Shoulder ultrasound is a safe, efficient, and cost-effective method for diagnosing rotator cuff tears. It is comparable to magnetic resonance imaging (MRI) in both sensitivity and specificity. This article provides an overview of the normal shoulder ultrasound appearance and how to perform a shoulder ultrasound examination.
Mohammad Hutaif
,
Emial
General principles Ultrasound basics:1
> Ultrasound uses the principles of sonar developed for ships at sea
> A transducer is used to produce sound waves
> When the sound waves encounter a border between two tissues that conduct
> sound differently some of the sound waves bounce back creating an echo
> The transducer detects the returning echoes which are analyzed by a computer and transformed into an image
> The more dense the tissue, the brighter the appearance on the image.
Definitions: 1 Echogenicity
:
The type of echo display: Anechoic/hypoechoic/hyperechoic.
Anechoic:
Without echoes; black; fluid filled structures; in shoulder pathology, anechoic signals typically represents pathology (e.g., effusion, tissue tear).
Hypoechoic:
With low-level echoes; grays; more solid structure.
Hyperechoic:
Bright echoes; white; dense or strong reflector.
Isoechoic:
Same echogenicity.
Attenuation
:
Loss of ene
rgy as a sound pulse travels through a medium.
Long-axis:
Along the length of the structure.
Short-axis:
Across the width of the structure.
Anisotropy:
An artifactual hypoechoic appearance of a normal hyperechoic structure that occurs because the transducer is not perpendicular to the structure being imaged
You can help combat this by maintaining an angle of close to 90 degrees between the probe and the structure of interest.
Frequency:
The range of sound waves produced by a transducer (measured in MHz)
The higher the frequency the better image detail, but lesser the penetration; a high-frequency transducer (12 to 15 MHz) is typically used to evaluate the shoulder
The lower the frequency the lesser image detail, but better the penetration; lower frequency transducer (9 MHz) may be used to achieve greater tissue penetration, which may be necessary when evaluating deeper structures such as when evaluating patients with a large body habitus.
Advantages of ultrasound:
- Cost-effective
- Safe
- Improves efficiency in the management of rotator cuff disease2
- Dynamic
- Accurate for detecting large and massive rotator cuff tears3,6
- Comparable to magnetic resonance imaging (MRI) in both sensitivity and
- specificity7
- Can be used in patients with contraindications to MRI (pacemaker,
- claustrophobia, etc.)
- Accurate for evaluating the rotator cuff in shoulders that have undergone an
- operation:
- Less susceptibility to suture anchor artifact.8
-
Allows for image guided injections.
Disadvantages:
Long learning curve:
100 ultrasound examinations recommended prior to clinical application.9,10
Operator dependent
Difficult with obese/well-muscled patients
Less sensitive for detecting partial-thickness rotator cuff tears and ruptures of
the biceps6
Does not evaluate intraarticular structures well (labrum, biceps anchor, etc.). Normal shoulder examination
Long head biceps tendon (LHBT): Patient position: Performed with shoulder in neutral or slight internal rotation, elbow
flexed 90 degrees, and forearm supinated and resting on the patient’s lap.
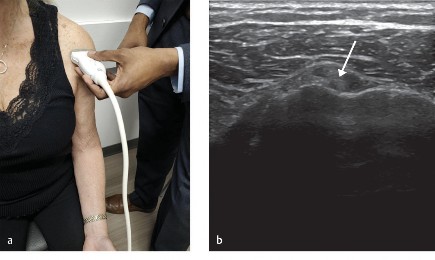
Short-axis image (▶ Fig. 6.1a, b ):
Hold the probe transversely with respect to the longitudinal axis of the LHBT

 Fig. 6.1 Long head biceps tendon (LHBT). (a) Patient and probe position for imaging the LHBT in short-axis. (b) Short-axis image of LHBT (arrow). (c) Patient and probe position for imaging the LHBT in long-axis. (d) Long-axis image of LHBT (short arrows).
Image is equivalent to an axial view on MRI Normal appearance:
Homogeneous, round, or ovoid hyperechoic structure (2–4 mm thick) located in the bicipital groove with trace amount of fluid within its tendon sheath.
Fig. 6.1 Long head biceps tendon (LHBT). (a) Patient and probe position for imaging the LHBT in short-axis. (b) Short-axis image of LHBT (arrow). (c) Patient and probe position for imaging the LHBT in long-axis. (d) Long-axis image of LHBT (short arrows).
Image is equivalent to an axial view on MRI Normal appearance:
Homogeneous, round, or ovoid hyperechoic structure (2–4 mm thick) located in the bicipital groove with trace amount of fluid within its tendon sheath.
Long-axis image (▶ Fig. 6.1c, d ):
Rotate the probe 90 degrees so that it is oriented along the longitudinal axis of the LHBT
Image is equivalent to a sagittal-oblique view on MRI
This image is typically used when performing a biceps tendon sheath injection
Normal appearance:
Smooth and fibrillar.
Subscapularis tendon:
Patient position:
Performed with shoulder in external rotation, elbow flexed 90 degrees,
and forearm supinated
External rotation delivers the tendon out from underneath the coracoid process.
Long-axis image (▶ Fig. 6.2a, b ):
Hold the probe so that it is aligned along the longitudinal axis of the
subscapularis muscle fibers
Image is equivalent to an axial view on MRI
Normal appearance:
Tendon is hyperechoic and convex shaped, tapering toward its insertion on the lesser tuberosity. Normal hypoechoic muscle should not be mistaken for fluid.
Short-axis image (▶ Fig. 6.2c, d ):
Rotate the probe 90 degrees so that it is oriented perpendicular to the
subscapularis muscle fibers
Image is equivalent to a sagittal-oblique view on MRI
Good for evaluating superior subscapularis tendon tears.
Supraspinatus tendon:
Patient position:
Patient is directed to place the palm of his or her hand on the ipsilateral
hip or buttock, with elbow flexed and adducted against the body
This allows the supraspinatus tendon to come out from underneath the acromion process.
Long-axis image (▶ Fig. 6.3a, b ):
Hold the probe so that it is aligned along the longitudinal axis of the supraspinatus muscle fibers. The muscle fibers and tendon of the supraspinatus are oriented anterolaterally


