Comprehensive Introduction and Patho-Epidemiology
The evolution of hip surgery, particularly primary total hip arthroplasty (THA), represents one of the most profoundly successful interventions in the history of modern orthopedic surgery. Often dubbed "the operation of the century," THA provides unparalleled pain relief and functional restoration for patients suffering from end-stage hip pathology. However, the contemporary standard of care demands more than mere pain relief; it requires the restoration of native biomechanics, meticulous soft tissue preservation, and the minimization of postoperative complications. Central to achieving these optimal outcomes is a profound understanding and mastery of the short external rotators (SERs) of the hip. These structures are not merely anatomical landmarks to be divided and discarded; they are critical dynamic stabilizers that dictate the success of the posterior approach, influence postoperative kinematics, and serve as the primary defense against prosthetic instability.


To appreciate the role of the short external rotators, one must first understand the baseline kinematics and range of motion (ROM) profiles of the native hip joint. The normal hip exhibits a complex, multi-planar arc of motion governed by osseous morphology and the surrounding capsuloligamentous and musculotendinous envelopes. Physiologic range of motion typically encompasses 125° of flexion, 0° of extension (with further apparent extension occurring via lumbar lordosis), 45° of abduction, 25° of adduction, 60° of external rotation, and 40° of internal rotation. The short external rotators are intimately involved in modulating this motion, particularly in controlling internal rotation during the stance phase of gait and preventing anterior subluxation of the femoral head. When these normal kinematics are disrupted by end-stage arthropathy, the surgical intervention must aim to restore this baseline without compromising the dynamic restraints.


Historically, in scenarios where arthroplasty was contraindicated or failed catastrophically, hip arthrodesis was employed. The optimum position for hip arthrodesis underscores the biomechanical resting state of the joint: 20°–25° of flexion, 0°–5° of adduction, and 0°–10° of external rotation. This position allows for optimal ambulation with compensatory pelvic and spinal motion. While arthrodesis is now a rare primary procedure, understanding this optimal spatial orientation is crucial for the arthroplasty surgeon. It highlights the functional imperative of slight external rotation for normal gait mechanics—a vector directly controlled by the SER complex. Mastery of these structures ensures that when a THA is performed, the dynamic tensioning required to maintain this functional resting state is preserved, thereby optimizing the patient's postoperative gait efficiency and reducing edge-loading on the prosthetic components.
The Evolution of Hip Arthroplasty
The trajectory of total hip arthroplasty has shifted from a focus purely on implant survivorship to a dual focus encompassing both tribological longevity and soft-tissue optimization. Early iterations of the posterior approach involved aggressive, non-repaired tenotomies of the short external rotators, leading to unacceptably high rates of posterior dislocation. The realization that the piriformis, the gemelli, the obturator internus, and the obturator externus are not expendable structures catalyzed a paradigm shift in surgical technique. Today, the academic consensus mandates an enhanced posterior soft tissue repair (EPSTR). This evolution reflects a deeper epidemiological understanding of dislocation mechanisms, revealing that the vast majority of early postoperative instability events are directly attributable to soft tissue insufficiency rather than component malposition.


Kinematics and Range of Motion Profiles
The kinematics of the reconstructed hip are heavily reliant on the integrity of the posterior envelope. While the bony architecture (acetabular version and femoral anteversion) provides static stability, the short external rotators provide the essential dynamic stability. During activities of daily living, such as rising from a low chair or pivoting, the hip is subjected to high degrees of flexion, adduction, and internal rotation—the classic position of posterior dislocation. In a native hip, the SER complex eccentrically contracts to decelerate internal rotation and compress the femoral head into the acetabulum. In the arthroplasty setting, a meticulously repaired SER complex acts as a physical tether and a proprioceptive trigger, safeguarding the 125° of flexion and 40° of internal rotation expected in a normal joint without allowing the prosthetic head to escape the confines of the acetabular liner.


