DEFINITION
A fingertip injury or amputation involves trauma to the finger distal to the distal interphalangeal (DIP) crease. The fingertip is the most sensitive area of the hand. Fingertip injuries are common, accounting for 45% of emergency room hand injuries.
ANATOMY
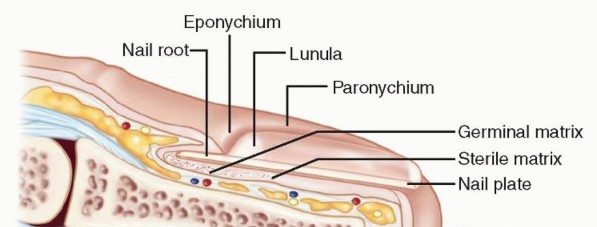
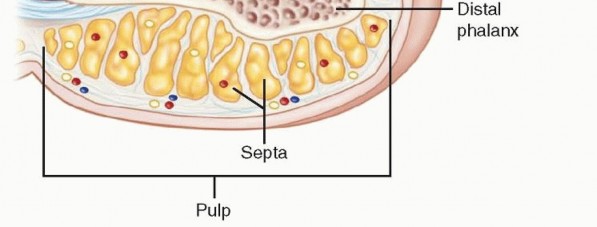
FIG 1 • Cross-section of a fingertip depicting key anatomic structures.
FINGERTIP AMPUTATION CLASSIFICATION (TAMAI)
Zone I: distal to lunula Zone II: DIP joint to lunula
PATHOGENESIS
Various mechanisms of traumaAvulsion Crush Compression SharpDull
NATURAL HISTORY
Fingertip injuries with no bone exposed will ultimately heal by secondary intention.In the setting of wounds less than 1 cm2, secondary intention healing aided by daily dressing changes actually allows for increased recovery of sensation.The use of secondary intention healing for larger injuries involves a prolonged period of dressing changes with associated risk of infection and unfavorable scarring.
PATIENT HISTORY AND PHYSICAL FINDINGS
Full history and physical examinationMechanism of injury AgeHandedness OccupationLevel of cooperation and understanding Injury assessmentDigit or digits involved: thumb versus fingerTransverse versus dorsal oblique-volar oblique versus radial-ulnar Damage to nail or nail bedExposure of boneStatic and moving two-point discrimination: There is decreased density of innervation with increased two-point discrimination.Terminal flexion and extension: Injury to tendons will require more significant flap coverage. Vascularity: Prolonged capillary refill is suggestive of arterial injury.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Plain radiographs in orthogonal planes (posteroanterior, lateral)
NONOPERATIVE MANAGEMENT
P.1251Most fingertip amputations may be treated at the bedside using sterile technique and employing a metacarpal block, finger tourniquet, and loupe magnification.There should be a low threshold for operative management.If no bone is exposed, options include healing by secondary intention, primary closure, or skin grafting. Secondary intention healing aided by daily dressing changes provides the best recovery of sensation and is appropriate for wounds less than 1 cm2.Primary closure is an option only if there is minimal skin loss.Tight closures should be avoided. This can minimize function by causing joint contracture and distal tip tenderness due to poor soft tissue coverage of the bony prominences.Sewing the volar skin tightly to the distal nail may result in a cosmetically displeasing hook nail.If a nail bed laceration is suspected, the nail plate should be removed with a Freer elevator, allowing repair of the nail bed with either 6-0 or 7-0 simple interrupted absorbable sutures (chromic gut). Loupe magnification is extremely helpful.The eponychial fold should be stented open with either trimmed and carefully cleansed nail or other material (eg, foil from a suture pack) to prevent abnormal growth of the future nail.With amputations through the germinal matrix, any remaining unrepairable matrix should be removed to prevent formation of a painful nail remnant.
SURGICAL MANAGEMENT
The decision to take a patient with a fingertip injury to the operating room depends on the size of the defect, presence of exposed bone, angle of amputation, willingness of the patient to do dressing changes, and surgeon experience.The goals are to preserve function and sensation and allow early return to activity.In terms of functional outcome, healing by secondary intention provides equal or better results for defects less than 1 cm in diameter.Full-thickness grafts are preferable to split-thickness grafts.Split-thickness grafts should be used only on the ulnar side of the index, middle, and ring fingers.Donor site options include the volar wrist skin (should be avoided, as it can mimic a suicide attempt laceration), antecubital skin, medial upper arm skin, and hypothenar skin.These donor sites can be closed primarily.If salvageable, the original skin from the amputated segment can be defatted and applied as a graft/biologic dressing.If bone is exposed, options include bone shortening and primary closure and bone shortening and healing by secondary intention or fingertip flaps.
