Introduction and Biomechanical Rationale
The subscapularis is the largest and most powerful of the rotator cuff muscles, providing more than 50% of the total cuff strength. It functions as the primary internal rotator of the glenohumeral joint and serves as a critical dynamic anterior stabilizer. Biomechanically, the subscapularis works in concert with the infraspinatus to create a transverse force couple that compresses the humeral head into the glenoid concavity during shoulder elevation.
Disruption of the subscapularis tendon severely compromises this force couple, leading to altered glenohumeral kinematics, superior and anterior humeral head migration, and accelerated degenerative changes. Historically, subscapularis tears were underdiagnosed and often treated via open approaches. However, advancements in arthroscopic techniques, specifically the systematic approaches pioneered by Burkhart and Tehrany, have revolutionized the management of these lesions, allowing for anatomic restoration with minimized surgical morbidity.
Clinical Pearl: When a subscapularis tear is identified in the setting of a massive rotator cuff tear, it must be repaired first before addressing the supraspinatus or infraspinatus. This maximizes visualization and working space in the confined anterior compartment.
Preoperative Evaluation and Setup
Clinical Assessment
Patients typically present with anterior shoulder pain, weakness in internal rotation, and increased passive external rotation compared to the contralateral side. Provocative testing is essential:
* Lift-Off Test (Gerber): Evaluates the lower functional portion of the subscapularis.
* Belly-Press Test: Highly sensitive for upper subscapularis tears.
* Bear-Hug Test: Maximizes the internal rotation force required, making it highly sensitive for subtle, partial articular-sided tears.
Patient Positioning and Anesthesia
The procedure is typically performed under general anesthesia supplemented with an interscalene regional nerve block to minimize postoperative narcotic requirements. The patient can be positioned in either the lateral decubitus or the beach chair position. The beach chair position is often preferred by many surgeons for subscapularis repair as it allows for unhindered rotation of the arm, which is critical for visualizing the lesser tuberosity footprint and mobilizing the tendon.
Surgical Technique: The Burkhart and Tehrany Approach
Portal Placement
Optimal portal placement is the cornerstone of a successful arthroscopic subscapularis repair. A dedicated four-portal technique is utilized to ensure adequate viewing angles and appropriate trajectory for instrumentation.
- Posterior Portal: Used primarily for arthroscopic viewing. It provides an excellent panoramic view of the subscapularis tendon and its bone bed on the lesser tuberosity.
- Anterior Portal: Established via an outside-in technique through the rotator interval. This portal is utilized for anchor placement and suture passage.
- Anterolateral Portal: Placed just anterior to the biceps tendon. This is the primary working portal for subscapularis mobilization and preparation of the bone bed.
- Accessory Anterolateral Portal: Placed just posterior to the biceps tendon. This portal is dedicated to managing traction sutures, which are essential for controlling the tendon during mobilization and repair.
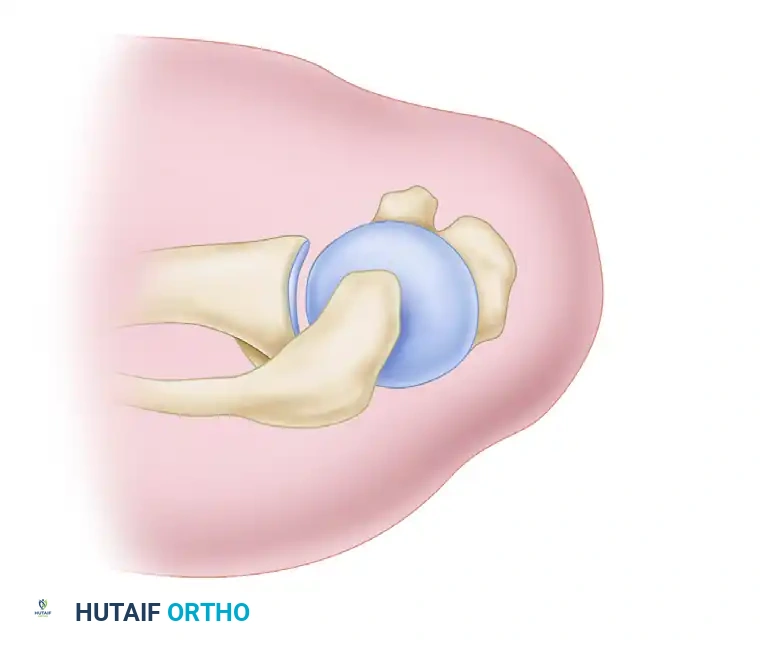
Figure 1: Burkhart and Tehrany portals for arthroscopic subscapularis repair. (A) Anterior portal for anchor placement. (B) Anterolateral portal for mobilization. (C) Accessory anterolateral portal for traction sutures. (D) Posterior portal for viewing.