Detailed Surgical Anatomy and Biomechanics
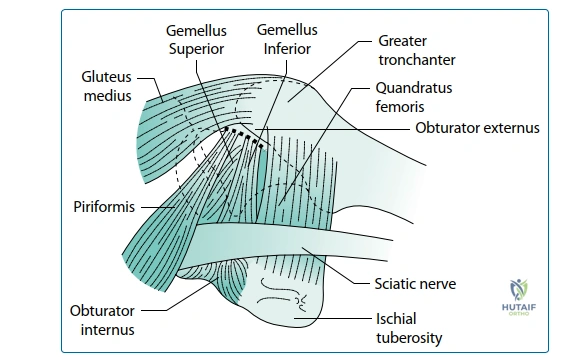
A rigorous, three-dimensional spatial awareness of the short external rotator complex is the hallmark of a master hip surgeon. This complex comprises six distinct muscles: the piriformis, superior gemellus, obturator internus, inferior gemellus, obturator externus, and quadratus femoris. The piriformis originates from the anterior sacrum and inserts into the superior aspect of the greater trochanter, serving as a primary landmark for identifying the anatomic femoral axis. Immediately inferior lies the triceps coxae—the superior gemellus, obturator internus, and inferior gemellus—which share a common tendinous insertion into the medial surface of the greater trochanter, deep to the piriformis fossa. The obturator externus courses inferior to the acetabulum to insert into the trochanteric fossa, while the broad quadratus femoris spans from the ischial tuberosity to the intertrochanteric crest.


Biomechanically, these muscles function synergistically as the "rotator cuff of the hip." While their primary concentric action is external rotation of the extended thigh, their more critical biomechanical role is as dynamic stabilizers. During the gait cycle, particularly at heel strike and early stance, these muscles fire to fine-tune the position of the femoral head within the acetabulum, resisting anterior translation vectors generated by the powerful hip extensors and abductors. Furthermore, the obturator externus has been identified as a critical inferior hammock, preventing inferior translation and providing a crucial barrier against prosthetic impingement during extreme flexion. The meticulous preservation or anatomic repair of these structures is paramount to restoring this dynamic stabilization, thereby preventing micro-separation and subsequent edge-loading of the bearing surfaces.


The vascular and neurological proximity of the short external rotators adds a layer of complexity to their surgical management. The medial circumflex femoral artery (MCFA), the primary blood supply to the native femoral head, courses superior to the upper border of the quadratus femoris and deep to the obturator externus. While the femoral head is resected in THA, preservation of the MCFA is critical in hip preservation surgeries and remains relevant in arthroplasty to minimize profound bleeding and hematoma formation. More critically, the sciatic nerve descends intimately posterior to the SER complex. It typically emerges from the greater sciatic foramen inferior to the piriformis (though anatomical variants exist) and rests directly upon the triceps coxae and quadratus femoris. The SERs thus act as a vital protective cushion for the sciatic nerve. Overzealous retraction or careless division of these muscles can lead to direct compressive or traction neurapraxia of the sciatic nerve, a devastating complication.


The Short External Rotator Complex
Surgical dissection of the SER complex requires a nuanced approach. The traditional method of en bloc tenotomy near the trochanteric insertion compromises the tendinous footprint, making robust repair challenging. Advanced techniques advocate for a "peel" or osteotomy of the tendinous insertions, taking a small fleck of bone or a thick sleeve of periosteum from the greater trochanter. This ensures that when the complex is repaired, the healing occurs via a bone-to-tendon or bone-to-bone interface, which is biomechanically superior to tendon-to-tendon healing. Furthermore, the obturator externus should be carefully identified and preserved whenever possible, as its division significantly increases the risk of inferior instability. If division is necessary for adequate exposure, it must be meticulously tagged alongside the piriformis and obturator internus for subsequent transosseous repair.


