
🎓
Viva Exam
| Radial head replacement | 113 | Elbow aspiration/injection | 152 |
|---|---|---|---|
| Total elbow arthroplasty | 123 | Elbow arthroscopy | 154 |
| Open elbow arthrolysis | 137 | Viva question | 158 |
| Tennis/golfer’s elbow release | 142 | ||
| Lateral collateral ligament reconstruction | 148 | ||
| --- | --- | --- | |
| Flexion | 150° | 130° | |
| Extension | 0° | 30° | |
| Pronation | 80° | 50° | |
| Supination | 80° | 50° | |
| Position of arthrodesis | |||
| 1. There is no fixed position of arthrodesis. | |||
| 2. Many authors recommend 90°. | |||
| 3. 110° may be best for activities of daily living, but 60° may suit work activities. | |||
| The deep surgical approaches to the elbow may be achieved through a single ‘utility’ posterior incision or through separate incisions. The approaches described here may be used in their entirety or in part, depending on the anatomy required to be exposed for each procedure. We focus on the approaches that will prove useful for common elbow operations, but this is not an exhaustive collection of all approaches described. | |||
| Radial head replacement | |||
| Preoperative planning | |||
| Indications | |||
| 1. Fractures not amenable to fixation (e.g. >3 fragments) with valgus instability due to medial collateral ligament insufficiency | |||
| 2. Radial head fracture with concurrent distal radioulnar joint injury (Essex-Lopresti injury) | |||
| 3. Instability following radial head resection | |||
| Contraindications | |||
| 4. Radial head/neck fractures with no associated injuries can be treated with excision of the radial head. | |||
| 5. Wear or extensive injury to the capitellum chondral surface. | |||
| 6. Inadequate bone and soft tissues around the implant. | |||
| Consent and risks | |||
| 1. Nerve injury | |||
| 2. Infection | |||
| 3. Aseptic loosening | |||
| 4. ‘Understuffing’ radiocapitellar joint: Recurrent or ongoing instability | |||
| 5. ‘Overstuffing’ radiocapitellar joint with increased joint pressure: Pain and stiffness | |||
| 6. Osteoarthritis | |||
| Operative planning | |||
| Anteroposterior and lateral radiographs less than 6 months old should be available. Silicone implants are no longer recommended due to high rates of osteolysis and implant fracture. | |||
| Other procedures can be utilised for lateral compartment arthrosis or conditions wherein both the capitellum and radial head require addressing, including radiocapitellar replacement, though their indications are distinct from those for radial head replacement. | |||
| Types of replacement | |||
| The following are implant design characteristics, though there is currently no evidence to suggest that any prosthesis is significantly superior to the others: | |||
| Type | Articulation | Stem | Fixation |
| --- | --- | --- | --- |
| Monoblock | Fixed bearing | Straight | Cemented |
| Modular | Mobile bearing (bipolar) | Curved | Press-fit |
| Pyrocarbon | |||
| Bipolar implants provide less stability than fixed-bearing prostheses in vitro , but a clinical difference has not been demonstrated. Modular implants allow for easy adjustment of the height of the head and neck, as well as the head size. | |||
| Anaesthesia and positioning | |||
| Anaesthesia is usually general, augmented by infraclavicular regional nerve blockade if not contraindicated (previous nerve trauma or palsy at the elbow or more proximally). An | |||
| initial dose of antibiotic is given intravenously. The antibiotic of choice depends on local policy; we use teicoplanin and gentamicin in our practice. Note: If intraoperative biopsies are required to diagnose sepsis, then antibiotics can be withheld until intraoperative samples have been obtained. | |||
| The patient is placed in the lateral decubitus position with the operated arm uppermost. Padded lumbar and pelvic supports are used. | |||
| A Carter Braine arm support or well-padded drape support is used to cradle the arm, allowing the forearm to move freely in the vertical position, permitting access to the dorsal aspect and both sides of the elbow and to the anterior compartment by external rotation of the shoulder, if required (Figure** 7.1**). Of note in this position: The ulnar nerve and medial aspect of the elbow are on the side of the elbow facing the feet of the patient. | |||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
| Figure 7.1 Patient position. | |||
| A padded narrow tourniquet (inflation to 200 mm Hg is usually sufficient) or an S-MART bandage/tourniquet is used. At least 15 cm of the dorsal aspect of the arm is required for ease of access. The elbow should be sufficiently mobile for appropriate movement intraoperatively. The hand, forearm and arm to the axilla are prepared with a germicidal solution. Waterproof drapes are used with adhesive edges to provide a seal to the skin. An antibacterial adhesive skin drape is applied. | |||
| Surgical technique | |||
| Any associated injuries will dictate the type of incision required. Posterior, medial and lateral structures can be exposed with the same single posterior incision; if only lateral access is required, a lateral incision can be performed. We delineate the more commonly used Kocher interval, as well as the Kaplan interval. | |||
| Posterolateral approach (Kocher) | |||
| This is an extensile intermuscular approach to the lateral elbow, between anconeus (supplied by the radial nerve) and extensor carpi ulnaris (supplied by the posterior interosseous nerve, PIN). | |||
| Landmarks | |||
| Landmarks include the lateral supracondylar ridge, lateral epicondyle, radial head and tip of the olecranon. Palpate the lateral epicondyle and move the fingers distally until a | |||
| depression is felt. The radial head lies within a palpable depression distal to the lateral epicondyle. It can be felt to move on pronation and supination of the forearm. | |||
| Incision | |||
| ## The skin incision extends approximately 5 cm proximal to the lateral epicondyle and continues distally over the epicondyle, along the anterolateral surface of the forearm for approximately 5 cm (Figure 7.2). | |||
| Lateral column | |||
| Extensor carpi ulnaris | |||
| Anconeus | |||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
| Figure 7.2 The incision for Kocher’s approach. | |||
| Dissection | |||
| Structures at risk | |||
| 1. Radial nerve | |||
| 2. Lateral antebrachial cutaneous nerve | |||
| 3. Posterior interosseous nerve | |||
 🔍 Click to enlarge |
|||
| The incision is continued through subcutaneous fat, protecting the lateral antebrachial cutaneous nerve typically lying on the deep fascia, and through the fascia between triceps and origins of the extensor carpi radialis longus (ECRL) and brachioradialis. An interval is developed between the triceps posteriorly and the origins of ECRL and brachioradialis anteriorly (Figure** 7.3**). In the proximal end of the wound, the radial nerve must be avoided in the interval between the brachialis and brachioradialis muscles. The common origin of the extensor muscles is elevated from the lateral epicondyle while preserving the origin of the lateral collateral ligament. Campbell’s modification of this approach describes taking | |||
| (b) | |||
| ECRB | |||
| Brachioradialis | |||
| ECRL | |||
| EDC | |||
| ECU | |||
| Triceps | |||
| Anconeus | |||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
| (a) | |||
| Radial nerve | |||
| ECRB | |||
| Brachioradialis | |||
| ECRL | |||
| EDC | |||
| ECU | |||
| Triceps | |||
| Anconeus | |||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
| C | |||
| A | |||
| B | |||
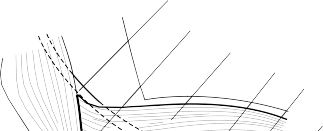
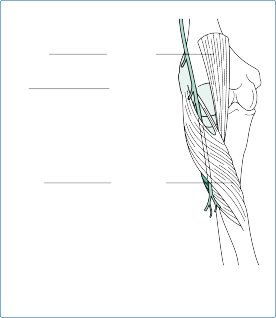
| Figure 7.3 (a) Normal lateral anatomy of the elbow, with the Kocher interval highlighted and path of the radial nerve shown. (A) Limited Kocher approach. (B) Extended Kocher approach. | |||
| (C) Column approach. (b) The limited Kocher approach, between anconeus | |||
| and extensor carpi ulnaris (ECU). (Continued) | |||
| (c) | |||
| Brachioradialis | |||
| ECRB | |||
| ECRL | |||
| EDC | |||
| ECU | |||
| Triceps | |||