Diagnostic Arthroscopy and Tear Recognition
With the arthroscope in the posterior portal, a thorough diagnostic sweep is performed. Subscapularis tears can be notoriously difficult to visualize, particularly partial tears or chronic retracted tears that have scarred medially.
To vary the field of view and expose hidden lesions, the surgeon must dynamically manipulate the arm. Abduction, internal rotation, and external rotation are utilized.
* Internal Rotation: Highly useful for enhancing the visualization of partial tears by relaxing the intact, tensioned portion of the subscapularis.
* Estimating Tear Size: For partial tears, the percentage of the torn tendon can be estimated by evaluating the superior-to-inferior dimension of the "bare footprint" (the exposed bone bed on the lesser tuberosity).
Surgical Warning: In chronic, retracted subscapularis tears, the tendon edge is often located far medially, sometimes retracting to the level of the glenoid rim. It can blend with the anterior capsule, making it difficult to recognize.
The "Comma Sign"
When facing a retracted tear, the surgeon must actively search for the "comma sign." In retracted subscapularis tears, the medial sling of the biceps—composed of the superior glenohumeral ligament (SGHL) and a portion of the coracohumeral ligament (CHL)—is torn from its humeral attachment at the upper border of the subscapularis footprint. However, it remains attached to the superolateral portion of the subscapularis tendon. As the tendon retracts medially, this capsuloligamentous complex forms a distinct, comma-shaped arc just above the superolateral corner of the subscapularis. Identifying this comma tissue is the key to locating the superolateral edge of the retracted tendon. Once identified, a tendon grasper is used to pull the medially retracted tissues laterally until positive identification of the upper border is confirmed.
Management of the Long Head of the Biceps Tendon (LHBT)
The LHBT is intimately associated with the subscapularis. Pathology of the subscapularis almost universally compromises the biceps pulley, leading to biceps instability.
* Partial Tears: Perform aggressive arthroscopic débridement or tenotomy.
* Subluxation/Dislocation: If the biceps is unstable (subluxated medially into the joint or dislocated), an arthroscopic tenotomy or tenodesis must be performed to eliminate a persistent source of anterior shoulder pain and to prevent the biceps from mechanically interfering with the subscapularis repair.
Interval Slide and Tendon Mobilization
For massive, contracted rotator cuff tears involving the subscapularis, an interval slide technique (as described by Tauro et al.) may be necessary to allow lateral excursion of the tendon without undue tension.
Figure 2: Basket punch inserted through the lateral subacromial portal to begin the interval release.
Figure 3: Completed interval slide release for a crescentic tear.
