Introduction and Pathogenesis
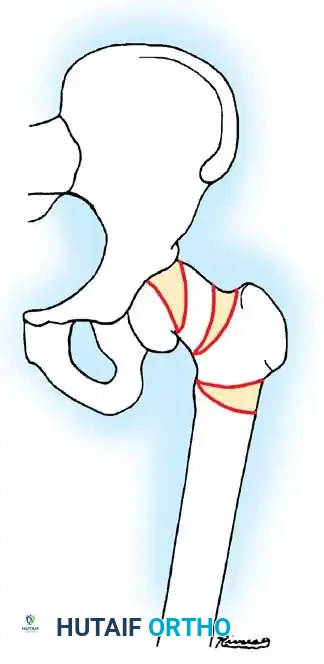
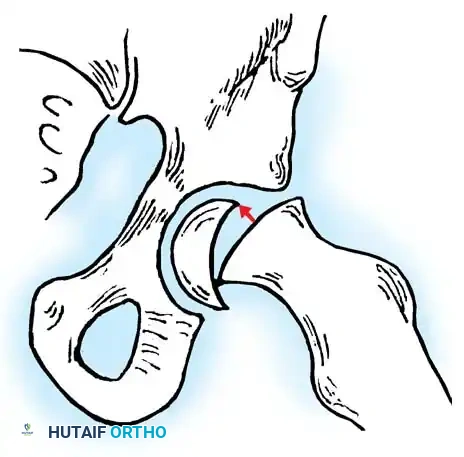
Slipped Capital Femoral Epiphysis (SCFE) represents a unique and complex pediatric hip disorder. While technically a type I transepiphyseal fracture-separation, SCFE is distinguished from standard epiphyseal separations by its distinct natural history, insidious pathogenesis, and biomechanical etiology. The disorder is characterized by the displacement of the proximal femoral epiphysis posteriorly and inferiorly relative to the femoral neck.
The pathogenesis of SCFE is multifactorial, involving a combination of mechanical shear forces and underlying endocrine or metabolic susceptibilities. During the adolescent growth spurt, the physis widens and weakens, making it vulnerable to the increased mechanical loads associated with obesity or rapid growth. Kordelle et al., utilizing three-dimensional computed tomography (CT) analysis in 30 slips, identified significant morphological variations predisposing to SCFE. They noted a reduced femoral anteversion averaging 7 degrees (compared to a normal 12.7 degrees) and a reduced femoral shaft angle of 134.2 degrees (compared to a normal 141 degrees). Furthermore, their analysis confirmed an absence of acetabular remodeling following the slip, underscoring the permanent biomechanical alteration of the joint if left untreated.
Clinical Evaluation and Diagnostic Imaging
The diagnosis of SCFE is typically apparent on high-quality orthogonal radiographs, though a high index of clinical suspicion is required for early or atypical presentations. Patients frequently present with groin, thigh, or referred knee pain, accompanied by an obligate external rotation of the hip during active flexion.
Radiographic Assessment
Standard evaluation mandates an anteroposterior (AP) radiograph of the pelvis and a cross-table (true) lateral view of the affected hip.
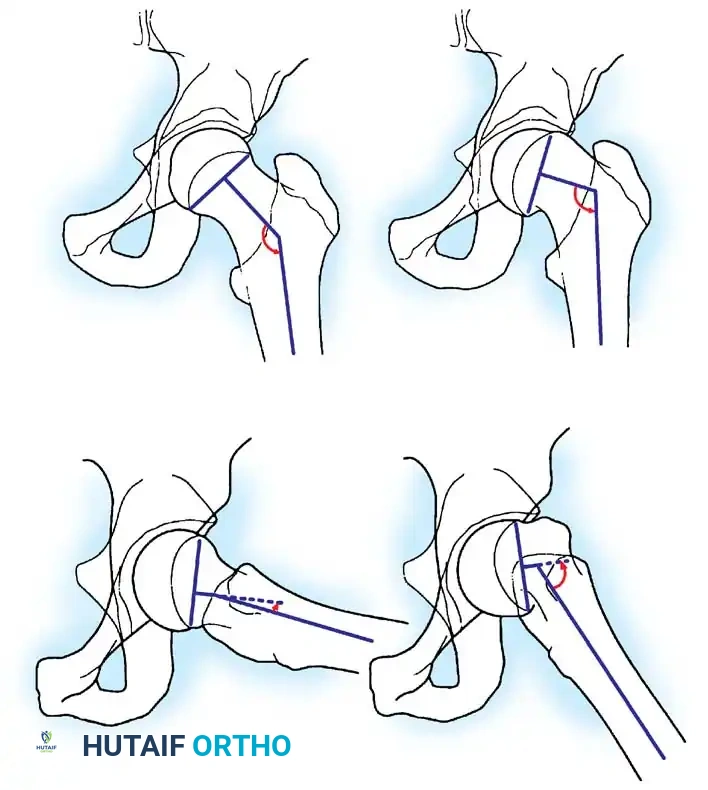
* AP Radiograph: Evaluates the head-shaft angle. The normal femoral head-shaft angle is approximately 145 degrees.
