INTRODUCTION TO PROXIMAL INTERPHALANGEAL JOINT HYPEREXTENSION DEFORMITIES
Hyperextension deformities of the proximal interphalangeal (PIP) joint, classically presenting as the swan-neck deformity, represent a complex biomechanical imbalance within the digital extensor and flexor mechanisms. Characterized by PIP joint hyperextension and reciprocal distal interphalangeal (DIP) joint flexion, this deformity severely compromises digital kinematics, precluding effective grasp and fine motor pinch.
While swan-neck deformities can arise from rheumatoid arthritis, trauma, or intrinsic contractures, they are particularly challenging in the context of spastic upper extremity conditions, such as cerebral palsy. In the spastic hand, hypertonia of the intrinsic muscles or the extrinsic extensors overpowers the stabilizing forces of the PIP joint volar plate and the flexor digitorum superficialis (FDS).
Surgical management aims to restore the delicate balance of forces across the PIP joint. Two highly effective, historically proven, and biomechanically sound procedures for addressing PIP hyperextension are the Sublimis Tenodesis (Curtis Technique) and the Lateral Band Translocation (Tonkin, Hughes, and Smith Technique). Both procedures aim to create a volar tether or dynamic checkrein to prevent PIP hyperextension while preserving active flexion.
BIOMECHANICAL CONSIDERATIONS OF THE PIP JOINT
To master these reconstructive techniques, the orthopedic surgeon must possess an intimate understanding of the PIP joint's functional anatomy. The PIP joint is a hinge joint stabilized by a robust capsuloligamentous complex and dynamically controlled by the intricate interplay of extrinsic and intrinsic tendons.
The Extensor Mechanism and Lateral Bands
The extensor mechanism at the level of the proximal phalanx trifurcates into a central slip (inserting on the base of the middle phalanx to extend the PIP joint) and two lateral bands. The lateral bands, formed by the convergence of the intrinsic tendons (lumbricals and interossei) and the lateral slips of the extrinsic extensor digitorum communis (EDC), glide dorsal to the PIP joint axis of rotation during extension.
In a swan-neck deformity, the lateral bands subluxate dorsally, increasing their extensor moment arm and locking the PIP joint in hyperextension. The transverse retinacular ligament of Landsmeer, which normally tethers the lateral bands volarly, becomes attenuated.
The Flexor Mechanism and Volar Plate
Volarly, the PIP joint is stabilized by the thick fibrocartilaginous volar (palmar) plate and the checkrein ligaments. The FDS tendon (historically referred to as the flexor digitorum sublimis) bifurcates at Camper's chiasm, wrapping around the flexor digitorum profundus (FDP) to insert on the volar-lateral aspects of the middle phalanx. The FDS serves as a primary flexor of the PIP joint and a dynamic stabilizer against hyperextension.
Clinical Pearl: In spastic cerebral palsy, the FDS may be weakened, over-lengthened, or overpowered by spastic intrinsics. Utilizing the FDS as a tenodesis (Curtis) or utilizing the lateral bands themselves as volar tethers (Tonkin) directly addresses the pathological dorsal migration of the extensor forces.
PREOPERATIVE EVALUATION AND PATIENT SELECTION
Thorough preoperative clinical and biomechanical assessment is mandatory. The surgeon must differentiate between a flexible, dynamic deformity and a fixed, rigid contracture.
- Passive Range of Motion (PROM): If the PIP joint cannot be passively flexed, a fixed contracture exists. Soft tissue releases (e.g., intrinsic release, lateral band mobilization) or joint manipulation must precede or accompany any tenodesis procedure.
- Intrinsic Tightness Testing (Bunnell Test): Evaluates whether the hyperextension is driven by intrinsic spasticity/contracture.
- FDS Function: The presence of an intact and functional FDS is a prerequisite for the Curtis sublimis tenodesis.
- Articular Integrity: Radiographs should confirm the absence of severe degenerative joint disease. Advanced arthrosis may necessitate PIP joint arthrodesis rather than soft-tissue reconstruction.