Vascular and Neurological Proximity
The anatomical relationship between the SERs and the sciatic nerve dictates the placement of retractors during the posterior approach. The classic Charnley retractor or blunt Hohmann retractors must be placed carefully superior to the piriformis and inferior to the quadratus femoris to avoid direct nerve compression. The divided ends of the SERs are often reflected posteriorly and held with a stay suture; this maneuver not only clears the surgical field but also interposes the muscle bellies between the retractors and the sciatic nerve, providing a protective buffer. Meticulous hemostasis of the ascending branch of the MCFA, located within the substance of the quadratus femoris, is mandatory. Failure to recognize and coagulate this vessel during the inferior release can result in a massive postoperative hematoma, which increases the risk of deep infection, sciatic nerve compression, and delayed wound healing.

Exhaustive Indications and Contraindications
Patient selection is the cornerstone of successful total hip arthroplasty. The primary indication for THA is a painful, debilitating condition of the hip joint that has proven refractory to comprehensive conservative management (including weight loss, physical therapy, activity modification, NSAIDs, and intra-articular injections). The most frequent underlying pathology is primary osteoarthritis, characterized by progressive loss of articular cartilage, subchondral sclerosis, and osteophyte formation. Inflammatory arthropathies, such as rheumatoid arthritis and ankylosing spondylitis, represent another major cohort, often presenting with bilateral, symmetric joint destruction and requiring careful preoperative systemic optimization. Avascular necrosis (osteonecrosis) of the femoral head, driven by trauma, corticosteroid use, or idiopathic causes, frequently necessitates arthroplasty in younger demographics. Additionally, post-traumatic arthritis secondary to acetabular fractures or femoral neck non-unions serves as a robust indication for intervention.


Conversely, strict adherence to contraindications is vital to prevent catastrophic failures. Absolute contraindications include active local or systemic infection. Performing a THA in the presence of bacteremia or an infected joint space guarantees prosthetic joint infection (PJI), a devastating complication requiring multiple revision surgeries. Another absolute contraindication is profound dysfunction of the abductor complex (gluteus medius and minimus) or severe, unrecoverable neurological disease (e.g., advanced Parkinson's disease, severe hemiplegia) that prevents ambulation or renders the hip inherently unstable. In these scenarios, the absence of dynamic stabilization will inevitably lead to recurrent dislocation, regardless of how meticulously the short external rotators are repaired.


Young age (<50 years) is traditionally viewed as a relative contraindication due to the finite lifespan of prosthetic bearing surfaces and the cumulative risk of multiple future revisions. However, advancements in highly cross-linked polyethylene and ceramic-on-ceramic tribology have significantly mitigated wear rates. Therefore, in the highly symptomatic young patient with profound functional limitation, THA is increasingly justified. Such cases must be discussed extensively with the patient, emphasizing the likelihood of future revision, and should be performed by an appropriately experienced surgeon capable of executing precise component positioning and meticulous soft tissue preservation to maximize implant longevity. Other relative contraindications include severe medical comorbidities (e.g., recent myocardial infarction, uncontrolled diabetes), morbid obesity (BMI > 40), and active intravenous drug abuse.
| Category | Specific Condition | Rationale / Surgical Consideration |
|---|---|---|
| Primary Indications | Primary Osteoarthritis | Refractory pain, loss of joint space, functional decline. |
| Inflammatory Arthropathy | Rheumatoid/Ankylosing Spondylitis; requires disease-modifying drug management pre-op. | |
| Avascular Necrosis (AVN) | Collapse of the femoral head; often affects younger patients requiring durable bearings. | |
| Post-Traumatic Arthritis | Secondary to acetabular/femoral neck fractures; often involves distorted anatomy. | |
| Absolute Contraindications | Active Infection | Local or systemic bacteremia guarantees PJI; requires eradication prior to surgery. |
| Abductor Dysfunction | Paralysis or massive tearing of gluteus medius/minimus leads to intractable instability. | |
| Non-ambulatory Status | Bedbound patients derive no functional benefit and face high surgical risks. | |
| Relative Contraindications | Young Age (< 50 years) | High risk of outliving the implant; requires advanced tribology and meticulous technique. |
| Morbid Obesity (BMI > 40) | Exponentially higher risk of infection, dislocation, and component failure. | |
| Severe Medical Comorbidities | Uncontrolled cardiopulmonary disease increases the 0.3% baseline mortality risk. |
Patient Selection Criteria
The decision-making process for THA must be highly individualized. The surgeon must correlate the patient's subjective complaints with objective radiographic findings. A patient with severe radiographic osteoarthritis but minimal pain should be managed expectantly, whereas a patient with moderate radiographic changes but profound functional limitation may be an excellent surgical candidate. The status of the short external rotators and the abductor mechanism should be assessed clinically preoperatively. A positive Trendelenburg sign or profound weakness in external rotation may alter the surgical approach or necessitate specific reconstructive techniques (e.g., the use of constrained liners or dual mobility constructs) to prevent postoperative instability.