* Lateral Radiograph: Crucial for determining the extent of posterior displacement. The normal head-shaft angle on the lateral view is 170 degrees or more.
* Frog-Leg Lateral: This view best demonstrates subtle, early slipping. However, it must be used with extreme caution—or avoided entirely—in patients with suspected unstable slips, as the positioning maneuver can inadvertently displace the epiphysis further.
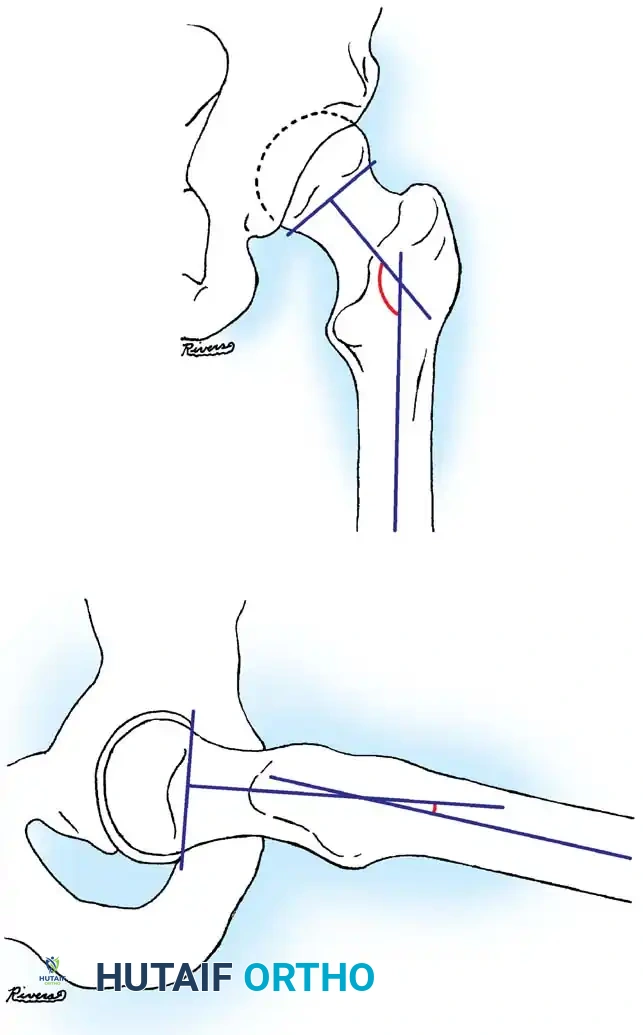
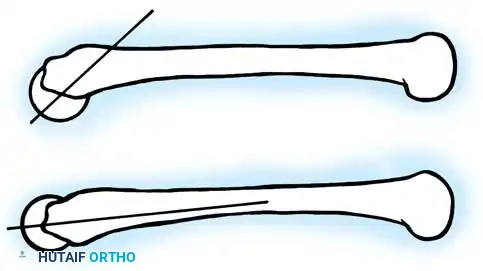
Fig. 33-128 A and B, Measurement of head-shaft angle on anteroposterior and lateral radiographs. Line A connects peripheral portions of the physis. Line B is perpendicular to line A, and line C is in the long axis of the femoral shaft. The intersection of lines B and C forms the head-shaft angle in both views.
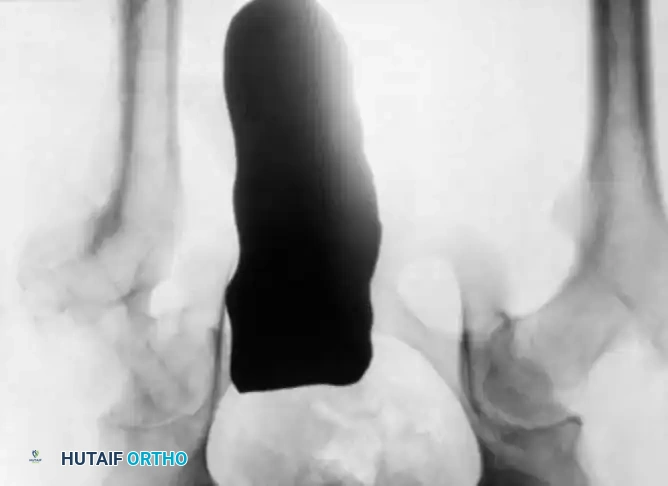
Advanced Imaging Modalities
In cases of "preslip"—an essentially radiographic finding characterized by irregularity, widening, and indistinctness of the physis without overt displacement—advanced imaging is invaluable.