SURGICAL TECHNIQUE 1: SUBLIMIS TENODESIS OF THE PIP JOINT (CURTIS)
The Curtis technique is a classic, powerful procedure designed to create a robust volar checkrein using one of the two insertion slips of the FDS tendon. By detaching one slip proximally, routing it under the remaining flexor apparatus, and anchoring it to the contralateral side of the middle phalanx, the surgeon creates a static tether that physically blocks PIP hyperextension.
Indications
- Flexible swan-neck deformities.
- Recurrent PIP joint hyperextension secondary to volar plate laxity.
- Spastic conditions where a strong, static block to extension is required.
Patient Positioning and Preparation
- Position: Supine with the operative arm extended on a radiolucent hand table.
- Anesthesia: Regional block (axillary or supraclavicular) or general anesthesia.
- Tourniquet: An upper arm pneumatic tourniquet is applied and inflated to 250 mm Hg after exsanguination.
- Magnification: Surgical loupes (2.5x to 3.5x) are highly recommended for precise tendon handling.
Step-by-Step Surgical Approach
- Incision and Exposure:
- Utilize a volar Bruner (zigzag) incision over the affected digit, extending from the distal palmar crease to the distal interphalangeal (DIP) joint crease.
- Elevate the skin flaps, taking care to identify and protect the neurovascular bundles bilaterally.
- Flexor Sheath Window:
- Expose the flexor tendon sheath. Create a window in the cruciform pulleys (C1 or C2) between the A2 and A4 pulleys to visualize the FDS and FDP tendons. Preserve the A2 and A4 pulleys meticulously to prevent bowstringing.
- Isolation of the FDS Slip:
- Identify the bifurcation of the FDS tendon (Camper's chiasm).
- Select one slip of the FDS (typically the ulnar slip, depending on the surgeon's preference and the specific digital mechanics).
- Leave the distal insertion of this selected slip intact on the volar-lateral base of the middle phalanx.
- Sharply divide the selected slip proximally at the level of the bifurcation.
- Rerouting the Tendon:
- Pass the freed proximal end of the FDS slip transversely under the remaining intact FDS slip and the FDP tendon to the opposite (contralateral) side of the PIP joint.
- Osseous Fixation:
- Prepare a small bony trough or drill hole on the lateral aspect of the middle phalanx on the side opposite the slip's original insertion.
- Secure the tendon into the bone using a pull-out wire suture technique (e.g., a Bunnell or Krackow stitch with a Keith needle passed dorsally through the bone and skin, tied over a sterile button). Alternatively, modern small-joint bone anchors (e.g., 1.3mm or 1.5mm suture anchors) can be utilized to avoid external hardware.
- Joint Pinning:
- Reduce the PIP joint to 20 to 30 degrees of flexion.
- Drive a 0.045-inch (1.14 mm) Kirschner wire (K-wire) obliquely across the PIP joint to hold it rigidly in this flexed position. This removes all tension from the tenodesis during the critical early healing phase.
Surgical Warning: Ensure the K-wire engages both cortices of the proximal and middle phalanges to prevent premature loosening. The tension on the tenodesis should be taut at 20 degrees of flexion; if it is loose, the checkrein effect will fail.
Postoperative Protocol (Curtis Technique)
- The hand is placed in a bulky soft dressing and a volar plaster splint.
- The traversing K-wire is left in place for 6 weeks to allow solid biological integration of the tenodesis.
- At 6 weeks, the K-wire and the pull-out wire (if used) are removed in the clinic.
- Active and active-assisted flexion exercises are initiated immediately. Extension is blocked at 20 degrees of flexion with a dorsal figure-of-eight splint for an additional 2 to 4 weeks to prevent stretching of the repair.