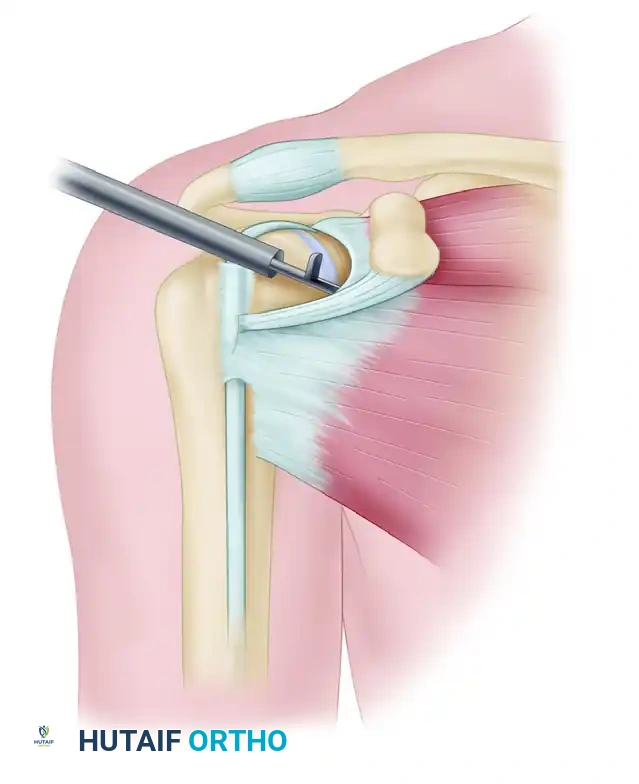
Figure 4: Completed interval slide release for a longitudinal tear.
Three-Sided Release
In isolated tears, the muscle-tendon unit is generally not severely retracted and may not require extensive mobilization. However, massive combined tears (subscapularis, supraspinatus, infraspinatus) almost always require aggressive mobilization.
If the tendon cannot be easily reduced over the bone bed on the lesser tuberosity, a systematic release is performed:
1. Pass a traction suture through the superolateral edge of the subscapularis tendon.
2. Bring an arthroscopic elevator through the anterolateral portal.
3. While exerting lateral traction on the tendon via the accessory anterolateral portal, use the elevator to mobilize the anterior, posterior, and superior aspects of the subscapularis.
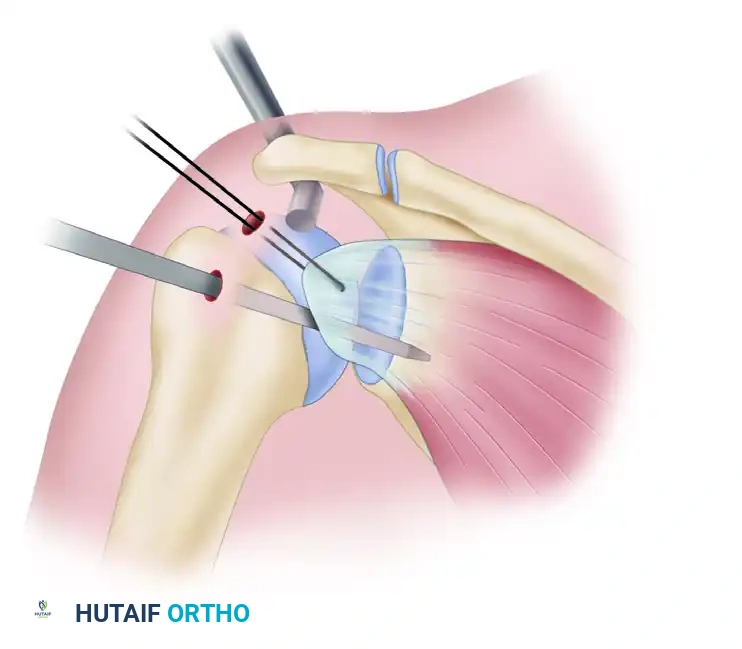
Figure 5: Superior view of subscapularis mobilization using an arthroscopic elevator while applying tension via a traction suture.