PREOPERATIVE PLANNING
Preliminary irrigation and débridement, exploration AntibioticsPatient comorbiditiesIs the patient a diabetic? smoker? recreational drug user? Is the tetanus status up-to-date?Anesthesia assessment
POSITIONING
Supine with standard hand table. An arm, forearm, or digital tourniquet is used. The arm is placed in the center of the hand table for equal access by the surgeon and assistant.
APPROACH
Once the decision to perform a flap has been made, the angle of amputation, patient age, and patient gender determines whether an advancement or regional flap is appropriate.
TECHNIQUE
SKIN GRAFTING

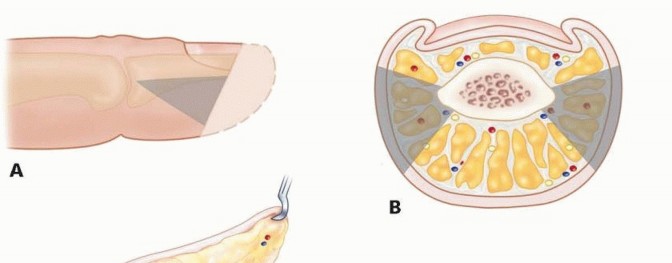
TECH FIG 1 • A. Ulnar defect of the long finger with the proposed hypothenar graft drawn out.(continued)
TECH FIG 1 •(continued)B. The hypothenar full-thickness skin graft is harvested, taking great care to




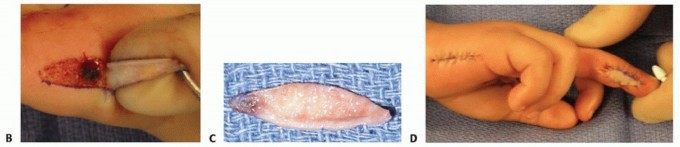
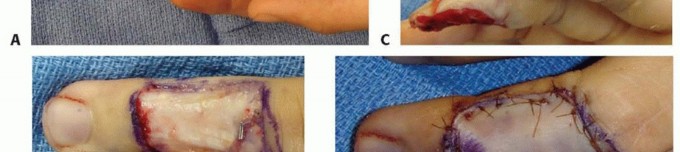
TECH FIG 2 • A. Distal thumb defect with exposed proximal phalanx. B. Nonreplantable distal phalanx. C. Intraoperative photograph indicating planned Moberg flap, with longitudinal incisions just dorsal to neurovascular bundles and based at metacarpophalangeal joint flexion crease. D. Moberg flap elevation from flexor sheath. E. Advancement of Moberg flap was possible without creation of an island flap or use of a triangle of Burow. F. Closure of the defect after advancement of Moberg flap. (Courtesy of James Chang, MD.)
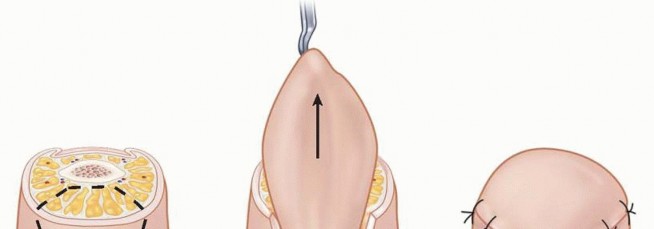
TECH FIG 3 • A. Lateral view of the digit with triangular flaps raised along the midlateral line. B. Flaps raised on both the radial and ulnar neurovascular bundles. C. Adventitia is released and the flaps are advanced distally to cover the defect. D. The flaps are sewn together to cover the defect, and the donor area is closed primarily in a lateral V-Y fashion.
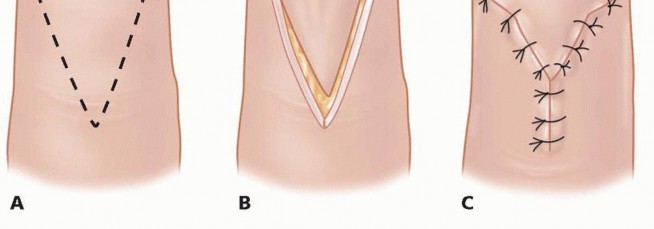
TECH FIG 4 • A. Volar-based V is incised. B. The volar flap is advanced distally to cover the distal defect. C. The flap is secured distally, and the donor area is closed primarily in a volar V-Y fashion.