| Anconeus | |||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
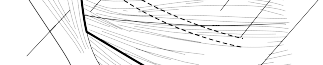
| Figure 7.3 (Continued) (c) The extended Kocher approach. The common extensor origin is reflected from the lateral epicondyle. | |||
| ## the common extensor origin together with a thin flake of bone, using a small osteotome. Reflecting the common origin distally exposes the radiocapitellar joint. The PIN is vulnerable as it enters the supinator and must be protected by pronation of the forearm during dissection, careful retractor placement and avoiding dissection into the supinator muscle (Figure 7.4). | |||
| Lateral approach (Kaplan) | |||
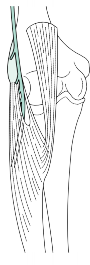
| ## The Kaplan intermuscular approach to the elbow between extensor digitorum communis (EDC, supplied by the PIN) and extensor carpi radialis brevis (ECRB, variable innervation supplied by the PIN, superficial branch of the radial nerve or the undivided radial nerve), which provides excellent radiocapitellar joint visualisation. The radial nerve can translate mediolaterally 1 cm with forearm pronation (Figure 7.4), but even so remains in close proximity to the surgical field; therefore, this approach is less commonly undertaken than the Kocher approach for radial head replacement. | |||
| Landmarks | |||
| Landmarks are the same as those mentioned for the Kocher approach. | |||
| Incision | |||
| The skin incision extends from the lateral epicondyle approximately 5 cm distally, towards the dorsal radial tubercle. Proximal extension is as described for the Kocher approach. | |||
| ECRB | |||
| Brachioradialis | |||
| ECRL | |||
| EDC | |||
| ECU | |||
| Triceps | |||
| Anconeus | |||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
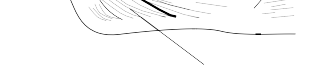
| Figure 7.4 The Kaplan approach, between extensor carpi radialis brevis and extensor digitorum communis. | |||
| Superficial dissection | |||
| Superficial dissection for the Kaplan approach is the same as for the Kocher approach. | |||
| Deep dissection | |||
| Kaplan’s interval lies between EDC posteriorly and ECRL and ECRB anteriorly. The interval can be developed distally to the level of the PIN, until it pierces the supinator at the Arcade of Frohse (Figure 7.5). As with the Kocher approach, the common extensor origin can now be elevated from the lateral epicondyle to grant access to the capsule deep to it. | |||
| Procedure | |||
| ## The origins of the brachioradialis and ECRL muscles are elevated subperiosteally and the capsule incised to expose the lateral aspect of the elbow joint. By incising the capsule anterior to the lateral ligamentous complex, (overlying the radial head) in line with the radius, the lateral collateral ligament can be avoided. The incision must not stray too far anteriorly as the radial nerve runs over the anterolateral portion of the elbow capsule (Figure 7.6). | |||
| ## The annular ligament is incised longitudinally before transecting the radial neck with an oscillating saw using a radial cutting jig (Figure 7.7). Exposure distal to the annular ligament risks damaging the PIN and is avoided. The cut surface of the proximal radius should be smooth and even, so that contact between it and the collar of the prosthesis is complete. | |||
| The proximal radial medullary canal is prepared with burs or rasps to accept the implant stem. A Hohmann retractor behind the posterior aspect of the radial neck can help to | |||
| Biceps tendon | |||
| Posterior interosseous nerve | |||
| Supinator | |||
| Forearm supinated | |||
| Forearm pronated | |||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
| Figure 7.5 The dynamic position of the posterior interosseous nerve. | |||
| Capsular incision | |||
| Radial collateral ligament | |||
| Lateral ulnar collateral ligament | |||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
| Figure 7.6 Lateral capsule incision, anterior to the lateral ligament complex. | |||
| deliver the neck, to facilitate access to the canal. For press-fit stems, the preparation must be tight and accurate; this is less critical for cemented stems. The diameter of the articulating surface of the radial head trial prosthesis should be chosen to match the diameter of the articulating surfaceof the native radial head (Figure** 7.8**). If the radial head diameter is between two available sizes, the smaller of the two should be used. A trial is inserted to | |||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
| Overestimated diameter | |||
| Radial head | |||
| Correct diameter of radial | |||
| head prosthesis | |||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
| Figure 7.8 Using the diameter of the radial head (left) may overestimate the size of the prosthesis. The diameter of the articulating surface (right) should be used instead. | |||
| Figure 7.7 The radial neck cut. | |||
| ## ensure that contact with the capitellum is satisfactory. To prevent excessive wear of the capitellum from ‘overstuffing’, the proximal edge of the prosthesis should be level with the lateral edge of the coronoid (Figure 7.9). The elbow is taken through a range of flexion and extension in both supination and pronation (Figure 7.10). If the elbow tracking is satisfactory in flexion and extension, the final prosthesis is inserted. | |||
| Closure of lateral approach | |||
| The annular ligament is repaired with an absorbable suture. The common extensor origin is reattached to the lateral epicondyle with transosseous sutures. A suction drain is inserted. The deep dermal layer is approximated with absorbable sutures, then a continuous | |||
| Gapping of the lateral ulnohumeral facet suggestive of overstuffing | |||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
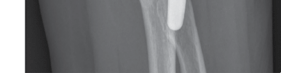
| Figure 7.9 Anteroposterior left elbow radiograph demonstrating a radial head replacement with an overstuffed radiocapitellar joint – identified by the separation of the ulnohumeral articulation. | |||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
 🔍 Click to enlarge |
|||
| Figure 7.10 Trial reduction to test range of motion. | |||
| absorbable subcuticular suture with Steri-Strips to the skin. An occlusive dressing is applied, and the elbow is wrapped with wool and a crepe bandage in extension. | |||
| Postoperative care and instructions | |||
| The drain, wool and bandage are removed after 24 hours. Gentle active mobilisation of the elbow can begin at this time under supervision. Return to work is allowed after | |||
| approximately 6 weeks for sedentary jobs, but may be delayed to 3 months or more in active work. The wound should be checked for any signs of abnormal healing or infection at 2 weeks, after which surgical follow-up is recommended at 6 weeks, 6 months and 1 year after surgery. Continuation of follow-up is typically at yearly intervals thereafter. The patient should be advised to return to clinic if there is pain or functional deterioration. | |||
| Recommended |
Scientific References
-
Heijink A, Kodde I, Mulder P et al. Radial head arthroplasty: A systematic review. _JBJS Rev_. 2016;**4(10)**. Marinelli A, Guerra E, Ritali A et al. Radial head prosthesis: Surgical tips and tricks. _Musculoskelet Surg_.
2017;101(Suppl 2):187–196.
Watkins CEL, Elson DW, Harrison JWK, Pooley J. Long-term results of the lateral resurfacing elbow arthroplasty. _Bone Joint J_. 2018;100-B(3):338–345.
[Total elbow arthroplasty](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark11)
Preoperative planning
With the significant advancements in the medical management of rheumatoid arthritis, the number of patients requiring primary elective total elbow arthroplasty (TEA) is decreasing. Nonetheless, the valuable role of TEA in improving pain and function in the appropriate patient cannot be underestimated. It remains a low-volume procedure, with just over 400 TEAs performed per year in the United Kingdom, compared with over 100,000 hip replacements. Recent guidelines advocate complex primary and revision TEAs being managed in specialist centres, with operations jointly performed by two senior surgeons.