Absolute and Relative Contraindications
Navigating contraindications requires a multidisciplinary approach. For patients with absolute contraindications like active infection, coordination with infectious disease specialists is mandatory for targeted antibiotic therapy and potential staged interventions. In cases of relative contraindications, such as morbid obesity, preoperative optimization programs focusing on weight loss and diabetic control (aiming for an HbA1c < 7.0) are critical to mitigating the elevated risks of infection (baseline 1-2%, but significantly higher in obese/diabetic cohorts) and thromboembolism (DVT 2%, PE 1%). The ethical imperative of the orthopedic surgeon is to optimize the host before introducing a massive foreign body, ensuring that the risk-to-benefit ratio remains overwhelmingly in the patient's favor.
Pre-Operative Planning, Templating, and Patient Positioning
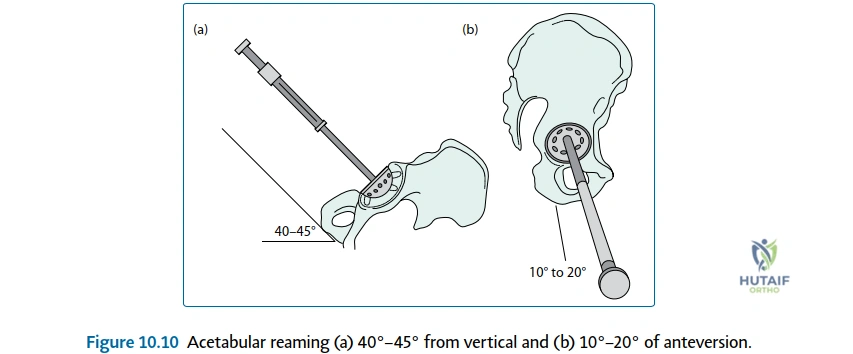
Meticulous preoperative planning is the foundation of a flawless execution in the operating theater. The goal of templating is not merely to select implant sizes but to comprehensively reconstruct the biomechanical parameters of the hip: the center of rotation, femoral offset, and leg length. Recent, high-quality, properly scaled radiographs are mandatory. An anteroposterior (AP) view of the pelvis with the hips internally rotated 15° (to profile the femoral neck) and a true lateral view of the affected hip are the standard requirements. Digital templating software allows the surgeon to accurately size the acetabular component, ensuring adequate coverage and restoration of the anatomic center of rotation, which is critical for optimizing the lever arm of the abductor musculature and the short external rotators.


