BIOMECHANICS AND PEDIATRIC SPINAL ANATOMY
The pediatric spine is a highly dynamic structure, biomechanically and anatomically distinct from the adult spine. Fractures and dislocations in children are relatively rare but carry the potential for catastrophic neurological morbidity. They are most frequently observed in newborns as a consequence of non-accidental trauma (child abuse), in young children with underlying syndromic ligamentous laxity (e.g., Down syndrome, Marfan syndrome), and in older children following high-energy trauma such as motor vehicle collisions or diving accidents.
The inherent flexibility of the pediatric cervical spine is attributed to several anatomical factors:
* Ligamentous Laxity: The supporting ligaments and joint capsules are highly elastic, allowing significant physiological translation.
* Facet Orientation: The articular facets in young children are oriented more horizontally, providing less osseous restraint against anterior translation.
* Incomplete Ossification: The vertebral bodies are wedge-shaped anteriorly, and the uncinate processes are underdeveloped, reducing structural stability.
* Fulcrum of Motion: Due to the disproportionately large head-to-body ratio in infants and toddlers, the fulcrum of cervical flexion is located higher (C2-C3) compared to adults (C5-C6).
Clinical Pearl: Because the pediatric spine can stretch up to 2 inches without structural failure, whereas the spinal cord can only stretch 0.25 inches, children are highly susceptible to Spinal Cord Injury Without Radiographic Abnormality (SCIWORA). Always maintain a high index of suspicion for cord injury even in the presence of normal plain radiographs.
PREHOSPITAL IMMOBILIZATION AND POSITIONING
Proper alignment during transport is critical to prevent iatrogenic neurological injury. Herzenberg et al. demonstrated that the standard adult backboard forces the young child's cervical spine into dangerous relative kyphosis due to their prominent occiput.
In children younger than 7 years, unstable cervical spine injuries typically exhibit anterior angulation or translation. Extension is the proper position for reduction in the vast majority of these cases. To achieve neutral alignment or slight extension, transport protocols must utilize a modified backboard featuring an occipital recess to lower the head, or a double mattress pad placed beneath the torso to elevate the chest.
RADIOGRAPHIC EVALUATION AND DEVELOPMENTAL VARIANTS
Differentiating normal physiological hypermobility from acute traumatic instability is the most challenging aspect of pediatric spine evaluation. Flexion and extension radiographs must be interpreted with a profound understanding of developmental anatomy.
The Atlanto-Dens Interval (ADI)
In adults, an anterior displacement of the atlas greater than 3 mm is abnormal. However, Cattell and Filtzer established that an ADI of up to 3 to 5 mm in flexion is a normal physiological variant in asymptomatic children aged 1 to 7 years.
* ADI 3–5 mm: Normal variant in children (due to ligamentous laxity).
* ADI > 5 mm: Indicates rupture of the transverse ligament.
* ADI > 10–12 mm: Indicates catastrophic failure of all stabilizing ligaments (transverse, alar, and apical).
Pseudosubluxation
Pseudosubluxation of C2 on C3 (and to a lesser extent C3 on C4) is a frequent normal variant, particularly in children under 7. It is characterized by apparent anterior displacement of C2 on C3 during flexion. Swischuk's line (drawn from the anterior aspect of the posterior arch of C1 to C3) is invaluable here; if the anterior aspect of the posterior arch of C2 misses this line by more than 2 mm, true structural dislocation should be suspected.
Fielding’s Radiographic Mimics
Fielding outlined 13 normal radiographic variations that are frequently misinterpreted as acute injuries:
1. Apical Ossification Center: The apical ossification center of the odontoid (terminal ossicle) appears between ages 3 and 6 and fuses by age 12. It can easily be confused with an acute type I odontoid fracture.
2. Secondary Ossification Centers: Located at the tips of transverse and spinous processes, mimicking avulsion fractures.
3. Incomplete Ossification: Especially of the odontoid process, creating the illusion of superior subluxation of the anterior arch of C1.
4. Persistent Synchondrosis: The physis at the base of the odontoid may persist radiographically long after physiological closure.
5. Anterior Wedging: Normal physiological wedging of the immature vertebral body mimicking a compression fracture.
6. Hypermobility (Pseudosubluxation): C2 anterior to C3.
7. Increased ADI: Up to 4–5 mm is acceptable in young children.
8. Absent Anterior Arch Ossification: In the first year of life, lack of ossification suggests false posterior displacement of C1.
9. Prevertebral Soft-Tissue Swelling: Physiological variations in width, exacerbated by the phase of respiration (always evaluate on inspiration).
10. Overlying Anatomy: Earlobes, braided hair, teeth, or the hyoid bone projecting over the spine.
11. Horizontal Facets: Creating the illusion of a pillar fracture.
12. Congenital Anomalies: Os odontoideum, spina bifida occulta, or block vertebrae (Klippel-Feil syndrome).
13. Absent Cervical Lordosis: A straight spine is common in children due to muscle spasm or positioning and does not inherently indicate trauma.