CROSS-FINGER FLAP




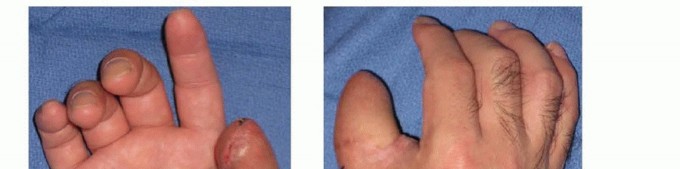
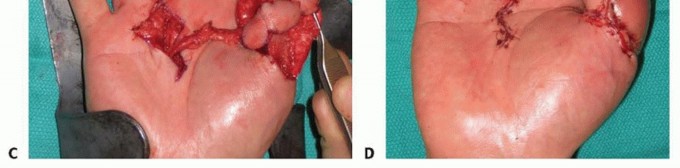
TECH FIG 5 • A. Intraoperative photograph depicting ring finger volar fingertip avulsion with exposed flexor tendon and small finger amputation at middle phalanx level. B,C. Two weeks after successful replantation of small finger with continued problem of ring finger wound, which had been treated with daily dressing changes. D. Intraoperative photograph after elevation of cross-finger flap from dorsal aspect of middle phalanx skin of adjacent finger. E. Intraoperative photograph after cross-finger flap from middle finger for coverage of volar ring finger defect. Donor site was covered with a full-thickness skin graft. Blue background indicates preservation of sensory branch.(continued)
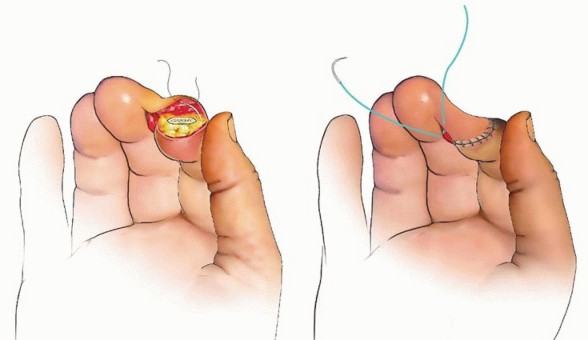
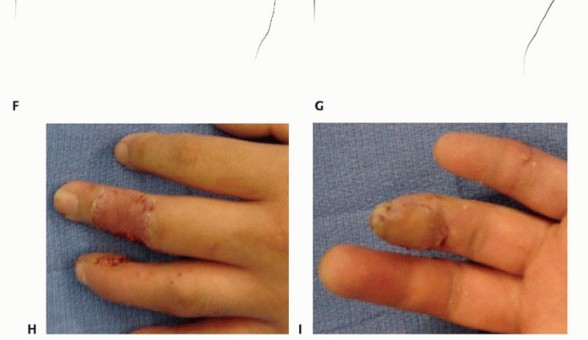
TECH FIG 5 •(continued)F,G. Illustration of the operative method. H,I. Intraoperative photographs after cross-finger flap division at 3 weeks.
REVERSE CROSS-FINGER FLAP


TECH FIG 6 • A. Dorsal defect of the right index finger with the flap drawn out on the adjacent long finger.




TECH FIG 6 •(continued)B. Ulnarly based skin flap raised from the long finger. C,D. The subcutaneous tissue is elevated off the paratenon of the long finger. E. The flap is inset onto the index finger defect. F. Split-thickness skin graft placed on the recipient site. The native ulnarly based skin flap is restored onto the long finger. G. Three months postoperatively. (Courtesy of Phani Dantuluri, MD.)
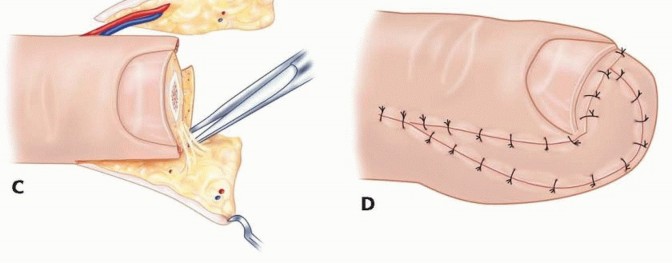
THENAR FLAP




TECH FIG 7 •(continued)C. Dissection of the flap is performed at the level of the thenar musculature. Note the digital nerve present in the field of dissection. D. The flap is sewn in position. (Courtesy of Thomas R. Hunt III, MD.)