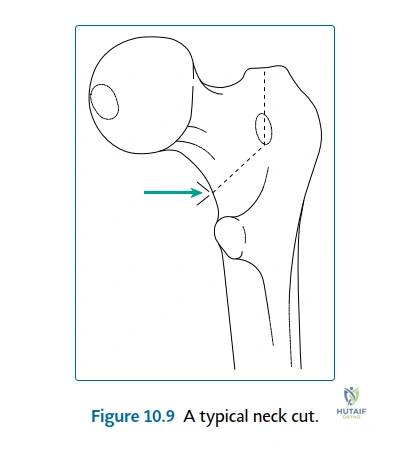
Femoral templating focuses on selecting a stem that provides rigid initial fixation (whether cemented or uncemented) while restoring the native femoral offset and leg length. Failure to restore offset leads to laxity in the abductor and SER complexes, significantly increasing the risk of dislocation and resulting in a biomechanically inefficient gait (Trendelenburg lurch). Conversely, excessive offset can cause trochanteric bursitis and localized pain. The surgeon must also template the level of the femoral neck cut, referencing the distance from the lesser trochanter, to ensure accurate reproduction of leg length. Anticipating limb length discrepancy (a complication occurring in up to 15% of cases) during the templating phase allows the surgeon to make intraoperative adjustments to achieve equality, which is paramount for patient satisfaction and spinal mechanics.


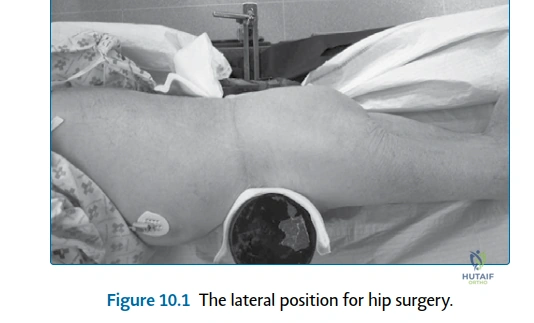
Patient positioning is equally critical, particularly when utilizing the posterior approach where the short external rotators will be directly manipulated. The patient is placed in the lateral decubitus position. Rigid pelvic fixation using specialized positioners (e.g., peg boards or specialized clamps) is mandatory to prevent pelvic roll during the procedure. Unrecognized pelvic tilt or rotation intraoperatively will lead to inaccurate assessment of acetabular version and inclination, predisposing the patient to impingement and dislocation. The anterior superior iliac spines (ASIS) must be perfectly vertical to the floor. Proper positioning ensures that the surgeon's spatial orientation remains true to the preoperative template, allowing for precise component implantation and optimal tensioning of the soft tissue envelope.
Radiographic Assessment and Digital Templating
Digital templating begins with scaling the radiograph using a known calibration marker (typically a 25mm or 30mm sphere placed between the patient's legs). The acetabular component is templated first, aiming for 40°-45° of inclination and 15°-20° of anteversion, touching the radiographic teardrop medially without violating the Kohler line. The femoral stem is then templated to establish the neck resection level and restore the center of rotation. The relationship between the center of the prosthetic head and the tip of the greater trochanter is evaluated; this distance dictates the resting tension of the short external rotators. If the center of rotation is medialized or the offset is decreased, the SERs will be pathologically lax, necessitating a more aggressive soft tissue repair or a change in component selection to prevent posterior instability.


Operating Room Setup and Positioning
The operating room setup must facilitate seamless workflow and strict asepsis. Following induction of anesthesia, the patient is rolled into the lateral decubitus position. The dependent leg is padded to prevent peroneal nerve palsy, and an axillary roll is placed to protect the brachial plexus. The pelvic positioners are applied firmly against the ASIS and the sacrum. The surgeon must physically palpate the pelvis to confirm absolute stability before draping. The surgical field is prepared with an alcohol-based chlorhexidine solution, and wide draping is employed to allow full mobility of the operative leg. This mobility is essential for the extreme positions required during the posterior approach (flexion, adduction, internal rotation) to adequately expose and safely detach the short external rotators without placing undue tension on the sciatic nerve.