SURGICAL TECHNIQUE 2: LATERAL BAND TRANSLOCATION (TONKIN, HUGHES, AND SMITH)
The lateral band translocation technique is a highly elegant, dynamic reconstruction. Rather than creating a static tether from the flexor tendons, this procedure addresses the primary pathology—the dorsal subluxation of the lateral bands. By mobilizing a lateral band and translocating it volar to the PIP joint's axis of rotation, the lateral band is converted from a deforming extensor force into a dynamic PIP joint flexor, while still maintaining its ability to extend the DIP joint.
Indications
- Spastic swan-neck deformities (highly favored in cerebral palsy).
- Flexible deformities where preservation of FDS function is paramount.
- Cases requiring simultaneous correction of DIP extension lag.
Step-by-Step Surgical Approach
- Incision and Exposure:
- Make a midlateral incision on the radial side of the finger, extending from the mid-proximal phalanx to the mid-middle phalanx.
- Elevate the dorsal flap to expose the extensor mechanism and the volar flap to expose the flexor tendon sheath.
- Mobilization of the Lateral Band:
- Identify the radial lateral band.
- Mobilize it from the midpoint of the proximal phalanx to the midpoint of the middle phalanx.
- Dorsal Release: Separate the lateral band from the central tendon mechanism dorsally.
- Volar Release: Divide the transverse retinacular ligament of Landsmeer on the palmar aspect of the lateral band. The lateral band should now be completely free-floating in the mid-substance.
- Preparation of the Retaining Sling:
- Identify the accessory collateral ligament and divide it at its insertion into the palmar (volar) plate. This exposes the free lateral margin of the palmar plate.
- Crucial Anatomy: Ensure the insertion of the palmar plate into the base of the middle phalanx and its origin from the proximal phalanx remain completely intact.
- (Optional) Perform a synovectomy of the PIP joint at this stage if inflammatory synovitis is present.
- Flexor Sheath Exposure:
- Open the flexor tendon sheath between the A2 and A4 pulleys.
- Identify the radial slip of the FDS insertion.
- Translocation and Sling Creation:
- Translocate the mobilized lateral band palmarward (volarly) so that it sits below (volar to) the anatomical axis of rotation of the PIP joint.
- Create a retaining sling to hold the lateral band in this new volar position. Use two 4-0 non-absorbable sutures (e.g., braided polyester or nylon) placed at the distal edge of the PIP joint.
- Pass these sutures between the free margin of the palmar plate and the radial slip of the FDS tendon.
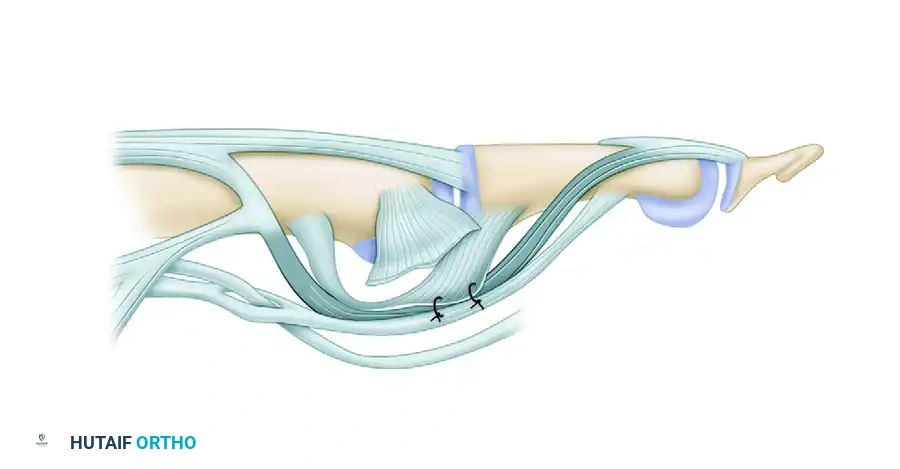
Figure: Tonkin et al. lateral band translocation technique. Separation of the lateral band from the midpoint of the proximal phalanx to the midpoint of the middle phalanx. Release of accessory collateral ligament. Suture of palmar plate to flexor digitorum superficialis tendon to create retaining sling.
