Score: 0%
Orthopedics Online MCQs
Sport Orthopedics Mcqs online Bank
A 32-year-old man has groin pain that is aggravated by sitting. A frog leg lateral and an axial MR arthrogram with gadolinium are shown in Figures 26a and 26b. Nonsurgical management has failed to provide relief and it has been decided to proceed with surgical intervention. The most appropriate surgical approach should include ](http://www.orthobullets.com/knee-and-sports/3130/femoroacetabular-impingement)Review Topic
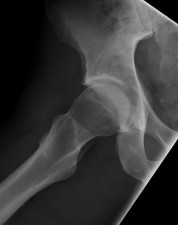





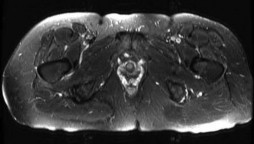









A 32-year-old man has groin pain that is aggravated by sitting. A frog leg lateral and an axial MR arthrogram with gadolinium are shown in Figures 26a and 26b. Nonsurgical management has failed to provide relief and it has been decided to proceed with surgical intervention. The most appropriate surgical approach should include ](http://www.orthobullets.com/knee-and-sports/3130/femoroacetabular-impingement)Review Topic

Keywords