_Indications_
Indications include painful elbow conditions that have failed non-operative management, including
- 1. Rheumatoid and other inflammatory arthropathies [View Source / PubMed]
- 2. Primary and post-traumatic osteoarthritis [View Source / PubMed]
- 3. Comminuted distal humeral fractures not amenable to fixation [View Source / PubMed]
- 4. Avascular necrosis _Contraindications_ [View Source / PubMed]
- 5. Infection (generalised or of the limb) [View Source / PubMed]
- 6. Paralysis or dysfunctional neuropathy of the elbow [View Source / PubMed]
- 7. Significant hand dysfunction [View Source / PubMed]
- 8. Relative contraindication – patients who will not be able to comply with postoperative restrictions on function _Consent and risks_ [View Source / PubMed]
- 1. Ulnar nerve injury: 3% [View Source / PubMed]
- 2. Deep infection: 3% [View Source / PubMed]
- 3. Intraoperative fracture: 5% [View Source / PubMed]
- 1. Triceps dehiscence or significant weakness: 1% [View Source / PubMed]
- 2. Dislocation/symptomatic subluxation: Unlinked, 5%; linked, 1% [View Source / PubMed]
- 3. Symptomatic aseptic loosening: Unlinked, 5%; linked, 5% [View Source / PubMed]
- 4. Need for revision surgery: 10%–15% Operative planning ## [Recent radiographs must be available. The lateral and medial distal humeral columns must be present to provide rotatory stability. In cases with significant bone loss, the surgeon should consider use of a custom implant, modular endoprosthesis (](#bookmark28)Figure 7.11) or structural allograft. Availability of the implants must be checked by the surgeon. Biologic agents for rheumatoid arthritis should be discussed with a specialist to create a perioperative plan for stopping and restarting medication.     Figure 7.11 Lateral right humeral radiograph of modular distal humeral replacement, used in tumour surgery and revision surgery for humeral loosening and osteolysis. _Types of replacement_ There are three types of TEA – linked, unlinked and convertible (which may function as an unlinked or linked arthroplasty and can be converted from one to the other intraoperatively). Fully constrained hinged prostheses are no longer used and instead semi-constrained linked prostheses use varying shapes of polyethylene articulating surface to permit some varus-valgus angulation throughout the arc of motion. Note: Though often used interchangeably in error, constraint is distinct from linkage. Some unlinked prostheses are more constrained than linked prostheses. | Linked | Unlinked | Convertible | | --- | --- | --- | | Coonrad-Morrey | Capitellocondylar | Acclaim | | Discovery | Kudo | Latitude | | GSB-III | Sorbie | Nexel | Souter-Strathclyde | | | Linked | Unlinked | | --- | --- | --- | | Advantages | 1. Can be used in cases of ligamentous insufficiency | [View Source / PubMed]
- 2. Allows for more aggressive soft tissue and contracture release [View Source / PubMed]
- 3. Better postoperative range of motion (further extension) | 1. Less bony resection required [View Source / PubMed]
- 2. Lower constraint, possibly lower wear and osteolysis [View Source / PubMed]
- 3. Can be used as distal humeral hemiarthroplasty (e.g. in trauma) Disadvantages | 1. Small risk of linkage dissociation [View Source / PubMed]
- 2. Increased constraint predisposes to increased bushing wear and osteolysis | 1. Risk of dislocation [View Source / PubMed]
- 2. Dependent on soft tissue integrity [View Source / PubMed]
- 3. Requires accurate component positioning Issues regarding the radiocapitellar joint and handling the ulnar nerve in a TEA remain contentious. The radial head may be preserved or excised during a TEA. Radial head impingement may occur if preserved, necessitating a secondary procedure to excise the head. The Latitude prosthesis is modular and allows the surgeon to replace the radiocapitellar articulating surface concurrently. The capitellar surface of the humeral component in this design is anatomic so can articulate with a native or replaced radial head, to allow lateral column load sharing, though any benefit has yet to be borne out in clinical studies. The ulnar nerve may be decompressed or anteriorly transposed during the operation. The approach used in the operation may dictate the handling of the ulnar nerve. Indications for transposing the ulnar nerve in a primary replacement include significant stiffness, preoperative neuropathy or when using a triceps-on approach (see later). It is the authors’ preference to excise the radial head and not to transpose the ulnar nerve routinely. _Anaesthesia and positioning_ Anaesthesia and positioning are the same as for radial head replacement. Surgical technique For primary total elbow arthroplasty the approach employed is largely at the discretion of the operating surgeon. Each approach offers different degrees of exposure to the bony anatomy and varies with their handling of the extensor mechanism. _Triceps splitting_ Many such approaches involve a midline split along the triceps tendon and elevation of each half from the posterior humerus and ulna, as described by Campbell. The Shahane-Stanley modification of this approach splits the triceps towards the medial aspect, with 75% of the muscle bulk laterally and 25% medially in order to avoid the triceps from ‘buttonholing’, while also providing protection for the ulnar nerve. The triceps is repaired with side-to-side sutures or transosseous sutures through the olecranon. _Triceps reflecting_ The Bryan-Morrey approach describes reflection of the triceps from medial to lateral. This provides excellent exposure, but risks postoperative triceps failure if the tendon repair fails. The triceps is reattached to the olecranon with sutures placed through transosseous drill holes. Wolfe and Ranawat described a modification involving osteotomising the triceps attachment on the olecranon with a thin wafer of bone, to aid healing. A lateral to medial reflecting approach can also be used for cases in which lateral-sided pathology requires addressing. _Triceps-on or triceps-preserving approach_ The triceps-on approach maintains the triceps in continuity with the olecranon, either with a single incision or more commonly, a dual para-tricipital incision. The Alonso-Llames approach uses medial and lateral incisions either side of the triceps and elevates the muscle from the posterior aspect of the humerus. The distal humerus can then be displaced medially or laterally to expose the proximal forearm. The approach is limited in its exposure by mobility of the bones and is therefore suited to trauma, when the distal humerus is fractured and more readily mobile. _Triceps-turndown approach_ Campbell’s original description of this approach utilises a V-Y advancement flap in the triceps tendon. This may be required in cases of chronic dislocation or other causes of triceps shortening. This approach has a high rate of triceps disruption and is therefore not commonly used in primary TEA. Instead, it is the authors’ preference when performing a turndown to use an approach based on the blood supply to the triceps, as described by Rajeev and Pooley. _Posterior approach to the elbow_ _Landmarks_ [View Source / PubMed]
- 1. Midline of the humerus [View Source / PubMed]
- 2. Lateral epicondyle [View Source / PubMed]
- 3. Radial head [View Source / PubMed]
- 4. Tip of the olecranon [View Source / PubMed]
- 5. Crest of the proximal ulna _Incision_ The incision is made in a curvilinear fashion towards the tip of the olecranon starting about 7.5 cm proximal to the olecranon, skirting on its lateral side, leaving between 0.5 and 1 cm between the incision and the lateral border of the olecranon (to avoid placing the incision on the weightbearing skin of the elbow). The incision is continued distally parallel to the crest of the ulna (_not_[crossing it or on it) for approximately 6 cm (](#bookmark29)**Figure 7.12**). Radial nerve Incision 7.5 cm Ulnar nerve 6 cm          Figure 7.12 Posterior approach to the elbow. _Superficial dissection_ _Structure at risk_ [View Source / PubMed]
- 1. Ulnar nerve The triceps tendon is more correctly an aponeurosis. There is a superficial sheet having a median vertical aponeurotic extension, between the lateral and long heads of the triceps, which leads to the deep head. This sheet is the guide to the dissection of the triceps. The lateral and medial musculotendinous boundaries of the triceps are revealed by epifascial dissection in the proximal part of the wound. Minimal epifascial dissection is used distal to the olecranon over the subcutaneous border of the ulna, sufficient only to see the deep antebrachial fascia over anconeus. Medial dissection is continued, sufficient to reveal the ulnar nerve immediately subjacent to the medial border of the triceps about 6–7 cm proximal to the medial epicondyle. The ulnar nerve is identified throughout its course, behind the medial condyle, noting the axial vessel and the vena comitans on the deep (articular) surface of the nerve in the cubital sulcus. The fibrous arch between the two bony origins of flexor carpi ulnaris (FCU) is incised, the incision being carried into the muscle for about 2 cm, marking and protecting the nerve branch to FCU, which typically arises proximal to the elbow, and allowing ready displacement of the nerve from the cubital sulcus without tension. A vessel loop can be placed around the nerve to protect and identify it for the remainder of the procedure. _Deep dissection_ _Triceps-splitting approach_ ## [This approach respects the nerve supply to anconeus (an important contributor to elbow stability): this is a distal branch of the radial nerve which crosses the interval between the distal border of the lateral head of triceps and the proximal border of anconeus. Dissection within the lateral head of triceps is to be avoided. The triceps is split between the nerve and blood supply to the long head (a segmental branch can occur very distally) and the nerve to the lateral head, both derived from the radial nerve. The deep head nerve supply is more proximal and is out of the surgical field. The ulnar nerve is protected by keeping dissection lateral and then deep to the long head of the triceps, using the muscular bulk as a protection for the nerve (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark30)[Figure ](#bookmark30)7.13). The triceps aponeurosis is