- Tensioning the Translocated Tendon:
- Pass the lateral band through the newly created sling.
- The Tension Test: Support the finger solely by the digital pulp. The tension of the translocated tendon must be adjusted so that the PIP joint does not extend beyond 5 degrees of flexion.
- Adjusting Tension:
- To loosen tension: Dissect the lateral band further proximally from the central tendon mechanism.
- To tighten tension: Resuture the lateral band to the central slip under greater tension.
- Preventing Propagation: To prevent the translocated tendon from splitting further away from the central tendon over time, place a single locking suture at the exact point of proximal and distal separation.
- Addressing the DIP Joint:
- Evaluate the DIP joint. If an extension lag remains (due to the altered mechanics of the lateral band), place a temporary 0.035-inch K-wire across the DIP joint to maintain it in full extension for 4 weeks.
- In severe, rigid cases, a primary DIP joint arthrodesis may be considered.
- Closure:
- Obtain meticulous hemostasis. Deflate the tourniquet prior to closure to ensure no digital ischemia.
- Suture the skin with 5-0 or 6-0 nylon.
Clinical Pearl: The success of the Tonkin procedure relies entirely on precise tensioning. If the lateral band is too loose, the swan-neck deformity will recur. If it is too tight, the patient will develop a fixed PIP flexion contracture (boutonnière-type deformity). The "pulp support test" intraoperatively is the most reliable indicator of correct tension.
Postoperative Protocol (Tonkin Technique)
Unlike the Curtis technique, the Tonkin procedure allows for earlier mobilization, relying on the dynamic sling rather than rigid osseous fixation.
* 0 to 48 Hours: The hand is immobilized in a bulky, compressive palmar resting splint with the metacarpophalangeal (MCP) joints flexed to 70 degrees and the interphalangeal joints in the resting flexed position obtained intraoperatively.
* 48 Hours: The initial bulky dressings are reduced.
* Early Mobilization: Gentle, active mobilization is initiated under the guidance of a specialized hand therapist.
* Splinting: A dorsal block splint must be worn continuously to protect the PIP joint from hyperextension for 2 to 4 weeks. The splint should block extension at approximately 10 to 15 degrees of flexion but allow full active flexion.
* DIP Management: If a DIP K-wire was placed, it is removed at 4 weeks in the clinic.
COMPLICATIONS AND PITFALLS
Both the Curtis and Tonkin procedures are technically demanding and carry specific risks:
- Recurrence of Deformity: The most common complication. In the Curtis procedure, this occurs if the pull-out wire fails or the tendon pulls through the bone before biological healing (usually due to premature K-wire removal). In the Tonkin procedure, recurrence is due to inadequate tensioning or failure of the palmar plate-FDS sling.
- PIP Joint Stiffness / Flexion Contracture: Over-tensioning either the FDS slip or the lateral band will result in a fixed flexion contracture. While a slight flexion contracture (5-10 degrees) is often functionally acceptable and preferable to hyperextension, severe contractures impair grasp.
- Hardware Complications: Pin tract infections from the traversing K-wires can occur. Meticulous pin care and oral antibiotics for superficial erythema are required. If deep infection occurs, the pin must be removed immediately.
- Swan-Neck to Boutonnière Conversion: Aggressive volar translocation and over-tightening of the lateral band can completely disrupt the extensor mechanism's balance, leading to a secondary boutonnière deformity.
CONCLUSION
The management of PIP joint hyperextension requires a nuanced understanding of digital biomechanics. The Curtis sublimis tenodesis provides a robust, static volar block ideal for severe laxity, while the Tonkin lateral band translocation offers a dynamic, anatomically elegant solution that directly reverses the pathological dorsal migration of the extensor forces. Careful patient selection, meticulous surgical execution—particularly regarding tendon tensioning—and strict adherence to postoperative rehabilitation protocols are paramount to achieving optimal functional outcomes in these complex reconstructive cases.