* CT Scanning: Highly sensitive for confirming the diagnosis in patients with early, mild slipping that remains equivocal on plain radiographs.
* Magnetic Resonance Imaging (MRI): While MRI may not always delineate the mechanical slip itself, T2-weighted images are highly sensitive for detecting periphyseal edema. The presence of such edema in a symptomatic adolescent is a definitive harbinger of an impending or early slip.
* Ultrasonography: Occasionally utilized to detect joint effusion associated with acute slips.
Clinical Pearl: Always evaluate the contralateral hip. Prophylactic pinning of the asymptomatic contralateral hip remains a topic of debate but is strongly indicated in patients with atypical SCFE or significant endocrine comorbidities.
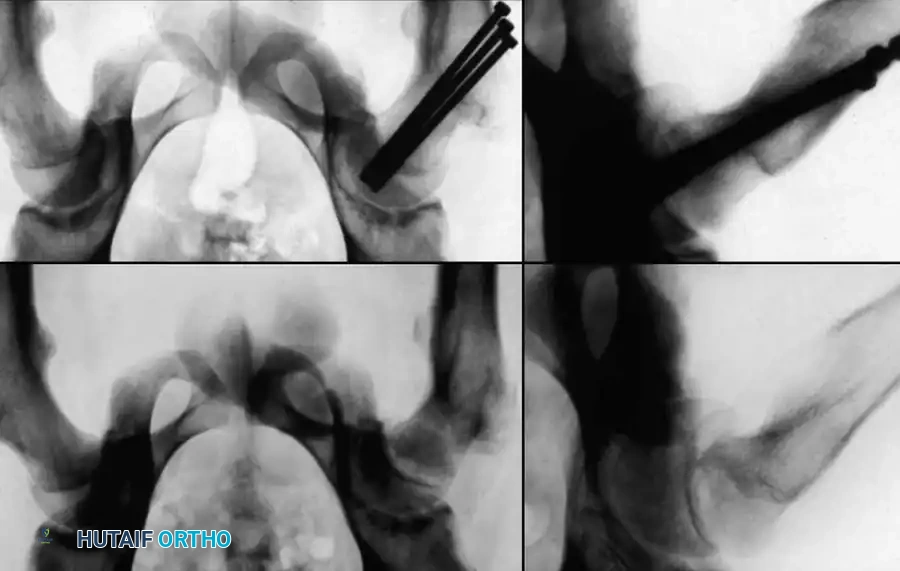
Radiographic Gallery: Diagnosis and Evaluation

Classification Systems
SCFE is classified using three primary paradigms: temporal duration, radiographic severity, and clinical stability. The stability classification is currently the most prognostic regarding the devastating complication of osteonecrosis.
1. Temporal Classification
Traditionally, SCFE has been categorized by the duration of symptoms:
* Acute Slips: Sudden onset of severe symptoms present for less than 2 weeks. Radiographs reveal epiphyseal displacement with absolutely no evidence of bone healing or remodeling.
* Chronic Slips: Gradual onset of symptoms lasting longer than 2 weeks. Radiographs demonstrate bony healing and remodeling along the posterior and medial femoral neck.
* Acute-on-Chronic Slips: Symptoms lasting longer than 1 month, punctuated by a recent, sudden exacerbation of pain following a relatively trivial injury.
In a landmark 1982 review by Ingram et al. of 329 slips, the distribution was: 60% chronic, 23% acute-on-chronic, 11% acute, and 6% preslips.
2. Radiographic Severity (Southwick Classification)
Severity is graded based on the degree of displacement relative to the femoral neck diameter or the deviation of the head-shaft angle:
* Mild (Grade I): Displacement < 1/3 of the femoral head diameter, or head-shaft angle deviation ≤ 30 degrees. (Comprises >50% of cases).
* Moderate (Grade II): Displacement between 1/3 and 1/2 of the diameter, or angle deviation between 30 and 60 degrees.
* Severe (Grade III): Displacement > 1/2 of the diameter, or angle deviation > 60 degrees.