Step-by-Step Surgical Approach and Fixation Technique
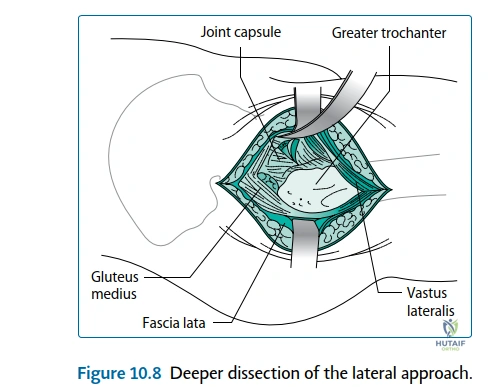
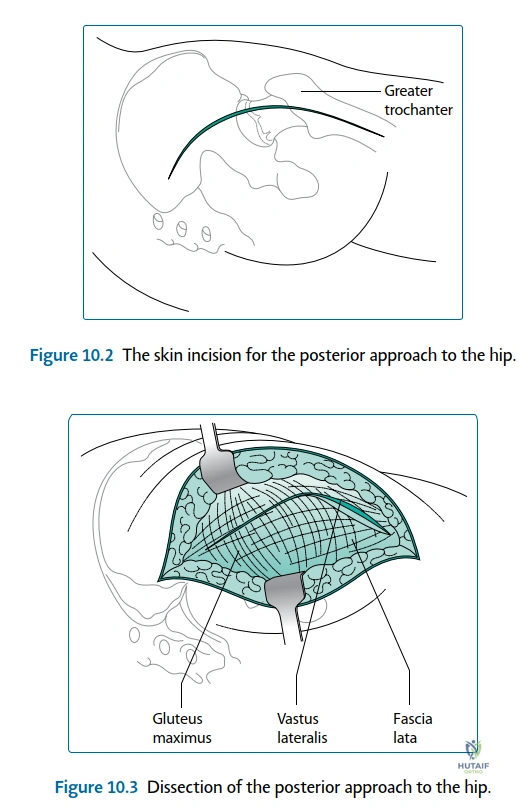
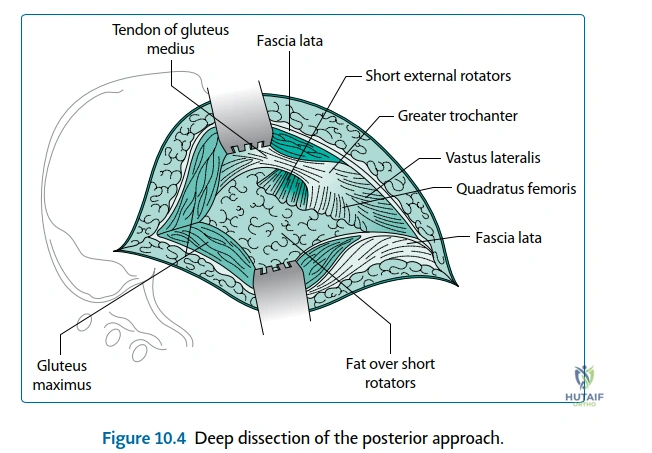
The posterior (Moore or Southern) approach remains the workhorse for total hip arthroplasty globally, offering unparalleled exposure of the proximal femur and acetabulum. The skin incision is centered over the posterior third of the greater trochanter, extending proximally toward the posterior superior iliac spine and distally along the femoral shaft. The subcutaneous tissues are divided, exposing the fascia lata and the gluteus maximus. The gluteus maximus is split bluntly in line with its fibers, avoiding the inferior gluteal nerve and vessels. A Charnley retractor is deployed to maintain this window. Deep to the maximus, the bursa overlying the greater trochanter is excised, revealing the critical anatomy: the posterior border of the gluteus medius proximally, the vastus lateralis distally, and the short external rotators in the center of the field.


The mastery of the procedure lies in the handling of the short external rotators. The hip is gently internally rotated to place the SER complex on stretch. The piriformis tendon is identified at its insertion into the superior aspect of the greater trochanter. Proceeding inferiorly, the conjoined tendon of the obturator internus and the gemelli is identified. A heavy, non-absorbable stay suture (e.g., #2 or #5 Ethibond) is passed through these tendons close to their insertion. The tendons are then sharply detached from the bone, ideally taking a small cortical flake to facilitate later bone-to-tendon healing. The obturator externus and the superior half of the quadratus femoris are similarly tagged and detached. These tagged muscles are reflected posteriorly, acting as a protective soft-tissue sling over the sciatic nerve. A complete capsulectomy or a robust capsulotomy (preserving the capsule for later repair) is then performed to expose the femoral head for dislocation and neck resection.