Advanced imaging, including thin-slice Computed Tomography (CT) and Magnetic Resonance Imaging (MRI), is essential when plain radiographs are equivocal, particularly to assess the integrity of the transverse ligament and the spinal cord.
CERVICAL SPINE INJURIES
Atlantoaxial Instability and Rotary Subluxation
Lesions from the occiput to C1 are extremely rare and usually fatal due to cervicomedullary junction transection. However, injuries from C1 to C4 are the most prevalent cervical injuries in the pediatric population.
Fielding classified C1-C2 interval lesions into four categories:
1. Ligamentous Laxity (Inflammatory): Often termed Grisel's syndrome, this is a non-traumatic atlantoaxial subluxation secondary to inflammation (e.g., upper respiratory infection, retropharyngeal abscess, juvenile rheumatoid arthritis).
2. Rotary Deformity: The most common cause of traumatic torticollis.
3. Traumatic Ligamentous Disruption: True structural failure.
4. Odontoid Fracture.
Management of Rotary Subluxation:
Most rotary deformities are benign and resolve with conservative management: head-halter traction, muscle relaxants, and bed rest. However, Fielding established strict criteria for surgical intervention (C1-C2 posterior fusion) in refractory cases:
* Persistent neurological deficit.
* Significant anterior rotary displacement with transverse ligament compromise.
* Failure to achieve or maintain reduction after 3 months.
* Recurrence of deformity after 6 weeks of rigid immobilization.
Odontoid Fractures in the Immature Spine
The anatomy of the pediatric axis is defined by its ossification centers. The synchondrosis at the base of the odontoid separates the dens from the body of C2. While it typically closes by age 7, a visible epiphyseal scar can persist into adolescence.
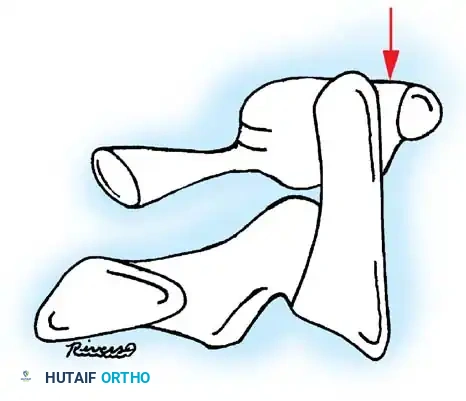
Fig. 1: Relationships of the atlas and axis in the pediatric spine. Note the apical epiphysis, the physiological space between the odontoid and anterior arch of the atlas (which may exceed 3 mm), and the basilar odontoid synchondrosis.
Because the synchondrosis is the biomechanically weakest point, almost all pediatric odontoid fractures occur at this level (a Salter-Harris I equivalent injury), rather than through the dense cortical bone of the odontoid waist seen in adults.
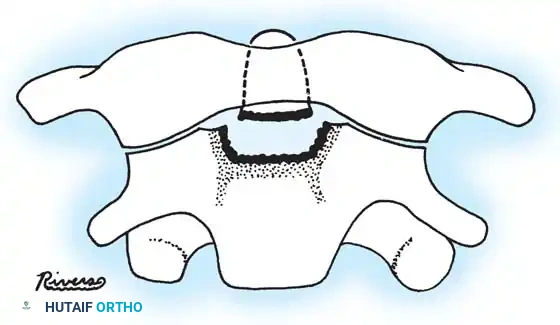
Fig. 2: Pattern of odontoid fractures. 'm' denotes the typical level of adult Type II fractures at the waist; 'l' denotes the area of childhood fractures occurring through the basilar synchondrosis.
Treatment Protocol for Pediatric Odontoid Fractures:
Unlike adult Type II fractures, which have a high nonunion rate, pediatric synchondrotic fractures possess massive osteogenic potential and heal reliably with conservative care.
1. Reduction: Achieved via passive manipulation or recumbency on a divided mattress with head-halter traction in extension.
2. Immobilization: Once reduced, apply a Minerva cast, halo vest, or rigid cervical orthosis for 8 to 12 weeks.
3. Surgical Indications: Surgery is rarely indicated unless the fracture is irreducible via closed means, or if there is an underlying congenital anomaly (e.g., os odontoideum) causing chronic instability.
Surgical Warning: Skeletal traction must be applied with extreme caution in children. The immature spine is highly susceptible to over-distraction, which can precipitate catastrophic ischemic injury to the spinal cord.
Subaxial Cervical Spine (C3-C7) Fractures
Fractures below C2 are exceedingly rare in young children. When they occur, they are often misdiagnosed due to the physiological anterior wedging of the vertebral bodies. True fractures or fracture-dislocations require stabilization.
Surgical Arthrodesis Principles in Children:
When fusion is indicated, the surgeon must respect the robust osteogenic response of the pediatric periosteum. Fusion masses develop rapidly and profusely.
* Limit Exposure: Only expose the specific levels intended for fusion. Subperiosteal dissection of adjacent normal segments will inevitably lead to "creeping fusion" (unintended arthrodesis of adjacent levels), resulting in severe restriction of neck mobility.
* Avoid Laminectomy: Laminectomy removes the posterior tension band, almost guaranteeing progressive post-laminectomy kyphosis in a growing child.