3. Stability Classification (Loder Classification)
Described by Loder et al., this simple two-part classification is the universally accepted standard today, as it directly correlates with the risk of avascular necrosis (AVN).
* Stable SCFE: The patient is able to walk or bear weight on the affected limb, with or without crutches. Satisfactory outcomes are achieved in approximately 96% of these cases.
* Unstable SCFE: Severe pain prevents walking, even with crutches, regardless of symptom duration. This is a true orthopedic emergency. In Loder's series, satisfactory results were obtained in only 47% of unstable slips, primarily due to a high incidence of osteonecrosis.
4. Etiological Classification: Idiopathic vs. Atypical
Loder et al. also evaluated 433 children to determine predictors of atypical SCFE (associated with renal failure, radiation therapy, or endocrine disorders like hypothyroidism). Children younger than 10 years or older than 16 years were 4.2 times more likely to have atypical SCFE, and 8.4 times more likely if their weight was below the 50th percentile.
Treatment Philosophy and Modalities
The ideal treatment of SCFE must achieve three goals: prevent additional slipping, stimulate early physeal closure, and avoid the triad of complications—osteonecrosis, chondrolysis, and osteoarthritis.
Historical Nonoperative Management
Historically, nonoperative treatment via traction and spica cast immobilization was utilized. While Davidson et al. reported a lower prevalence of osteonecrosis after cast treatment (1.6%) compared to pinning (3%), chondrolysis was unacceptably high (14.3% vs. 1.9%). Betz et al. suggested casting as an alternative, noting chondrolysis in 13.5% of hips with no osteonecrosis. However, due to the high morbidity and chondrolysis risk, nonoperative management is rarely, if ever, indicated today.
Operative Management: The Gold Standard
Operative modalities include percutaneous in situ pinning, open reduction and internal fixation (ORIF), epiphysiodesis, and corrective osteotomies. For the vast majority of mild, moderate, and severe acute or chronic slips, percutaneous in situ pinning is the treatment of choice.
Single vs. Multiple Pin Fixation
Historically, multiple pins (Knowles pins, threaded Steinmann pins) were used. However, contemporary evidence overwhelmingly supports the use of a single, large-diameter central cannulated screw.
* Biomechanical Evidence: Kibiloski et al. subjected bovine SCFE models to physiological shear loads (100 cycles at 1.1 Hz; 400 N for slow walking, 900 N for fast walking). They found no significant difference in creep between single-screw and double-screw fixation.
* Clinical Evidence: Blanco et al. compared single vs. multiple pins in 114 hips. Complications occurred in only 4.6% of single-pin hips versus 36% of multiple-pin hips. O’Beirne et al. reported zero slip progression or pin breakage with single-pin fixation. Aronson and Loder similarly reported excellent outcomes using single cannulated screws in 97 slips.
Surgical Warning: Laplaza and Burke noted that the epiphysis "grew off" the pins in 18% of hips treated with threaded Steinmann pins. Cannulated screws with reverse-cutting flutes prevent this phenomenon and are easier to remove once the physis has closed.
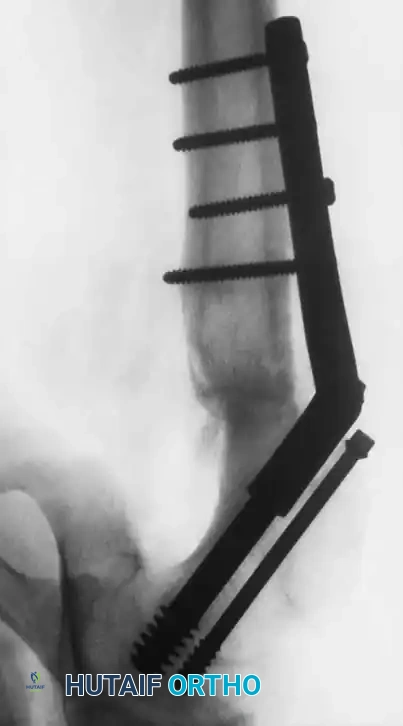
Dynamic Screw Fixation for Atypical SCFE
In young patients with atypical SCFE (e.g., renal osteodystrophy), premature physeal closure can lead to severe leg-length discrepancies. Oppenheim et al. recommended Steinmann pins that are smooth distally and threaded proximally. More recently, Kumm et al. described single dynamic screw fixation.