incised in the midline and undermined to define the vertical sheet between the two superficial heads of the triceps. The dissection is then taken down the lateral side of this sheet, i.e. in the intervascular/ interneural plane, to the deep head of the triceps. The superficial heads are parted for about 6 cm, uncovering the filmy layer between them and the deep head. The deep head is then incised (the only muscular incision required in this technique) noting the deep transverse epicondylar vessels under the muscle at the proximal margin of the fat pad in the olecranon fossa. The vessels are cauterised. The fat pad is excised and the olecranon fossa exposed. A posterior capsulectomy is performed and any olecranon osteophytes removed. The antebrachial fascia is incised parallel to and about 1 cm lateral to the crest of the ulna over anconeus. The dissection is taken under the fascia but outside anconeus to the crest and then, on bone, down to the supinator crest, the annular ligament and capsule of the proximal radioulnar joint, lifting anconeus away from the capsule and radial head, but preserving the posterior band of the lateral collateral ligament (to maintain stability in varus strain). _Triceps-reflecting approach_ The medial head of the triceps muscle is separated from the medial intermuscular septum and dissected down to the humerus. Note: At this point, the triceps is still ‘on’ (attached Medial head Lateral head Ulnar nerve Brachioradialis Incision Anconeus Extensor carpi ulnaris Flexor carpi ulnaris Ulna         Figure 7.13 Triceps-splitting approach, deep dissection. to the olecranon) and this is where a triceps-on approach would free the medial border of the triceps from the intermuscular septum. With the triceps-reflecting approach, the medial incision is extended approximately 6 cm distally with subperiosteal dissection of the medial antebrachial fascia to expose the posterior capsule. This fascia is thin over the posterior ulna; therefore, a narrow osteotome can be used to create a series of osteo-periosteo-fascial shingles (small, superficial shards of bone). The periosteo-antebrachial fascia is then sharply dissected from the crest in continuity with the olecranon shingles. ## [The triceps, fascia and periosteum can then be elevated from the olecranon from medial to lateral as a single flap. This is done at 30° flexion to relieve tension on the flap. The flap is mobilised laterally, elevating the anconeus origin from the distal humerus until it can be reflected over the capitellum (](#bookmark31)Figure 7.14). Remnants of the triceps and posterior capsule can then be elevated from the posterior humerus. _Triceps-turndown approach_ A transverse incision is made through the triceps aponeurosis approximately 4 cm proximal to the triceps insertion on the olecranon. The incision is then extended distally Ulnar nerve Triceps muscle Sliver of bone Olecranon                 Figure 7.14 Triceps-reflecting approach, maintaining the triceps in continuity while reflecting from medial to lateral. ## [from its lateral aspect along the deep fascia of the lateral head of triceps and then the deep fascia overlying anconeus midway between the lateral epicondyle and olecranon, until the incision reaches the lateral subcutaneous border of the ulna. The triceps aponeurosis and deep fascia overlying anconeus is then stripped from the muscle bellies, usually requiring sharp dissection proximally and medially. The first transverse incision is extended distally from its medial aspect, to create a fascial flap (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark32)[Figure ](#bookmark32)7.15). ## [Anconeus is then elevated subperiosteally from the ulna. The lateral head of triceps is separated from the intramuscular aponeurosis between the lateral and medial heads with sharp dissection. The muscle fibres run parallel to this incision; therefore, the muscle fibres are not transected. The lateral head and anconeus can now be reflected laterally as a single unit (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark33)[Figure ](#bookmark33)7.16). ## [Repeat the process of separating the muscle from the intramuscular aponeurosis with the medial head of triceps and retract this medially. The intramuscular aponeurosis can now be divided 2 cm proximal to its insertion on the olecranon, permitting access to the posterior distal humeral and posterior capsule (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark34)[Figure ](#bookmark34)7.17).       Figure 7.15 Creation of a fascial flap. (From Rajeev A, Pooley J, _Eur J Orthop Surg Traumatol_. 2009;19:467–472.) _Procedure_ _Preparation of distal humerus and proximal ulna_ ## [The forearm is rotated laterally to allow exposure of the distal humerus. The radial head and tip of olecranon, along a line tangent to the posterior-most portion of the olecranon articulation, are excised with an oscillating saw (](#bookmark35)Figure 7.18). ## [To mark the humeral saw cuts, the olecranon fossa guide is available on the instrument set. To orientate the guide, the shaft of the fossa guide is aligned with the humeral canal. The medial border should lie along the medial trochlea. The guide should also align with the anatomical internal rotation of the trochlea, which approximates the flat surface posterior and just proximal to the olecranon fossa. Using a fossa reamer or burr, a hole is created and an oscillating saw is used to remove the remains of the trochlea, along the lines previously marked, allowing access to the medullary canal of the humerus (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark36)[Figure ](#bookmark36)7.19). ## [The canal is identified with a high-speed rotating bur at the proximal aspect of the resection of the olecranon fossa in a proximal direction (](#bookmark37)Figure 7.20). Open the medullary canal to a size sufficient to allow a humeral rasp (about 4 mm). ## [The humeral rasps are now used to prepare the humeral canal (](#bookmark38)Figure 7.21). Serial rasps increasing in size are used until cortical resistance is met. If a rasp is unable to be advanced fully, use an implant corresponding to the largest size of rasp which was fully introduced.               Figure 7.16 Retraction of the lateral head of triceps, together with anconeus. (From Rajeev A, Pooley J, _Eur J Orthop Surg Traumatol. 2009;19:467–472.)_ The medial and lateral portions of the supracondylar columns _must be preserved_[during the preparation of the distal humerus. They act as points of reference to ensure satisfactory orientation and alignment. The trial prosthesis is inserted until the margins of the prosthesis are exactly level with the epicondylar articular surface margin on the capitellar and trochlear sides (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark39)**[Figure** ](#bookmark39)**7.22**). Further small pieces of bone are removed with rongeurs or bone nibblers from the distal humerus to aid proper seating of the component. ## [A high-speed burr is used at an angle of roughly 45° from the vertical in a posterior and distal direction to remove subchondral bone to identify the ulnar medullary canal. Serial rasps are introduced into the medullary canal of the ulnar until cortical resistance is met (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark40)[Figure ](#bookmark40)7.23). As with the humerus, the size of implant used corresponds with the largest size of rasp fully inserted. The appropriate rasps are used to shape the proximal ulna, maintaining vigilance to ensure the rasps are aligned down the medullary canal to avoid angular malpositioning. After the proximal ulna and distal humerus have been prepared, a trial will evaluate the elbow for complete flexion and extension. During trialling, inspect the anterior flange of the humeral component. If there is a space between the anterior humeral cortex and Lateral head triceps Anconeus     Figure 7.17 Division of tricipital intermuscular septum, 2 cm proximal to its insertion on the olecranon. (From Rajeev A, Pooley J, _Eur J Orthop Surg Traumatol_. 2009;19:467–472.)   Figure 7.18 Radial head and tip of olecranon excised. the flange, an allogenic or autologous (from the excised trochlea) bone graft may be used for added rotational stability. The bone graft should measure roughly 1.5 cm × [1 cm, and 2–3 mm in depth and can be placed in the space during cementation to establish contact between the flange and the bone (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark41)**[Figure** ](#bookmark41)**7.24**). The medullary canals are cleaned with pulsatile lavage and the canals dried. A cement restrictor is inserted into both canals. A cement gun is used for retrograde insertion of low-viscosity cement into the canals. If the components are cemented separately, the ulnar component is inserted first. The centre of the ulnar component is aligned with the centre             Figure 7.19 Use of guide, fossa reamer and oscillating saw to prepare the humerus.        Figure 7.20 A high-speed burr is used to identify the humeral canal.  Figure 7.21 Rasping the humeral canal.  Figure 7.22 Trial of the humeral component.  Figure 7.23 Rasping of the ulnar metaphysis. Anterior flange Cortical bone graft Anterior humerus   Figure 7.24 A cortical bone graft can be placed under the anterior flange of the humeral component if there is a gap between the prosthesis and bone. ## [of the sigmoid fossa. The humeral component is impacted down to a point that allows articulation of the device and the placement of the axle and the locking clip or interlocking axis pins (if a linked device is used) (](#bookmark42)Figure 7.25). The arm is held in extension until the cement has cured, then the humeral device can be linked with the ulnar component. _Closure_ The soft tissues that were dissected deeply in each approach are repaired with absorbable sutures (number 2 gauge). The olecranon osteo-periosteo-fascial medallion is repaired by transosseous non-absorbable sutures (number 2 gauge) to the olecranon. A suction drain is placed deep to the triceps muscle. The triceps aponeurosis and antebrachial fascia are closed with the elbow flexed at 90° flexion using absorbable braided number 1 interrupted sutures (continuous suturing reduces the ‘give’ of the tendon during assisted motion).                 Figure 7.25 Implanted components. [View Source / PubMed]