NEUROVASCULAR ISLAND PEDICLE FLAP (LITTLER)



TECH FIG 8 • A,B. Insensate volar distal thumb after coverage of amputation site with free flap. C. Intraoperative photograph depicting neurovascular island pedicle flap (Littler) harvested from ulnar aspect of middle finger. D. Intraoperative photograph after tunneling of neurovascular island pedicle flap (Littler) to volar distal thumb, closure of wounds, full-thickness skin grafting of donor site, and application of a bolster dressing. (Courtesy of James Chang, MD.)


TECH FIG 9 • A. Positioning the amputated part between the surgeon's ring fingers of both hands. B. Palmar vein repair.Four to five 10-0 nylon sutures are used to repair the large central artery.To aid the visualization and placement of the sutures, heparinized saline is used to irrigate the vessel lumen.In zone I, following arterial repair, the clamps are released momentarily to locate the subdermal palmar vein.Close the skin from dorsal to palmar, and then anastomose the subcutaneous palmar vein.Palmar vein anastomosis is carried out using a 1-V double clamp. If the clamp cannot be applied, the two ends are brought together and the corner sutures are held while the others are put in (TECH FIG 9B).A 11-0 suture with 50 μm needle is used.Repair the nerve ends with 10-0 nylon suture.Artery and vein clamps are removed after the repair, and skin flaps are approximated to cover the anastomosis.The limb is kept immobilized in a short-arm cast for 2 weeks. The finger is watched for color change. Bluish coloring with hyperbrisk capillary refill indicates a venous congestion problem and a pale color with poor capillary refill and turgor indicates an arterial inflow problem. Continuous pulse oximetry may be used to monitor the oxygenation of the digit as well.The patient is kept on intravenous (IV) antibiotics and continuous infusion of 500 mL Dextran 40 and 5000 units of Heparin for 5 days, followed by 75 mg of aspirin for 3 weeks.P.1259
PEARLS AND PITFALLS
Fingertip injuries less than 1 cm2 can generally be treated with dressing changes with equal or better results than flap closure.The bridging vessels should be carefully preserved when performing a Moberg flap to prevent skin necrosis.V-Y advancement flaps may lead to scarring and hypersensitivity at the fingertip.The radial digital nerve should be carefully preserved and protected when performing a thenar flap. Cross-finger flaps (nonglabrous skin) may lead to hair growth on the fingertip and deficiency of pulp.Thenar flaps (glabrous skin) allow good sensibility in the flap but may be complicated by development of PIP joint contractures, especially in older male patients.Poor sensory outcome in neurovascular island flaps can be minimized by use of the most distal portion of donor skin, preservation of as much subcutaneous skin on the pedicle as possible, and avoidance of tension and kinking in the pedicle.
POSTOPERATIVE CARE
When possible, the patient should meet the hand therapist preoperatively. Active and passive range of motionSensory reeducation Scar massageMoberg advancement flap: thumb spica splint for 10 days to 2 weeks, followed by range-of-motion exercisesLateral V-Y advancement and volar V-Y advancement flaps: finger splintage of only the involved joint for 10 days to 2 weeks, followed by range-of-motion exercisesCross-finger flap and reverse cross-finger flap: A nonadherent bolster dressing is applied to the skin graft site and a splint is applied. PIP joints and the DIP joint of the donor finger can be gently ranged 2 weeks after flap inset, taking care to avoid tension on the flap. After flap division at 3 weeks, range-of-motion exercises are directed toward extending the PIP joints. Severe contractures may be treated with static progressive splinting.Thenar flap: A splint is applied postoperatively. Gentle range of motion of unaffected digits is started 2 weeks after flap inset, with care taken to avoid tension on the flap. Full range-of-motion exercises are started after flap division at 3 weeks. Severe contractures may be treated with static progressive splinting.Neurovascular island flap: The splint is changed 10 days after surgery, when sutures can be removed; gentle active range of motion is started, with full range of motion delayed until 3 weeks after surgery. Sensory reeducation is necessary to help differentiate thumb from middle finger sensation.Distal fingertip replantation: The Kirschner wire is removed in 4 weeks and a finger splint is kept on for an additional 2 weeks for lifting and during sleep. Otherwise, therapy for range-of-motion exercises is begun.