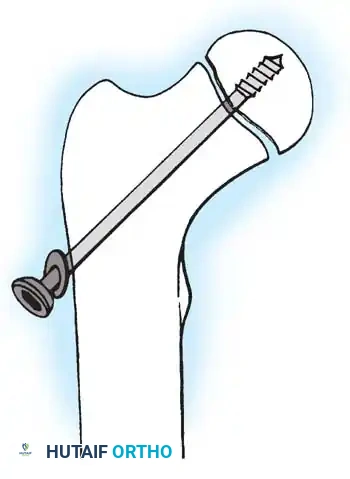
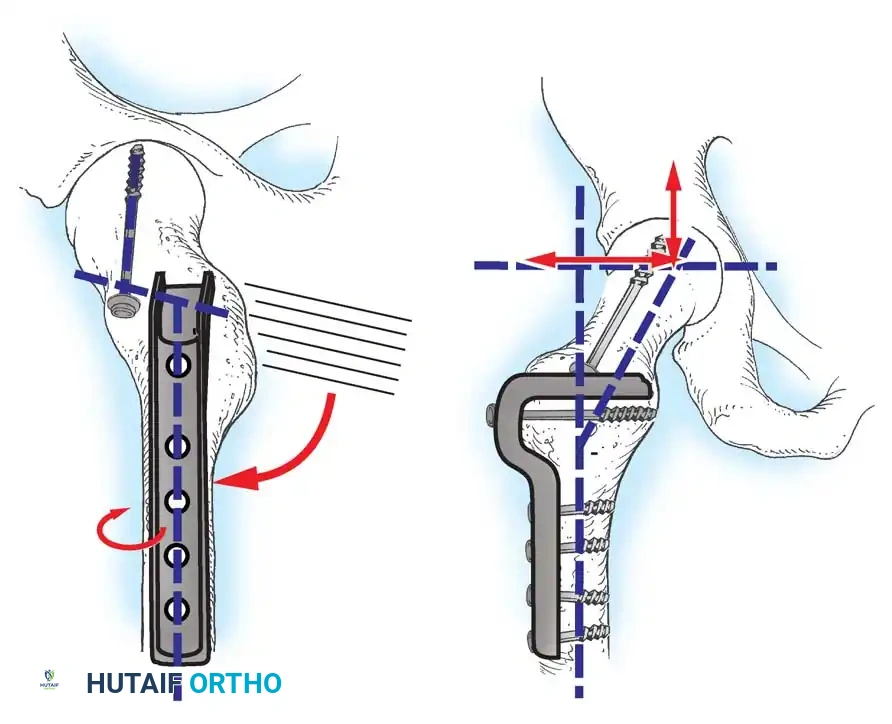
Fig. 33-129 Principle of dynamic screw fixation. A short screw thread (10 mm) engages the epiphysis only, and the screw and washer are left protruding 15 to 20 mm to accommodate continued growth.
Using a 7 mm cannulated screw with 10-mm threads placed precisely in the center of the femoral head, the screw is left protruding 15 to 20 mm laterally. In their study of 29 hips, the femoral neck continued to grow approximately 15 mm without premature physeal closure or loss of fixation.
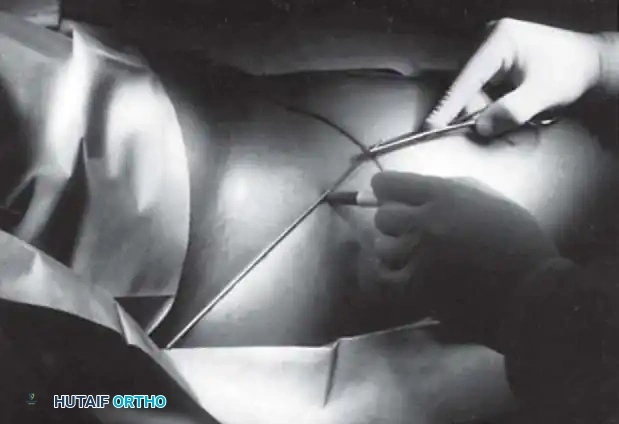
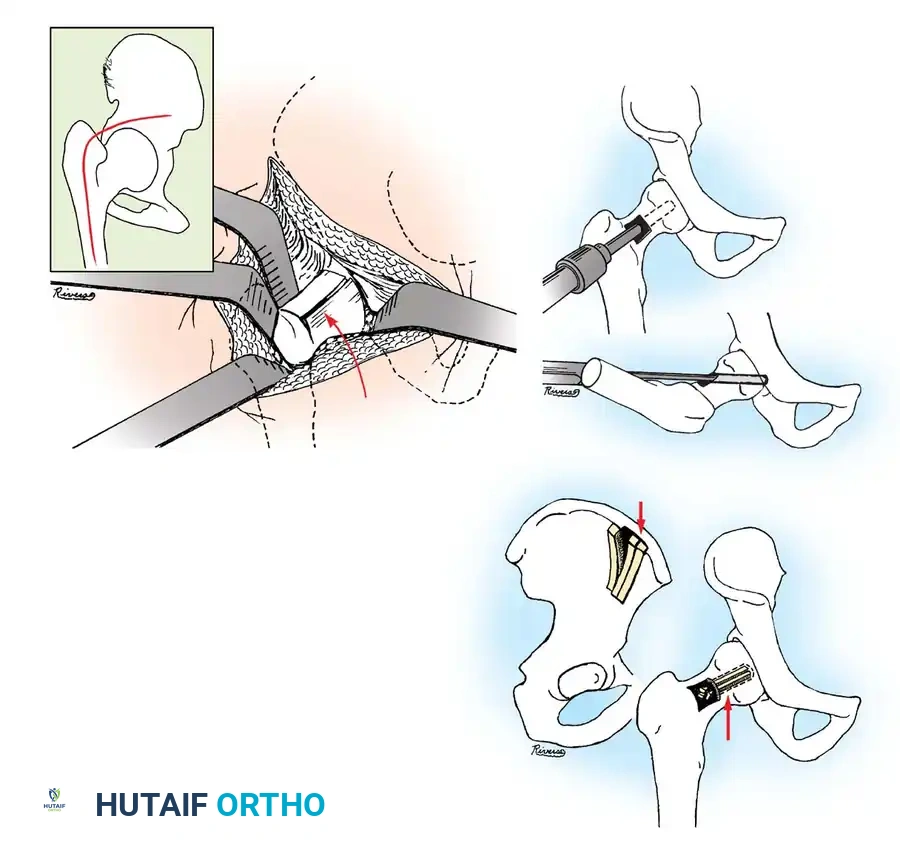