Following acetabular reaming, cup impaction, and femoral preparation, the components are implanted. The final, and arguably most crucial step for preventing dislocation, is the Enhanced Posterior Soft Tissue Repair (EPSTR). The hip is reduced, and the components are tested for stability through a full range of motion. The tagged short external rotators and the posterior capsule are then advanced back to their anatomic footprint on the greater trochanter. This is typically achieved by drilling two or three transosseous tunnels through the posterior aspect of the greater trochanter. The heavy sutures attached to the SERs are passed through these tunnels and tied tightly over the lateral cortex with the hip in slight external rotation and abduction. This robust repair restores the dynamic posterior tension band, significantly reducing the dead space for hematoma formation and providing an immediate mechanical barrier against posterior dislocation.
The Posterior Approach and Soft Tissue Handling
The meticulous handling of the soft tissue envelope dictates the speed and quality of postoperative recovery. When dividing the quadratus femoris, the surgeon must be vigilant for the ascending branch of the medial circumflex femoral artery. This vessel must be isolated and electrocoagulated or ligated; failure to do so results in a persistent postoperative hematoma that can compromise the SER repair and increase the risk of deep infection. The reflection of the SERs must be gentle to avoid traction injury to the underlying sciatic nerve. Throughout the procedure, retractors must be placed precisely—avoiding placement deep to the transverse acetabular ligament or hooking excessively over the anterior column, which can endanger the obturator or femoral nerves, respectively.


Component Implantation and Enhanced Repair
The biomechanical success of the EPSTR relies on the rigid fixation of the components. If the femoral stem is placed in excessive retroversion, the SERs will be under pathological tension and may avulse from their repaired footprint. Conversely, excessive anteversion leaves the repair lax and ineffective. The transosseous repair of the SERs must be robust enough to withstand the early forces of rehabilitation. Studies have shown that a meticulous EPSTR reduces the dislocation rate from a historical >3% down to less than 1%, comparable to the rates seen with the direct anterior approach. The repair is tested intraoperatively by internally rotating the hip to 45° in extension; the repaired tendons should remain firmly approximated to the trochanteric bone without gapping or suture pull-out.

Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, total hip arthroplasty carries a defined risk profile. The overarching mortality rate is approximately 0.3%, primarily related to cardiopulmonary events in the immediate perioperative period. Nerve injury, most commonly involving the sciatic or peroneal nerves, occurs in roughly 1% of cases. This is often due to excessive lengthening of the limb, direct retractor compression, or postoperative hematoma formation deep to the repaired short external rotators. Infection remains one of the most dreaded complications, occurring in 1%–2% of patients with primary osteoarthritis, but escalating to 5% in immunocompromised cohorts, such as those with rheumatoid arthritis. Thromboembolic events are a persistent threat, with deep vein thrombosis (DVT) occurring in 2% of cases and pulmonary embolism (PE) in 1%, necessitating rigorous pharmacological and mechanical prophylaxis protocols.


Dislocation occurs in approximately 3% of all primary THAs, though this rate is highly dependent on surgical approach, component positioning, and the integrity of the soft tissue repair. A failed or omitted repair of the short external rotators is a primary driver of early posterior dislocation. Heterotopic ossification (HO) develops in up to 10% of patients, though the vast majority of these cases are radiographically apparent but clinically asymptomatic; severe Brooker Class III or IV HO requiring excision is rare. Limb length discrepancy is a frequent source of patient dissatisfaction, noted in up to 15% of cases. While mild discrepancies (<1 cm) are well-tolerated, larger discrepancies can lead to pelvic obliquity, secondary spinal pain, and sciatic nerve stretch. Long-term, aseptic loosening remains the primary mode of failure, with revision surgery required in up to 10%
Clinical & Radiographic Imaging Archive