- 1. The skin is closed with a dermal supporting absorbable suture and an absorbable continuous subcuticular suture plus Steri-Strips. [View Source / PubMed]
- 2. An occlusive dressing is applied with the elbow in 90° of flexion. [View Source / PubMed]
- 3. A bulky wool and crepe bandage dressing is applied in two layers. Postoperative care and instructions The drain, wool and bandage are removed after 24 hours. Supervised physiotherapy should allow active- and gravity-assisted extension, as well as active and passive flexion, pronation and supination. It is the authors’ practice to apply a removable extension splint, which the patient can wear at night for 6 weeks in order to maintain full extension. The wound should be checked for any signs of abnormal healing or infection at 2 weeks, after which surgical follow-up is recommended at 6 weeks, at which point the patient can begin strengthening exercises. Thereafter, follow-up should be at 6 months and 1 year after surgery, then at yearly intervals if required. The patient should be advised to return to clinic if there is pain or functional deterioration. Patients are recommended to avoid lifting with the ipsilateral limb objects weighing more than 1 kilogram on a regular basis or lifting more than 5 kg on a single event. Recommended references Rajeev A, Pooley J. A posterior approach to the elbow joint based on the blood supply to the triceps muscle. _Eur J Orthop Surg Traumatol_. 2009;19:467–472. Sanchez-Sotelo J. Total elbow arthroplasty. _Open Orthop J_. 2011;5:115–123. Sanchez-Sotelo J. Primary elbow arthroplasty: Problems and solutions. _Shoulder Elbow_. 2016;9(1):61–70. Voloshin I, Schippert D, Kakar S et al. Complications of total elbow replacement: A systematic review. _J Shoulder Elbow Surg_. 2011;20(1):158–168. [Open elbow arthrolysis](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark13) Preoperative planning _Indications_ [View Source / PubMed]
- 4. Post-traumatic capsular contracture of the ulnohumeral (medial column), radiocapitellar (lateral column), and proximal radioulnar joints (anterior and posterior compartments) [View Source / PubMed]
- 5. Degenerative contracture of anterior and posterior compartments [View Source / PubMed]
- 6. Intracompartmental adhesiolysis, usually of the radiocapitellar joint [View Source / PubMed]
- 7. In association with intra-articular corrective osteotomy of the distal humerus, proximal ulna or radial head [View Source / PubMed]
- 8. In association with joint replacement arthroplasty of the elbow, including lateral compartment resurfacing and radial head replacement _Contraindications_ [View Source / PubMed]
- 9. Vascular compromise of the limb [View Source / PubMed]
- 10. Infection (generalised or of the limb) [View Source / PubMed]
- 11. Compromised skin in the region of the surgical incision [View Source / PubMed]
- 12. Inability of the patient to understand the postoperative rehabilitation programme [View Source / PubMed]
- 13. Contraindication to regional nerve blockade; previous nerve trauma or palsy (particularly if incomplete nerve lesion) at the elbow or more proximally _Consent and risks_ [View Source / PubMed]
- 1. Ulnar nerve injury: 10% transient ulnar neuritis, 1% tardy ulnar nerve palsy, less than 1% acute permanent lesion [View Source / PubMed]
- 2. Infection: Less than 1% [View Source / PubMed]
- 3. Heterotopic ossification: 10% [View Source / PubMed]
- 4. Recurrence: More common in post-traumatic stiffness syndrome, less common in degenerative or inflammatory contractures [View Source / PubMed]
- 5. Failure to achieve desired result (due to surface/topographical articular lesions) [View Source / PubMed]
- 6. Need for further surgery, including joint replacement arthroplasty Operative planning Anteroposterior and lateral (in flexion and extension) radiographs, less than 6 months old, should be available. For articular surface lesions a computed tomography (CT) arthrogram is desirable. It should be possible to readily convert from an arthroscopic procedure to an open procedure (see positioning and incision sections). _Anaesthesia and positioning_ Anaesthesia and positioning are the same as for radial head replacement and total elbow arthroplasty. Surgical technique Arthrolysis can be performed open or arthroscopically. _Open arthrolysis_ The choice of approach is governed by which compartment is to be accessed: [View Source / PubMed]
- 14. _For the lateral compartment, plus anterior and posterior capsule : The lateral column (Morrey) approach can be used. This is equivalent to the proximal half of the extended Kocher approach and can be extended proximally into a lateral approach to the humerus and distally into a Kocher approach to the radial head and neck. The_ anterolateral compartment is readily accessible (see section ‘Radial head replacement’, p. 113). [View Source / PubMed]
- 15. _For the medial side of the anterior compartment : The direct medial approach anterior to the ulnar nerve (see section ‘Tennis/golfer’s elbow release’, p. 142)._ [View Source / PubMed]
- 16. _For the anterior compartment alone(e.g. for lengthening of the biceps tendon):_ ## [The anterior approach. This is a lazy-S incision respecting the flexure crease of the elbow, passing from medial to the tendon of the biceps proximally over the brachial neurovascular bundle, to the medial side of the ‘mobile wad’ (of Henry) distally (](#bookmark44)Figure 7.26). Incision Figure 7.26 Anterior approach. [View Source / PubMed]
- 17. _For the dorsal (olecranon fossa) compartment and ulnar nerve : A dorsal (trans-tricipital) approach may be used, as for elbow arthroplasty. The anterior compartment may then be accessed via a transhumeral approach by making an aperture in the olecranon fossa (the Outerbridge-Kashiwagi or OK procedure)._ _Column procedure_ This procedure provides access to the anterior and posterior capsule, as well as to the coronoid and olecranon, should osteophyte excision be required. The incision can be extended distally to readily access the radiocapitellar joint. _Superficial dissection_ ## [The superficial dissection is the same as for Kocher’s extended approach, but using only the proximal half of the incision (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark45)[Figure ](#bookmark45)7.27). If access to the medial side is required (e.g. preoperative ulnar nerve symptoms necessitating release or transposition) or a posterior approach has previously been used, then a dorsal skin incision can be used with subcutaneous dissection to the lateral aspect in order to expose the column. Lateral supracondylar ridge, the “column”     Figure 7.27 The distal lateral humerus that is proximal to the lateral epicondyle is termed ‘the column’. _Deep dissection_ Release of the origin of ECRL and the distal origin of brachioradialis from the lateral column on the humerus permits access to the superolateral anterior capsule. The brachialis muscle can be swept away from the capsule with a periosteal elevator, which can now be entered at the radiocapitellar joint. Careful retraction will protect the brachialis muscle, median nerve and brachial artery, allowing the anterior capsule to be excised to at least the level of the coronoid. Anterior (coronoid) osteophytes may be excised if required, and the articular surface of the trochlea can be visualised. If there is still a significant fixed flexion deformity or lateral radiographs identify posterior osteophytes, then the triceps can be elevated from the posterior aspect of the column with Lateral column Anterior capsular release Coronoid osteophyte Posterior capsular release Olecranon osteophyte   Figure 7.28 The column procedure, with both anterior and posterior releases demonstrated. ## [epifascial dissection. The posterior capsule may then be released, clearing the olecranon fossa of soft tissue and excising osteophytes from the olecranon, as needed (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark46)[Figure ](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark46)7.28). _Outerbridge-Kashiwagi procedure_ ## [The procedure begins as per the trans-tricipital approach to the distal humerus. An aperture is then made through the distal humerus using a high-speed burr, directing the burr radially and proximally: the medial humeral column is thinner and flatter than the lateral column, so the transhumeral opening should be directed radially immediately medial to the lateral column to avoid iatrogenic medial column fracture. The aperture should exit anteriorly immediately behind the tip of the coronoid process (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark47)[Figure ](#bookmark47)7.29).  Figure 7.29 The Outerbridge-Kashiwagi procedure. The diameter of the aperture should be no more than half the transverse diameter of the humerus at this level. The anterior capsule of the radiocapitellar joint, the coronoid tip, and most of the anteromedial capsule can be removed through the aperture, using elbow flexion to bring the capsule into the aperture. It is inadequate for release of the medial capsule, and the anterior band of the ulnar collateral ligament should not be incised, to avoid iatrogenic valgus instability. _Technical aspects_ Where total capsulectomy has been required in cases such as post-traumatic contracture, heterotopic ossification and myositis ossificans, the collateral ligaments are often released –the elbow is therefore unstable. Fixed splintage is counterproductive. Dynamic splintage is required: a hinged external fixator is indicated if the ligaments cannot be reattached and should be retained for about 8 weeks, before application of a removable hinged brace for a further 4 weeks. If the ligaments can be restored to their optimal tension an external hinged removable brace can be used. Re-fixation of the ligaments to their footprint origins is facilitated by one of the several varieties of anchors that are available. The elbow must be stable enough to permit full-range assisted sagittal motion with gravity eliminated immediately after the operation. _Closure_ A limited lateral release (e.g. anterior column procedure alone) may not require a drain; however, anything more extensive will warrant a suction drain placed deep to triceps. The triceps aponeurosis and antebrachial fascia are closed with the elbow flexed at 90° flexion using absorbable braided number 1 interrupted sutures (continuous suturing reduces the ‘give’ of the tendon during assisted motion). [View Source / PubMed]