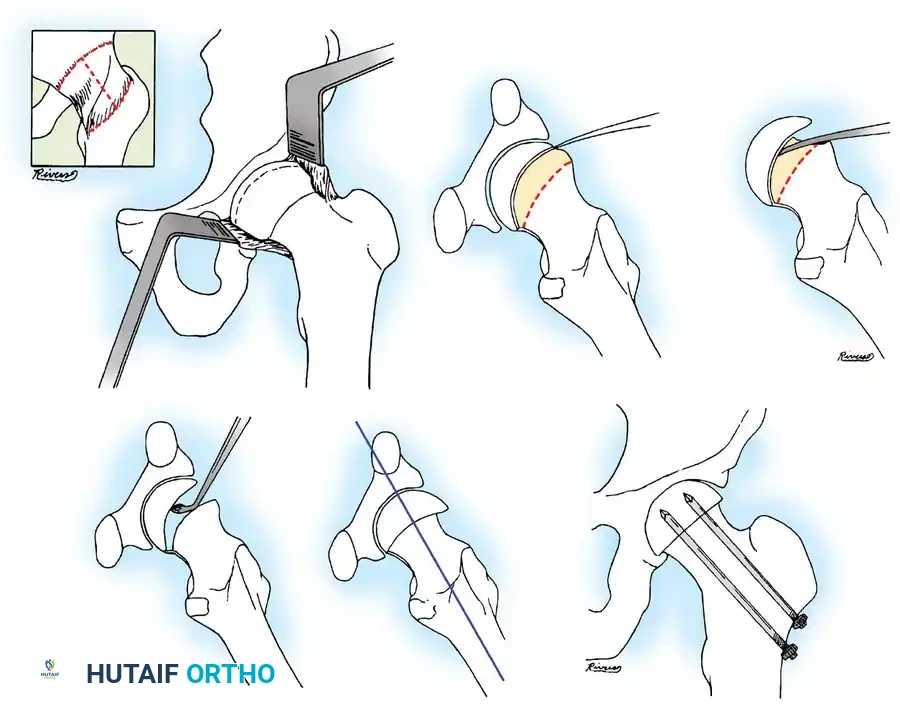
Surgical Technique: Percutaneous In Situ Pinning
Percutaneous single cannulated screw fixation is the preferred technique for over 90% of SCFE cases. It minimizes morbidity and allows for highly accurate, fluoroscopically guided hardware placement.
1. Preoperative Planning and Positioning
The patient is placed supine on a radiolucent fracture table.
* Stable Slips: The limb is positioned in its resting state of external rotation. Do not attempt forceful internal rotation or reduction, as this drastically increases the risk of iatrogenic osteonecrosis by kinking the delicate retinacular vessels.