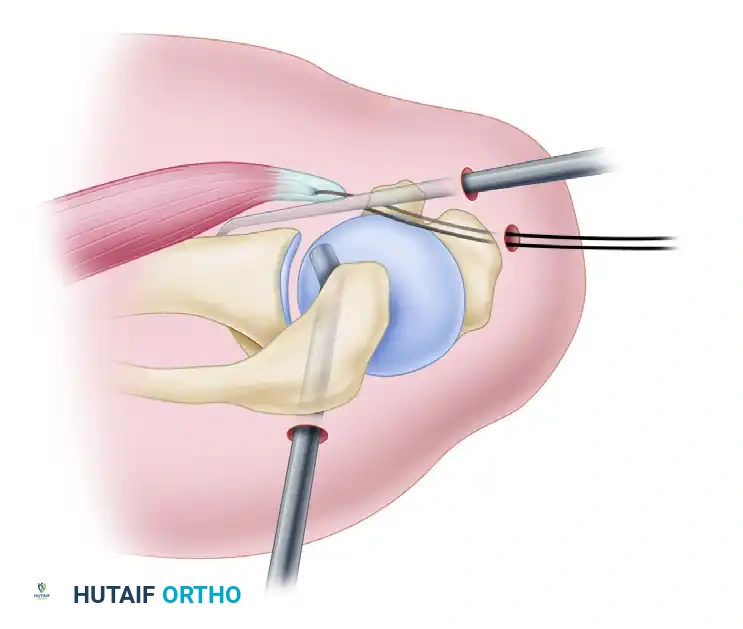
Figure 6: Anterior view demonstrating the elevator freeing the capsular adhesions from the subscapularis.
Surgical Pitfall - The Axillary Nerve: You must strictly avoid dissecting or cutting near the inferior border of the subscapularis tendon. The axillary nerve and posterior humeral circumflex vessels run dangerously close to this inferior margin. By freeing the anterior, posterior, and superior borders, lateral traction on the tendon will effectively and safely disrupt any remaining inferior adhesions through blunt tension, minimizing the risk of catastrophic neurovascular injury.
Preparation of the Bone Bed
A robust healing response requires a meticulously prepared bleeding bone bed.
1. Introduce a high-speed arthroscopic burr through the anterolateral portal.
2. Decorticate the lesser tuberosity footprint.
3. To maximize tendon-to-bone contact and reduce tension on the repair, medialize the bone bed by approximately 5 mm. This is achieved by removing the articular cartilage at the medial margin of the footprint down to a bleeding cancellous base.
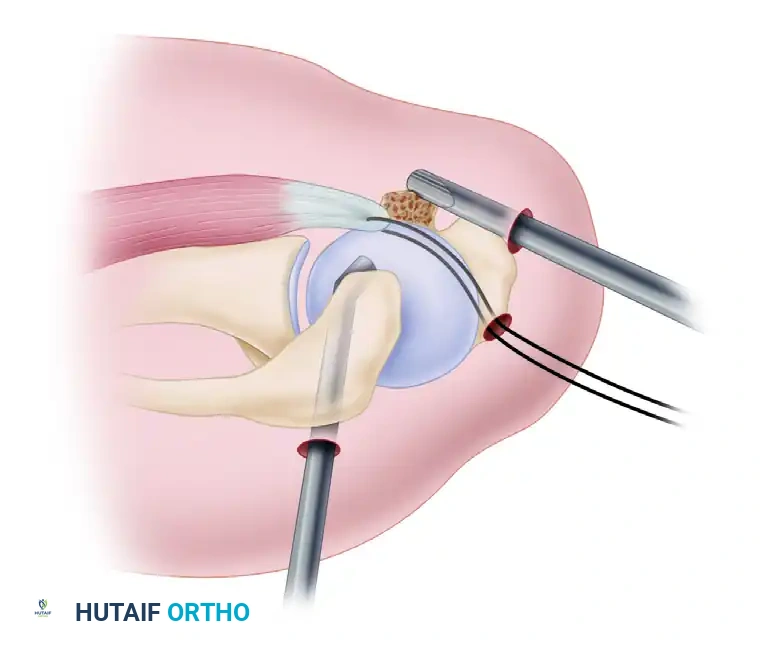
Figure 7: Preparation of the bone bed on the lesser tuberosity using a high-speed burr (superior view).
Anchor Placement and Fixation Techniques
The choice of fixation depends on the size of the tear and the degree of tendon excursion achieved after mobilization.