- 18. The skin is closed with a dermal supporting absorbable suture and an absorbable continuous subcuticular suture plus Steri-Strips. [View Source / PubMed]
- 19. An occlusive dressing is applied with the elbow in 90° of flexion. [View Source / PubMed]
- 20. A bulky wool and crepe bandage dressing is applied in two layers. Arthroscopic arthrolysis _Landmarks_ [View Source / PubMed]
- 21. Lateral epicondyle [View Source / PubMed]
- 22. Radial head [View Source / PubMed]
- 23. Tip of the olecranon _Approach_ The usual portals (as described in the section ‘Elbow arthroscopy’, p. 154) are used. In principle the arthroscopic portals respect the same incisions, i.e. the portals are placed in the line of the standard skin incisions to permit extension into an open approach as required. Using the anteromedial and anterolateral portals, fibrous tissue can be resected from the anterior part of the joint, using a combination of a full-radius resector and electrocautery. Any loose bodies are removed. The coronoid fossa is re-created, using the resector and a burr for any bony hypertrophy. The coronoid tip is removed if there is evidence of coronoid impingement. The resector is used to strip the capsule proximally, off the distal humerus, for approximately 2.5 cm proximal to the olecranon fossa until the fibres of brachialis come into view proximally. To complete the release a 1 cm capsulotomy of the anterior capsule from medial to lateral is required. Using the direct posterior and posterolateral portals, the posterior compartment is debrided similarly. The scope enters through the posterolateral portal and the resector or burr through the direct posterior portal to complete the procedure. Careful release of the contracture, with a full-radius resector, releases the posteromedial and posterolateral gutters. Beware of the ulnar nerve in close proximity medially. Manipulation of the elbow is used to achieve maximum extension. _Closure_ [View Source / PubMed]
- 24. A drain is placed in the direct posterior portal and the portals closed with absorbable sutures. [View Source / PubMed]
- 25. Occlusive dressings are applied. [View Source / PubMed]
- 26. The elbow is splinted in maximum extension. Postoperative care and instructions The arm is rested on pillows at chest height for 48 hours. The bandage is reduced at 24 hours and the drain is removed. A Tubigrip bandage is applied. If there is uncertainty about elbow stability a removable extension splint may be applied, to be worn between exercise periods. Active assisted sagittal full-range motion exercises are performed for 20 minutes four or five times per day. Fist gripping and forearm pronosupination are undertaken as comfort permits. Supervised physiotherapy for the neck, shoulder and hand is undertaken. If achieving extension is problematic, then a removable elbow splint or brace can be applied at night. Active unassisted movement is permitted by 6 weeks and axial weightbearing at approximately 12 weeks. Passive motion of the elbow may be indicated for recalcitrant/ recurrent arthrofibrosis. However, continuous passive motion equipment is difficult to apply accurately, particularly in the unstable joint. A continuous patient-controlled analgesic infusion, or continuous infraclavicular regional anaesthetic infusion are commonly required. Recommended references Mansat P, Morrey BF. The column procedure: A limited lateral approach for extrinsic contracture of the elbow. _J Bone Joint Surg Am_. 1998;80(11):1603–1615. Morrey BF. The posttraumatic stiff elbow. _Clin Orthop Relat Res_. 2005;(431):26–35. Nandi S, Maschke S, Evans PJ, Lawton JN. The stiff elbow. _Hand (NY)_. 2009;4(4):368–379. [Tennis/golfer’s elbow release](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark14) Preoperative planning _Indications_ Tennis and golfer’s elbow release is indicated when conservative management has failed. They are erroneously termed lateral and medial epicondylitis, though do not feature an inflammatory reaction; instead, it is a degenerative process in the tendons involving immature fibroblasts. Patients with tennis elbow have tenderness at the common extensor origin, with reproduction of symptoms upon resisted wrist extension with the elbow in extension. Non-operative treatment with anti-inflammatories, counterforce bracing and up to three steroid injections to the site of maximal tenderness can achieve success in up to 95% of cases. The ECRB tendon is invariably affected, though the tendon of extensor digitorum communis (EDC) may also be affected in up to 35% of cases and therefore should not be neglected. Tennis elbow occurs at least five times more commonly than golfer’s elbow. In golfer’s elbow, pain and tenderness are localised to the common flexor origin. Pain is reproduced by resisted forearm pronation and wrist flexion. Non-operative treatment is similar to that for tennis elbow but usually more difficult to treat. A number of operative methods have been developed, including open, arthroscopic and percutaneous debridement. Of note, platelet-rich plasma injections have shown promise as a therapeutic intervention and demonstrate greater symptomatic relief than steroid injections alone. Over 90% of patients do not require surgical intervention; of those that do, 85%–95% experience symptomatic relief from any of the above surgical procedures, and there is little evidence to suggest one is conclusively superior to the others. Arthroscopic debridement may be incomplete if much of the pathology is extra-articular, potentially resulting in ongoing pain. Some recent evidence suggests that surgical debridement for tennis elbow may not even have any benefit over sham surgery (i.e. no debridement of the degenerative tendon), though the evidence is not yet conclusive and research is ongoing. Nonetheless, we delineate the operative process for an open debridement of both pathologies. _Consent and risks_ [View Source / PubMed]
- 1. Failure [View Source / PubMed]
- 2. Nerve injury: 1% [View Source / PubMed]
- 3. Infection [View Source / PubMed]
- 4. Heterotopic ossification at surgical site: 10% [View Source / PubMed]
- 5. Posterolateral instability: If there is excessive debridement of the collateral ligament origins as well as the origins of the extensor muscles from the lateral epicondyle Operative planning Recent anteroposterior and lateral radiographs of the elbow should be available to rule out lateral compartment arthrosis with suspected tennis elbow. Calcification may be visible in the flexor origin in long-standing golfer’s elbow. _Anaesthesia and positioning_ Anaesthesia is usually general, but may be regional or combined. The supine position is used with the arm placed on an arm board. A pneumatic tourniquet or S-MART bandage/ tourniquet is used. The elbow should be sufficiently mobile for appropriate movement intraoperatively. The surgical field is prepared with a germicidal solution. Waterproof drapes are used with adhesive edges to provide a seal to the skin. Surgical technique _Extensor origin debridement (tennis elbow)_ _Landmark_ The lateral epicondyle is a landmark. _Incision_ ## [A 4–5 cm gently curved skin incision is made centred over the lateral epicondyle (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark49)[Figure ](#bookmark49)7.30). Lateral epicondyle  Figure 7.30 Tennis elbow skin incision. _Superficial dissection_ The incision is continued through subcutaneous fat and down to fascia. The fascia overlying the posterior edge of ECRL is incised and elevated to expose extensor carpi radialis brevis (ECRB), which lies beneath ECRL. Just posterior to ECRL lies the extensor aponeurosis, the anterior edge of which may be abnormal. ECRL is then dissected sharply off the anterior ridge and displaced anteromedially to expose ECRB. ECRB is inferior to the origin of ECRL and deep to EDC. The border between ECRB and EDC is often poorly defined. _Deep dissection_ ## [Degenerate tissue is excised, taking care not to release any normal looking tendon. The procedure is therefore more accurately a debridement than a release. The abnormal tissue may appear fibrillated or discoloured and may contain calcium deposits. The bony site of the ECRB resection (i.e. not the lateral epicondyle) is decorticated with an osteotome, bone nibbler or drill to enhance blood supply and theorised to fill the void with fibrous tissue (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark50)[Figure ](#bookmark50)7.31). (a) Removal of degenerative tissue, ECRB Lateral epicondyle   (b) Healthy ECRB distally Common extensor origin   Figure 7.31 Tennis elbow debridement and decortication. (_Continued_) (c) Decortication with drill Lateral epicondyle   _Closure of lateral approach_ Figure 7.31 (Continued) The defect between the posterior edge of ECRL and the extensor aponeurosis is repaired with an absorbable suture to restore the normal anatomical position. Superficial closure utilises absorbable sutures to approximate the subcutaneous fat, then a subcuticular continuous absorbable suture. An occlusive dressing is applied, followed by a bulky wool and crepe bandage dressing in two layers. _Postoperative care and instructions_ Dressings are reduced at 48 hours. Early range-of-motion exercises are begun, followed by strengthening exercises. Strenuous activity is resumed within pain limits at 8–10 weeks, and full power should have returned by 3 months. Follow-up is recommended at 6 weeks, with a wound check by the primary care practitioner at 2 weeks. _Flexor origin debridement (golfer’s elbow)_ _Landmark_ The medial epicondyle is the landmark. _Structures at risk_ [View Source / PubMed]