OUTCOMES
Moberg flaps consistently provide return of normal two-point discrimination or within 2 mm of the contralateral digit and may result in a decrease in the hyperextensibility of the interphalangeal joint with no functional impairment.V-Y advancement flaps result in return of sensation to within 2.75 mm of the contralateral digit but may also result in paresthesia, hypersensitivity, and cold intolerance (50%).Patients who undergo a cross-finger flap have a return of protective sensation (8 mm of two-point discrimination), most predictably in younger patients, but the sensation remains less than the normal pulp.Hematoma or seroma significantly impairs the return of sensation.Thenar flaps provide superior return of sensation compared to cross-finger flaps but still less than normal.Neurovascular island flaps may result in hyperesthesia (23%) and cold intolerance (32%), which can beminimized by proper attention to detail and technique.
COMPLICATIONS
Moberg flap: interphalangeal joint flexion contracture and skin necrosisLateral V-Y advancement flaps (Kutler): scarring at the fingertip, which may be insensate or painful Volar V-Y advancement flap (Atasoy-Kleinert): hook nail or hypersensitivityCross-finger flap: deficiency of fingertip pulp and hair growth on the fingertip Thenar flap: PIP joint flexion contracture of recipient fingerHematoma Seroma Infection Skin necrosisDysesthesia or altered sensation Flexion contracturesLoss of flapEpidermal inclusion cysts Nail deformities Symptomatic neuromas
SUGGESTED READINGS
- Atasoy E. Reversed cross-finger subcutaneous flap. J Hand Surg Am 1982;7(5):481-483.
- Barbato BD, Guelmi K, Romano SJ, et al. Thenar flap rehabilitation: a review of 20 cases. Ann Plast Surg 1996;37:135-139.
- Blair WF, ed. Techniques in Hand Surgery. Baltimore: Williams & Wilkins, 1996.
- Baumeister S, Menke H, Wittemann M, et al. Functional outcome after Moberg advancement flaps in the thumb. J Hand Surg Am 2002;27(1):105-114.
- Fitoussi F, Ghobani A, Jehanno P, et al. Thenar flap for severe fingertip injuries in children. J Hand Surg Br 2004;29(2):108-112.
- Foucher G, Delaere O, Citron N, et al. Long-term outcome of neurovascular palmar advancement flaps for distal thumb injuries. Br J Plast Surg 1999;52:64-68.P.1260
- Goitz RJ, Westkaemper JG, Tomaino MM, et al. Soft tissue defects of the digits. Coverage considerations. Hand Clin 1997;13:189-205.
- Green DP, Hotchkiss RN, Pederson WC, eds. Green's Operative Hand Surgery, vol 2, ed 5. Philadelphia: Churchill Livingstone, 1999: 1798-1816.
- Henderson HP, Reid DA. Long-term follow-up of neurovascular island flaps. Hand 1980;12:113-122.
- Kappel DA, Burech JG. The cross-finger flap: an established reconstruction procedure. Hand Clin 1985;1:677-683.
- Koch H, Kielnhofer A, Hubmer M, et al. Donor site morbidity in cross-finger flaps. Br J Plast Surg 2005;58:1131-1135.
- Lau C, Knutson GH, Brown WA. Thenar and palmar-flap repair in finger-tip amputations. Can J Surg 1969;12:294-301.
- Lee NH, Pae WS, Roh SG, et al. Innervated cross-finger pulp flap for reconstruction of the fingertip. Arch Plast Surg 2012;39:637-642.
- Melone CP Jr, Beasley RW, Carstens JH Jr. The thenar flap: an analysis of its use in 150 cases. J Hand Surg Am 1982;7(3):291-297.
- Nicolai JP, Hentennar G. Sensation in cross-finger flaps. Hand 1981;13:12-16.
- Nishikawa H, Smith PJ. The recovery of sensation and function after cross-finger flaps for fingertip injury. J Hand Surg Br 1992;17(1): 102-107.
- Nomura S, Kurakata M, Sekiya S, et al. The modified thenar flap and its usefulness. J Jpn Soc Hand Surg 2000;16:707.
- Okazaki M, Hasegawa H, Kano M, et al. A different method of fingertip reconstruction with the thenar flap. Plast Reconstr Surg 2005;115:885-888.
- Shepard GH. The use of lateral V-Y advancement flaps for fingertip reconstruction. J Hand Surg Am 1983;8(3):254-259.
- Tamai S. Twenty years' experience of limb replantation—review of 293 upper extremity replants. J Hand Surg Am 1982;7:549-556.
- Trumble TE. Principles of Hand Surgery and Therapy. Philadelphia: WB Saunders, 2000:192-200.