- Anchor Selection: For complete tears, two anchors are generally required to recreate the broad footprint of the subscapularis. For tears limited to the upper half of the tendon, a single anchor is sufficient. Standard screw-type anchors (e.g., Corkscrew; Arthrex, Naples, FL) are placed via the anterior portal.
- Standard Suture Passage: For tendons that easily reach the bone bed but cannot be over-pulled beyond it, standard suture passers (e.g., penetrators, bird-beaks) or shuttle relay techniques are utilized to pass sutures through the tendon.
- The "Traction Shuttle" Technique: For large, complete subscapularis tears that required extensive mobilization, passing sutures can be technically demanding. The "traction shuttle" technique is highly effective here:
- Pass the braided sutures from the seated anchor through the tendon by threading them through a loop created on the pre-existing traction suture.
- Pull the traction suture out through the tendon. As it exits, it "shuttles" the anchor's braided sutures through the tendon tissue with it.
- Retrieve the sutures and bring them out through the anterolateral portal, where arthroscopic knot tying is performed.
Clinical Pearl for Suture Management: After passing the suture through the tendon, retrieving the transtendon suture limb can sometimes be exceedingly difficult due to poor exposure caused by intraoperative deltoid swelling and fluid extravasation. To overcome this, thread the suture limb through the lumen of a single-hole knot pusher. Slide the knot pusher down the cannula to deliver the suture directly into the joint space, where it can be easily visualized and retrieved with a grasper.
Completion of the Procedure
Once the subscapularis repair is securely tied and probed for stability, the surgeon can proceed to address the remainder of the rotator cuff.
1. Perform a subacromial bursectomy and smoothing.
2. Crucial Step: Preserve the coracoacromial (CA) ligament. The CA ligament is a vital secondary stabilizer against anterosuperior escape, especially in the setting of massive rotator cuff tears.
3. Proceed with arthroscopic suture anchor repair of the supraspinatus and infraspinatus tendons as indicated.
Postoperative Care and Rehabilitation
The postoperative rehabilitation protocol must balance the need for tissue healing with the prevention of postoperative stiffness. Because the subscapularis is an internal rotator, external rotation places direct tension on the repair.
Phase I: Protection (Weeks 0-6)
* The patient is immobilized in a padded sling for 6 weeks.
* The shoulder is positioned in approximately 30 degrees of internal rotation to remove tension from the repaired tendon.
* Strict Restrictions: External rotation beyond neutral (0 degrees) is strictly prohibited. Active internal rotation is prohibited. Active or passive overhead elevation is restricted to protect the repair and any concomitant superior cuff repairs.
* Elbow, wrist, and hand range of motion exercises are encouraged immediately.
Phase II: Passive Range of Motion (Weeks 6-10)
* The sling is discontinued.
* Begin passive range of motion (PROM) focusing on forward elevation and gentle, progressive external rotation.
* External rotation is gradually increased, typically aiming for 30 degrees by week 8, depending on intraoperative tension assessments.
Phase III: Active Range of Motion and Early Strengthening (Weeks 10-14)
* Transition to active-assisted and active range of motion (AROM).
* Begin gentle isometric internal rotation exercises.
* Avoid aggressive stretching or sudden, forceful external rotation movements.
Phase IV: Advanced Strengthening (Weeks 14+)
* Progressive resistive exercises for the rotator cuff and periscapular stabilizers.
* Return to heavy labor or contact sports is generally delayed until 6 months postoperatively, contingent upon the restoration of strength and dynamic stability.
Conclusion
Arthroscopic subscapularis tendon repair is a technically demanding procedure that requires a profound understanding of anterior shoulder anatomy, precise portal placement, and advanced arthroscopic suturing skills. By systematically identifying the tear via the comma sign, adequately mobilizing the tendon while respecting the axillary nerve, and achieving secure footprint restoration, surgeons can provide patients with excellent functional outcomes and durable joint preservation. Adherence to a strict, phased postoperative rehabilitation protocol is equally critical to ensure the long-term success of the repair.