* Unstable Slips: Gentle, incidental reduction may occur during positioning, but aggressive manipulation remains contraindicated. Some surgeons prefer open capsulotomy for unstable slips to decompress the joint hematoma, though this remains controversial.
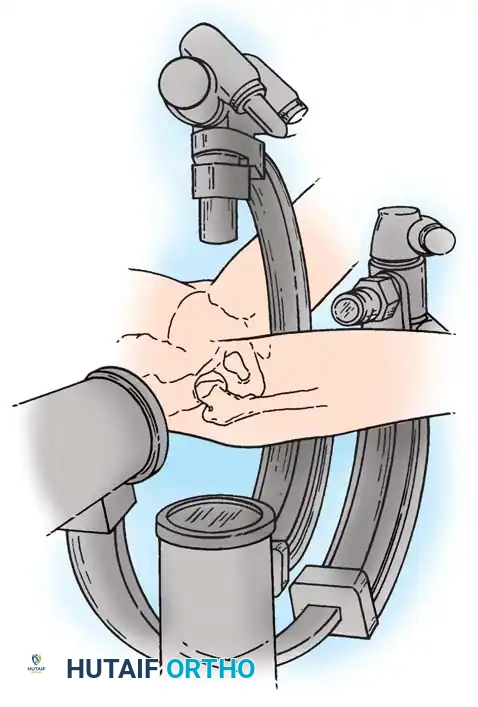


2. Fluoroscopic Setup and the "Rotating Beam" Technique
In situ pinning is fundamentally a radiographic technique. Menche, Lehman, Rab, Moseley, and Morrissy have all emphasized the absolute necessity of a rotating fluoroscopic beam.
The C-arm must be able to rotate freely through a 90-degree arc from the AP to the true lateral position without moving the patient's leg.




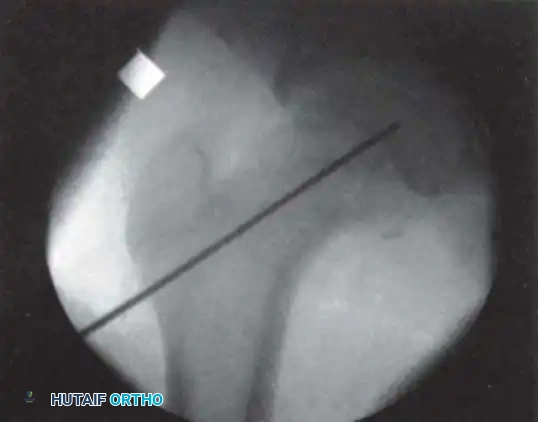
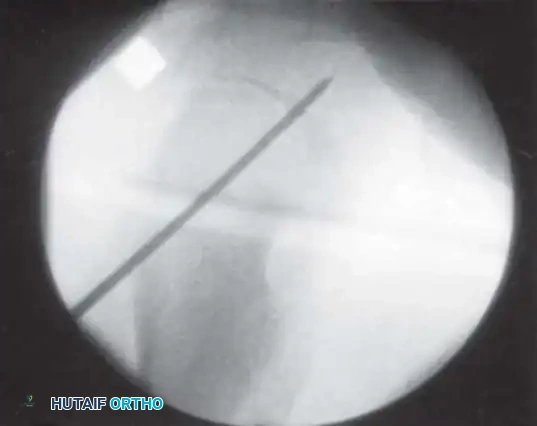
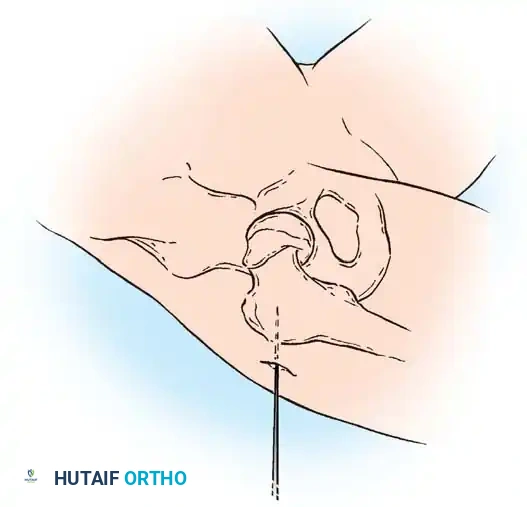
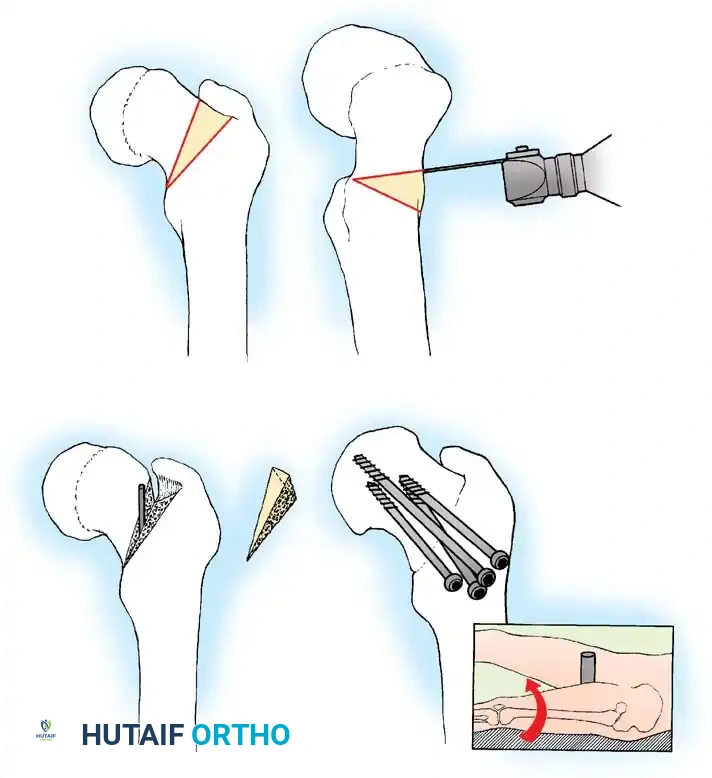
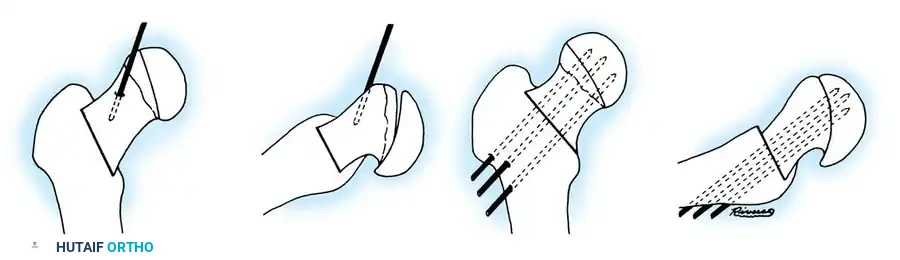
3. Guidewire Placement: The Morrissy Principles
Morrissy identified two common errors in SCFE pinning:
1. Passing the pin obliquely toward the anterior surface rather than the center of the head.
2. Passing the pin out the posterior neck and into the head.
To avoid this, the starting point must be selected based on the position of the displaced femoral head. The guidewire must enter the femoral neck so that it crosses the physis perpendicular to its surface and anchors in the exact center of the epiphysis.