- 1. Medial antebrachial cutaneous nerve  Medial antebrachial cutaneous nerve Ulnar nerve Medial epicondyle          _Incision_ Figure 7.32 Golfer’s elbow skin incision. ## [A 3–4 cm longitudinal skin incision is made just posterior to the medial epicondyle. This avoids sensory branches of the medial antebrachial cutaneous nerve anterior and distal to the medial epicondyle (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark51)[Figure ](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark51)7.32). _Dissection_ ## [The incision is continued through subcutaneous fat and down to fascia exposing the common flexor origin. Partial debridement of the abnormal tendinosis tissue is usually all that is required, usually involving the flexor carpi radialis and medial side of pronator teres (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark52)[Figure ](#bookmark52)7.33). Any normal tissue attached to the medial epicondyle is left intact. _Closure of medial approach_ The defect in the flexor-pronator origin is closed with absorbable sutures. Superficial closure utilises absorbable sutures to approximate the subcutaneous fat, then a subcuticular continuous absorbable suture. An occlusive dressing is applied, followed by a bulky wool and crepe bandage dressing in two layers. _Postoperative care and instructions_ Dressings are reduced at 48 hours. Early mobilisation of the elbow should be encouraged in all patients. Follow-up is recommended at 6 weeks, with a wound check by the primary care practitioner at 2 weeks. The patient should be cautioned to return to the clinic if there is pain or functional deterioration. Degenerated tendon Flexor carpi ulnaris arcade Ulnar nerve Resection degenerated tendon                   Figure 7.33 Flexor origin debridement. Recommended references Amin NH, Kumar NS, Schickendantz MS. Medial epicondylitis: Evaluation and management. _J Am Acad Orthop Surg_. 2015;23(6):348–355. Kroslak M, Murrell GAC. Surgical treatment of lateral epicondylitis: A prospective, randomized, double-blinded, placebo-controlled clinical trial. _Am J Sports Med_. 2018;46(5):1106–1113. Pierce TP, Issa K, Gilbert BT et al. A systematic review of tennis elbow surgery: Open versus arthroscopic versus percutaneous release of the common extensor origin. _Arthroscopy_. 2017;33(6):1260–1268.e2. [Lateral collateral ligament reconstruction](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark15) The procedure for medial collateral ligament reconstruction was popularised by Jobe and then modified as the ‘docking’ procedure. Medial collateral ligament insufficiency is common in the United States, as a result of overhead throwing activities, particularly baseball. The lateral ulnar collateral ligament (LUCL) and remaining lateral collateral ligament (LCL) is typically the first structure to be injured during acute elbow dislocation which, despite appropriate initial management can lead to symptomatic posterolateral rotatory instability. The operative procedure for LUCL reconstruction was derived from the procedures on the medial side and therefore shares many similarities. We focus on the lateral side here. Preoperative planning _Indications_ [View Source / PubMed]
- 1. Symptomatic posterolateral instability in the presence of LCL insufficiency (acute or chronic) _Contraindications_ [View Source / PubMed]
- 2. Infection, generalised or localised around the site of surgery. [View Source / PubMed]
- 3. Inadequate bone and soft tissues around the reconstructive graft. [View Source / PubMed]
- 4. Open physes in children is considered a relative contraindication, though a modified technique has been described to avoid iatrogenic physeal injury. [View Source / PubMed]
- 5. Absence of a radial head has been shown to adversely affect outcomes; therefore, the procedure may still be performed with caution, or can be undertaken with a concurrent radial head replacement. _Consent and risks_ [View Source / PubMed]
- 1. _Inadequate tensioning : Ongoing instability or stiffness_ [View Source / PubMed]
- 2. _Nerve injury related to tendon donor site : Median palmar cutaneous nerve, saphenous nerve_ [View Source / PubMed]
- 3. Infection [View Source / PubMed]
- 4. Stress fracture [View Source / PubMed]
- 5. _Nerve injury in medial collateral ligament reconstruction : Transient ulnar neuropathy 5%–10%_ Operative planning Rarely in cases of acute injury there may be adequate capsule and ligamentous tissue remaining to permit repair, rather than reconstruction. In the case of reconstruction, choice of autograft or allograft is at the discretion of the operating surgeon. Autografts may be taken from the ipsilateral or contralateral side to the operative site. Described tendon grafts include palmaris, gracilis, plantaris, Achilles tendon (medial sliver) and the toe extensors. The presence of a palmaris tendon should be confirmed if planning to use this as an autograft (absent bilaterally in approximately 16% of patients and unilaterally in 22%). Diagnosis of posterolateral instability is made with discerning clinical assessment but can be aided with magnetic resonance (MR) imaging, including MR arthrogram. Fluoroscopic assessment can be useful to demonstrate lateral and posterolateral instability on stress tests. Finally, diagnostic arthroscopy may offer a conclusive answer in the face of diagnostic uncertainty. Surgical techniques include various fixation methods such as the figure-of-eight method, the docking procedure and use of an endo-button prosthesis, though all share the principle of defining a point of isometry on the lateral humerus. _Anaesthesia and positioning_ Anaesthesia and positioning is the same as for radial head replacement and TEA, though antibiotics are not routinely required. The entire forearm should be accessible if considering an ipsilateral autologous palmaris graft, otherwise prepare the required limb for the autograft of choice. If the palmaris longus tendon is absent and the surgeon still wishes to use an autograft, the leg should be prepped and draped to allow access to the knee for gracilis tendon harvesting. Surgical technique _Landmarks/incision/dissection_ The limited Kocher approach offers perfect exposure of the lateral ligament complex. The palmaris tendon can be visualised by opposing the thumb and little finger together and should be marked with a skin marker prior to the procedure. The distal flexor crease of the wrist will serve as the landmark for the tendon harvest. _Procedure_ ## [Onexposureofthedeficientcapsule/ligamentcomplex, thecapsuleisincisedlongitudinally, just anterior to the lateral ligament complex to visualise the radiocapitellar joint. The ulna is drilled at the distal attachment of the lateral ligament complex just anterior to the crest. A second drill hole should be made such that the perpendicular bisector of these two ulnar holes points towards the origin of the LUCL (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark54)[Figure ](#bookmark54)7.34). An angled bone curette can then create a bone tunnel between the two holes within the ulna. A suture is placed through the tunnel, held with a haemostat and extended towards the lateral epicondyle while taut. The elbow is taken through flexion and extension until the isometric point of origin on the humerus is found. The suture should remain taut throughout flexion and extension when held at this point. A point _just anterior to the isometric point_[is drilled to mark the origin of the ligament. Two tunnels should be drilled from this point, exiting posteriorly on the lateral epicondyle (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark55)**[Figure** ](#bookmark55)**7.35**). To obtain the palmaris tendon autograft, create a 10 mm transverse incision just proximal to the distal wrist crease over the palmaris longus tendon. Identify the tendon at this level, confirm that it is not the median nerve and harvest the tendon with a tendon stripper. The muscle can be removed from the tendon and the tendon doubled on itself to create a four-ply repair. ## [The doubled tendon is introduced through the ulnar tunnel and each of the arms can then be taken through one of the humeral tunnels to create a figure-of-eight. The elbow is reduced with a valgus and pronated position and the ends of the tendon can then be measured cut such that approximately 5 mm of the tendon lies within each humeral tunnel (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark56)[Figure ](#bookmark56)7.36).   Figure 7.34 Ulnar tunnels in a lateral ulnar collateral ligament reconstruction. The perpendicular bisector of the two ulnar tunnels joins the lateral ulnar collateral ligament origin on the humerus. A non-absorbable suture is placed in each end of the doubled tendon arm and locked. The capsule is then closed under the tendon graft, and it is imperative that the graft remains extracapsular. The sutures are introduced through the humeral tunnels and the elbow reduced once again in a valgus and pronated position, then the sutures tied together. Further tension is often required at this point, so the two limbs of the graft can be brought together side-to-side along the length of the tendon.                Figure 7.35 Humeral tunnels in a lateral ulnar collateral ligament reconstruction, isometric point arrowed.                       Figure 7.36 Five millimetres of the doubled tendon should lie within each humeral tunnel. _Closure_ Closure is routine as for radial head replacement, no drain is required. Postoperative care and instructions The elbow should be immobilised in a range-of-motion brace locked at 90° in full pronation for 2 weeks postoperatively. The wound should then be checked and the brace movement range progressively increased with supervised physiotherapy, keeping a 30° extension block until 6 weeks. The patient will be seen in a surgical clinic at 6 weeks and the brace can be removed. Resisted supination should be avoided for 3 months following surgery. Elbow strengthening exercises can begin at 3 months, together with any sport-specific rehabilitation protocol. The patient should be followed up again 6 months postoperatively. Most patients can return to sports at 4–6 months. Recommended references Anakwenze OA, Kancherla VK, Iyengar J et al. Posterolateral rotatory instability of the elbow. _Am J Sports Med_. 2014;42(2):485–491. Jones KJ, Dodson CC, Osbahr DC et al. The docking technique for lateral ulnar collateral ligament reconstruction: Surgical technique and clinical outcomes. _J Shoulder Elbow Surg_. 2012;21(3):389–395. [Elbow aspiration/injection](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark10) _Indications_ [View Source / PubMed]
- 1. Inflammatory arthritis and other arthropathies [View Source / PubMed]
- 2. Suspected infection [View Source / PubMed]
- 3. Haemarthrosis _Consent and risks_ [View Source / PubMed]
- 1. Nerve injury: Less than 1% [View Source / PubMed]