THORACOLUMBAR SPINE FRACTURES
Thoracic and lumbar fractures are less common than cervical injuries but incidence increases with age, peaking in adolescence due to sports, recreational activities, and motor vehicle trauma.
Pathological Mimics
Before diagnosing an acute traumatic compression fracture, the surgeon must rule out pathological entities that cause vertebral collapse (vertebra plana) or wedging:
* Eosinophilic Granuloma (Langerhans cell histiocytosis)
* Scheuermann Disease (microfractures in adolescent athletes/gymnasts)
* Gaucher Disease
* Osteogenesis Imperfecta
* Idiopathic Juvenile Osteoporosis
* Metastatic Disease (e.g., neuroblastoma, leukemia)
Slipped Vertebral Apophysis (Apophyseal Ring Fracture)
A unique pediatric injury is the displacement of the lumbar vertebral ring epiphysis. This occurs in adolescents when a fragment of the bony apophyseal ring avulses and displaces posteriorly into the spinal canal, often taking the annulus fibrosus and disc material with it.
* Clinical Presentation: Indistinguishable from an acute herniated nucleus pulposus (sciatica, positive straight leg raise).
* Diagnosis: MRI is the gold standard, though a fine-cut CT scan best delineates the osseous fragment.
* Treatment: Surgical excision of the bony fragment and associated disc material via a limited laminotomy/microdiscectomy approach.
Spinal Cord Injury and Paraplegia
Thoracolumbar trauma carries a high risk of complete spinal cord lesions. The management of pediatric paraplegia requires a multidisciplinary approach due to the severe developmental sequelae:
1. Progressive Spinal Deformity: Paralytic scoliosis, kyphosis, and lordosis are nearly universal if the injury occurs before the adolescent growth spurt.
2. Paralytic Hip Dislocations: Due to muscle imbalance and lack of weight-bearing.
3. Long Bone Fractures: Secondary to profound disuse osteopenia.
4. Soft Tissue Complications: Decubitus ulcers and severe flexion contractures.
5. Genitourinary Dysfunction.
SURGICAL APPROACHES AND TECHNIQUES
When conservative management fails or the spine is grossly unstable, surgical stabilization is required.
Step-by-Step: Pediatric C1-C2 Posterior Arthrodesis
For irreducible rotary subluxation or unstable os odontoideum, a C1-C2 fusion is indicated.
1. Positioning: Prone, using a pediatric Mayfield skull clamp or halo ring. Ensure the neck is in a neutral or slightly extended position. Neuromonitoring (SSEP/MEP) is mandatory.
2. Exposure: Midline incision from the inion to C3. Meticulous subperiosteal dissection is limited strictly to the posterior arch of C1 and the lamina/spinous process of C2.
3. Instrumentation (Harms Technique):
* C1 Lateral Mass Screws: The C2 nerve root is mobilized inferiorly. The entry point is at the junction of the C1 posterior arch and the lateral mass. Use pediatric-sized polyaxial screws (typically 3.5 mm diameter).
* C2 Pars/Pedicle Screws: Entry point is in the superior-medial quadrant of the C2 isthmus. Trajectory is 20 degrees up and 20 degrees medial.
4. Reduction & Fixation: Rods are contoured and secured, reducing the C1-C2 articulation.
5. Bone Grafting: The posterior arch of C1 and lamina of C2 are decorticated. Autologous iliac crest bone graft (structural and cancellous) is packed into the interlaminar space.
6. Closure: Layered closure over a subfascial drain. Postoperatively, a rigid cervical collar is maintained for 6-12 weeks until radiographic fusion is confirmed.
Thoracolumbar Pedicle Screw Fixation
Operative indications for pediatric thoracolumbar fractures mirror adult criteria (e.g., >50% loss of vertebral body height, >30 degrees of kyphosis, neurological deficit).
* Technique: Pedicle screw fixation is safe in children, provided preoperative CT is used to measure pedicle diameter. In children under 10, the pedicles may be too narrow for standard screws, necessitating the use of hooks (laminar, pedicle, or transverse process) or specialized pediatric instrumentation systems.
* Fusion: Perform a meticulous posterolateral decortication and arthrodesis using autograft. Avoid extending the fusion across the thoracolumbar junction if possible to preserve motion.
POSTOPERATIVE PROTOCOLS AND LONG-TERM SURVEILLANCE
The postoperative management of pediatric spine fractures extends far beyond the acute healing phase.
* Immobilization: Halo vests or custom-molded Thoracolumbosacral Orthoses (TLSO) are typically worn for 8 to 12 weeks.
* Radiographic Surveillance: Serial standing radiographs are required every 6 months until skeletal maturity. The "crankshaft phenomenon" (continued anterior vertebral growth in the presence of a solid posterior fusion) can lead to progressive rotational and angular deformities, occasionally necessitating secondary anterior release and fusion.
* Rehabilitation: Early mobilization, aggressive physical therapy, and integration into specialized pediatric spinal cord injury programs are essential for maximizing functional recovery and mitigating the psychosocial impact of the injury.