* Because the head slips posteriorly, the starting point on the lateral cortex must move anteriorly. The more severe the slip,
Associated Surgical & Radiographic Imaging

📚 Medical References
- Slipped capital femoral epiphysis associated with renal failure osteodystrophy, J Pediatr Orthop 17:205, 1997.
- Loeffl er R, Sherman F: The effect of treatment on growth and deformity in hypophosphatemic vitamin D-resistant rickets, Clin Orthop Relat Res 162:4, 1982.
- Mankin HJ: Rickets, osteomalacia, and renal osteodystrophy: 1, J Bone Joint Surg 56A:101, 1974.
- Mankin HJ: Rickets, osteomalacia, and renal osteodystrophy: 2, J Bone Joint Surg 56A:352, 1974.
- Mankin HJ: Metabolic bone disease, J Bone Joint Surg 76A:760, 1994.
- Nicol RO, Williams PF, Hill DJ: Transient osteopaenia of the hip in children, J Pediatr Orthop 4:590, 1984.
- Oppenheim WL, Fischer SR, Salusky IB: Surgical correction of angular deformity of the knee in children with renal osteodystrophy, J Pediatr Orthop 17:41, 1997.
- Scriver CR, Reade T, Halal F, et al: Autosomal hypophosphatemic bone disease responds to 1,25-(OH) 2 D 3 , Arch Dis Child 56:203, 1981.
- Sheridan RN, Chiroff RT, Friedman EM: Operative and nonoperative treatment of rachitic lower extremity deformities: a long-term study with 46-year average follow-up, Clin Orthop Relat Res 116:66, 1976.
- Smith R: Idiopathic osteoporosis in the young, J Bone Joint Surg 62B:427, 1980.
