muscle and the lateral border is formed by the edge of the trapezius muscle. _Incision_ _Structure at risk_ [View Source / PubMed]
- 1. Supraclavicular nerves The skin incision is made approximately one finger’s breadth above the clavicle in line with the bone. Care must be taken not to damage the supraclavicular nerves, as a painful neuroma may develop. _Dissection_ Skin flaps are raised exposing the apex of the posterior triangle superiorly and the clavicle inferiorly. Next the plane between the external jugular vein and the sternocleidomastoid is developed, with the omohyoid muscle displayed inferiorly in the wound. The muscle is divided and reflected. Deep to the fat pad, the transverse cervical artery is present and is at risk; it is ligated. The phrenic nerve is visualised running across the scalenus anterior. The nerve is followed proximally, revealing C5. The deep cervical fascia is incised, and C5 and C6 are seen emerging from the lateral aspect of scalenus anterior; C7 is visualised between the scalenus anterior and the upper trunk. The lower trunk is seen following division of the scalenus anterior. By following the plane between the subclavian artery and the lower trunk, C8 and T1 are visualised. Infraclavicular approach to the brachial plexus _Indications_ [View Source / PubMed]
- 9. Complete exposure of brachial plexus (when combined with supraclavicular approach) [View Source / PubMed]
- 10. Infraclavicular brachial plexus repair _Dissection_ Essentially this is analogous to the deltopectoral approach to the upper humerus. The difference lies in mobilising the cephalic vein medially and detaching and reflecting the pectoralis minor muscle from the coracoid process. In a full exposure, the pectoralis major insertion on the humerus may also be detached. Fiolle Delmas approach _Indications_ The Fiolle Delmas approach combines the supraclavicular and infraclavicular approaches and is useful in an extensive injury to the plexus. _Incision_ [The platysma, with skin flaps, is elevated and the mid-portion of the clavicle is exposed superiorly and inferiorly. An extension is made of the collar incision to expose the supraclavicular portion (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/5.%20Surgery%20of%20the%20Peripheral%20Nerve_Converted.html#bookmark28)[Figure ](#bookmark28)5.11). This extension starts at around the mid-portion of the supraclavicular incision and extends distally over the mid-portion of the clavicle running over the delto-pectoral groove to the axilla. It is a true extensile approach and can be continued distally, if necessary, as the anterior approach to the humerus. When the infraclavicular is combined with the supraclavicular approach, full exposure is given from the second part of the subclavian artery to the terminal portion of the axillary artery, with exposure of the brachial plexus from the spinal nerves to the terminal branches of the plexus. _Dissection_ [A clavicular osteotomy may be required to facilitate access, especially if there is a vascular injury. In this case a plate should be precontoured and holes predrilled for easy fixation at the end of the procedure, remembering that the bone will be shortened by the thickness of the saw blade. Distally the pectoralis major muscle is detached from the humerus in its upper portion or, if required, its entirety. The muscle is then reflected medially exposing the clavicle, pectoralis minor muscle and clavipectoral fascia (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/5.%20Surgery%20of%20the%20Peripheral%20Nerve_Converted.html#bookmark29)[Figure ](#bookmark29)5.12). The pectoralis minor muscle is divided at its tendon taking care not to damage the musculocutaneous nerve. The subclavius muscle is divided with the suprascapular vessels (once ligated). This exposes the entire plexus and vasculature from the first rib to the axilla.  Figure 5.11 Incision for the Fiolle Delmas approach to the brachial plexus. Subclavian vein Deltoid Subclavius divided Pectoralis major divided Pectoralis minor                             Figure 5.12 Dissection in the Fiolle Delmas approach to the brachial plexus. Postoperative care and instructions Following nerve repair/transfer, the limb may require immobilisation in a cast for 3 weeks after which the patient can start motion progressively. In the case of brachial plexus surgery, a sling is applied with a body strapping for 3 weeks, followed by readmission for a week at 6 weeks after index operation to start the rehabilitation process. Recommended references Birch R. _Surgical Disorders of the Peripheral Nerves_. London, UK: Springer London, 2011. Henry HK. _Extensile Exposure_ , 2nd ed. Edinburgh, Scotland: Churchill Livingstone, 1957. Isaacs J, Cochran AR. Nerve transfers for peripheral nerve injury in the upper limb. _Bone Joint J_. 2019;101–B(**2**):124–131. Ray WZ, Chang J, Hawasli A, Wilson TJ, Yang L. Motor nerve transfers: A comprehensive review. _Neurosurgery_. 2016;78(**1**):1–26. Tupper JW, Crick JC, Mattich LR. Fascicular nerve repairs. _Orthop Clin North Am_. 1988;19:57–69. [_Viva questions_](file:///C:/Users/DELL/Desktop/hip/quick%20fact/5.%20Surgery%20of%20the%20Peripheral%20Nerve_Converted.html#bookmark12) [View Source / PubMed]
- 1. Describe the landmarks and incision for a carpal tunnel decompression. [View Source / PubMed]
- 2. Describe the main structures at risk in a carpal tunnel decompression. [View Source / PubMed]
- 3. What are the sites of compression of the ulnar nerve at the elbow? [View Source / PubMed]
- 4. What are the surface landmarks for Guyon’s canal? [View Source / PubMed]
- 5. Which structures commonly cause ulnar tunnel compression neuropathy at the elbow? [View Source / PubMed]
- 6. Describe the techniques used in primary nerve repair. [View Source / PubMed]
- 7. What options are available if primary repair is not possible? [View Source / PubMed]
- 8. What are the principal considerations for successful nerve transfer surgery? [View Source / PubMed]
- 9. What are the priorities in gaining function after brachial plexus injury? [View Source / PubMed]