- 2. Infection: Less than 1% _Landmarks_ ## [Landmarks include radial head, lateral epicondyle, and tip of the olecranon (anconeus triangle) (](#bookmark58)Figure 7.37). _Approach_ The elbow can be entered either ulnarly or radially, but the radial approach is preferred in order to avoid ulnar nerve injury. _Procedure_ _Structure at risk_ [View Source / PubMed]
- 1. Radial nerve The skin is prepared with a germicidal solution. Prior to needle insertion, the elbow is flexed and the forearm pronated to protect the radial nerve. An 18G needle is inserted into the joint, through the soft spot at the centre of the anconeus triangle. With this approach the needle will penetrate only the anconeus and joint capsule. If the needle hits bone, it should be withdrawn slightly and redirected at a slightly different angle. If performing an injection, it is wise to aspirate first to ensure the needle is not in a blood vessel. Lateral epicondyle Radial head Olecranon process          Figure 7.37 Landmarks for elbow aspiration. Postoperative care and instructions An occlusive dressing is applied. Mobilisation of the joint depends on the underlying reason for aspiration/injection. Recommended references Cardone DA, Tallia AF. Diagnostic and therapeutic injection of the elbow region. _Am Fam Physician_. 2002;66(11):2097–2100. Foocharoen T, Foocharoen C, Laopaiboon M et al. Aspiration of the elbow joint for treating radial head fractures. _Cochrane Database Syst Rev_. 2014;(11):CD009949. [Elbow arthroscopy](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark12) Preoperative planning _Indications_ Elbow arthroscopy is indicated in a variety of painful conditions of the elbow. The most frequent are [View Source / PubMed]
- 4. Debridement for osteoarthritis [View Source / PubMed]
- 5. Osteochondritis dissecans of capitellum [View Source / PubMed]
- 6. Arthrolysis [View Source / PubMed]
- 7. Removal of loose bodies [View Source / PubMed]
- 8. Synovectomy or synovial biopsy [View Source / PubMed]
- 9. Septic arthritis [View Source / PubMed]
- 10. Radial head resection [View Source / PubMed]
- 11. Diagnostic _Contraindications_ [View Source / PubMed]
- 12. Infection of overlying skin [View Source / PubMed]
- 13. Bony or severe fibrous ankylosis [View Source / PubMed]
- 14. Caution should be taken by the operating surgeon in cases of previous trauma and surgical management as distorted anatomy may predispose nerve injury _Consent and risks_ [View Source / PubMed]
- 1. Nerve injury [View Source / PubMed]
- 2. _Infection : Less than 1%; risk is low, so prophylactic antibiotics are not routinely recommended_ _Operative planning_ Recent radiographs and, where taken, MR images and MR arthrograms, should be available. The correct equipment must be available, and this should be checked by the surgeon. A 30° 4 mm arthroscope should be used. The water flow should be controlled with an inflow pump. _Anaesthesia and positioning_ Anaesthesia is general or combined with regional. The lateral decubitus position is used, the position being maintained by side supports. The tourniquet is applied high around the arm, and the arm is placed over a bolster applied to the bed. The elbow should be free to flex to 90° with the hand pointing towards the floor. The TV monitor is placed on the opposite side of the patient. The surgical field is prepared with a germicidal solution. Waterproof drapes are used with adhesive edges to provide a seal to the skin. Surgical technique _Landmarks_ Palpable landmarks are outlined with a marker pen: [View Source / PubMed]
- 15. Lateral epicondyle [View Source / PubMed]
- 16. Radial head [View Source / PubMed]
- 17. Tip of the olecranon [View Source / PubMed]
- 18. Medial epicondyle [View Source / PubMed]
- 19. Ulnar nerve _Portals_ ## [The direct lateral portal is located in the soft spot at the centre of the triangle formed by the lateral epicondyle, radial head and tip of the olecranon, as for an elbow aspiration (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark60)[Figure ](#bookmark60)7.38, see section ‘Elbow aspiration/injection’, p. 152). This portal traverses the anconeus muscle. The elbow is initially distended through this portal. Proximal anterolateral portal Posterior antebrachial cutaneous nerve Lateral epicondyle Radial nerve Mid-lateral portal Lateral antebrachial cutaneous nerve Midanterolateral portal Anterolateral portal     Figure 7.38 Lateral portals for elbow arthroscopy. _Distal anterolateral portal_ This portal is usually established first after elbow distension. It is used for instrumentation as well as visualisation of the lateral aspect of the radial head. With the elbow flexed to 90° the portal is located 3 cm distal and 1–2 cm anterior to the lateral epicondyle. This should bring the portal just anterior and proximal to the radiocapitellar articulation. The skin incision is made with a number 11 blade and a haemostat used to bluntly dissect down to the joint capsule. This portal traverses the extensor carpi radialis brevis muscle. A blunt trochar is used to enter the joint with the portal driven toward the centre of the trochlea. The elbow joint _must be distended prior to trochar insertion and kept at 90° flexion during insertion_ since extension brings the radial nerve closer to the joint (3–7 mm). _Structure at risk_ [View Source / PubMed]
- 1. Radial nerve _Proximal anterolateral portal_ This is located 2 cm proximal and 1 cm anterior to the lateral epicondyle. It is further from the radial nerve than other anterolateral portals. It allows for excellent views of the anterior radiohumeral and ulnohumeral joints as well as the anterior capsular margin. _Anteromedial portal_ _Structure at risk_ [View Source / PubMed]
- 1. Median nerve Some surgeons prefer to establish this portal first. The elbow should be flexed to 90° as the portal is established. It is situated 2 cm anterior and 2 cm distal to the medial epicondyle. It must be placed _under direct vision_ : The median nerve lies 1–2 cm anterior and lateral to this portal. _Proximal anteromedial portal_ _Structures at risk_ [View Source / PubMed]
- 1. Median nerve [View Source / PubMed]
- 2. Ulnar nerve [View Source / PubMed]
- 3. Medial brachial cutaneous nerve [View Source / PubMed]
- 4. Medial antebrachial cutaneous nerve [View Source / PubMed]
- 5. Brachial artery This portal allows visualisation of the anterior elbow including the anterior joint capsule, medial condyle, coronoid process, trochlea, capitellum and radial head. The joint should already be distended with fluid and the ulnar nerve identified before establishing this portal. The portal is established using a longitudinal skin stab incision and blunt dissection 2 cm proximal to the medial epicondyle and immediately anterior to the intermuscular septum. The trochar is inserted over the anterior surface of the humerus aiming towards the radial head. Contact is maintained with the anterior surface of the humerus _to avoid neurovascular damage_. The ulnar nerve lies 4 mm from the portal. The median nerve lies 7–20 mm from the portal with the elbow in flexion. _Posterolateral portal_ _Structures at risk_ [View Source / PubMed]
- 1. The posterior antebrachial or lateral brachial nerves can be damaged with deep incisions. This is 3 cm proximal to the olecranon tip and just lateral to the border of the triceps tendon. _Direct posterior portal_ _Structures at risk_ [View Source / PubMed]
- 1. The ulnar nerve, if placed too medially This is 3 cm proximal to the olecranon tip and 2 cm medial to the posterolateral portal. It is _established under direct vision[with the arthroscope in the direct lateral portal (](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark61)**[Figure** ](#bookmark61)**7.39**)._ Ulnar nerve Medial antebrachial cutaneous nerve Superomedial portal Medial epicondyle Anteromedial portal Median nerve Brachial artery    Figure 7.39 Medial portals for elbow arthroscopy. _Procedure_ A systematic approach is essential if pathology is not to be missed. To distend the capsule, 15–25 mL of fluid is instilled into the joint through the direct lateral portal using an 18G needle. Backflow of fluid confirms correct placement. The anterolateral portal is established (see earlier) and the arthroscope and cannula inserted. The capsule medial to the articulation is examined first. Medial laxity can be assessed by supinating the forearm and applying valgus stress to the elbow in varying degrees of flexion. Flexing and extending the elbow allows the trochlea to be viewed. The radioulnar articulation is observed as the forearm is rotated and, for coronoid impingement, as the elbow is fully flexed. The anteromedial portal is established under direct vision and the arthroscope introduced to view the radioulnar and radiocapitellar articulations plus the annular ligament. Extending the elbow reveals more of the capitellum, and forearm rotation exposes more of the radial head. The anterolateral gutter and capsule should also be examined. Next, the direct lateral portal is established. Via this portal, the radial head (concave) is viewed, articulating with the capitellum (convex). The articulation between the olecranon and the trochlea is also well seen. Finally, through the posterolateral portal, the olecranon fossa, olecranon tip and posterior trochlea are examined. Loose bodies and osteophytes are sought, particularly on the olecranon tip. Specific instruments can be used for removal of loose bodies or debridement. _Closure_ Non-absorbable suture is used to close the skin defects. Occlusive dressings are applied. A wool and crepe bandage pressure dressing is used. Postoperative care and instructions The pressure dressing is removed at 48 hours. The patient mobilises the elbow fully following a diagnostic arthroscopy. Recommended references Kelly EW, Morrey BF, O’Driscoll SW. Complications of elbow arthroscopy. _J Bone Joint Surg Am_. 2001;83-A(1):25–34. Steinmann SP. Elbow arthroscopy: Where are we now? _Arthroscopy_. 2007;23(11):1231–1236. [_Viva question_](file:///C:/Users/DELL/Desktop/hip/quick%20fact/7.%20Surgery%20of%20the%20Elbow_Converted.html#bookmark13) 1\. Could you inform us of how many questions are required and the format of the questions? It would be helpful to see examples of questions from other chapters in order to keep the style consistent. [View Source / PubMed]