Fig. 6.2 Subscapularis tendon. (a) Patient and probe position for imaging the subscapularis in long-axis. (b) Long-axis image of subscapularis tendon (arrows). (c) Patient and probe position for imaging the subscapularis in short-axis. (d) Short-axis image of subscapularis tendon (arrows).
While maintaining probe in the same axis, scan from anterior to posterior
Image is equivalent to a coronal-oblique view on MRI
Biceps tendon marks the anterior leading edge of the supraspinatus. Posterior supraspinatus is marked by the change in shape of the greater tuberosity, from ledge-like to flat. This area of transition is where the fibers of the posterior supraspinatus and anterior infraspinatus interdigitate and may be mistaken for a tear if the orientation of the probe is not corrected.
Fig. 6.3 Supraspinatus tendon. (a) Patient and probe position for imaging the supraspinatus in long-axis. (b) Long-axis image of the supraspinatus tendon (arrows). (c) Patient and
probe position for imaging the supraspinatus in short-axis. Note long head biceps tendon (LHBT) visualized anterior to the supraspinatus tendon (arrow). (d) Short-axis image of the supraspinatus tendon (short arrows). (e) Illustration of supraspinatus in long-axis (left) and short axis (right) showing the articular (arrows) and bursal (curved arrows) surfaces of the supraspinatus tendon. BT, biceps tendon; ST, supraspinatus tendon. (Adapted from Jacobson JA. Fundamentals of Musculoskeletal Ultrasound.)




Normal appearance:
Smooth, hyperechoic, and fibrillar, tapering at its insertion or
footprint.
Subacromial-subdeltoid bursa:
The subacromial-subdeltoid bursa is located between the rotator cuff
and the overlying deltoid muscle and acromion
The bursae is a potential space which consists of a thin hypoechoic band measuring less than 2 mm surrounded by a thin hyperechoic line superficial and deep to this. It should have a smooth appearance throughout.
Short-axis image (▶ Fig. 6.4c d ):
Turn probe 90 degrees so that it is aligned perpendicular to the longitudi-
nal axis of the supraspinatus muscle fibers
Image is equivalent to a sagittal-oblique view on MRI
While maintaining probe in the same axis, scan from medial to lateral
Normal appearance:
The hyperechoic lines of the humeral head and the bursal border of the supraspinatus parallel each other.
Infraspinatus tendon:
Patient position:
Performed with shoulder in neutral rotation, elbow flexed 90 degrees, and forearm supinated and resting on the patient’s lap.
Long-axis image (▶ Fig. 6.4a, b ):
Hold the probe below the scapular spine. Align it so that it is along the
longitudinal axis of the infraspinatus muscle fibers
Image is equivalent to an axial view on MRI
Normal appearance:
Similar fibrillar pattern as supraspinatus tendon; tendon is hyperechoic and tapers toward its insertion on the greater tuberosity. Central tendon can be identified within the surrounding hypoechoic infraspinatus muscle.
Short-axis image (▶Fig. 6.4c, d ):
Turn probe 90 degrees so that it is aligned perpendicular to the longitudi-
nal axis of the infraspinatus muscle fibers
Image appears similar to sagittal-oblique MRI
While maintaining probe in the same axis, scan from medial to lateral
Normal appearance:
Similar echogenicity as supraspinatus.
Fig. 6.4 Infraspinatus tendon. (a) Patient and probe position for imaging the infraspinatus in long-axis. (b) Long-axis image of infraspinatus tendon (arrows). (c) Patient and probe position for imaging the infraspinatus in short-axis. (d) Short-axis image of infraspinatus tendon (arrows).


Coracoid and anterior glenohumeral joint:
Patient position:
Performed with shoulder in external rotation, elbow flexed 90 degrees,
and forearm supinated.
Long-axis image (▶ Fig. 6.5a, b ):
Hold the probe in the same position as the long-axis image for the subscapularis tendon (i.e., along the longitudinal axis of the subscapularis muscle fibers). While maintaining the probe in this axis, slide the probe medially
Image is equivalent to an axial view on MRI

Fig. 6.5 Coracoid and anterior glenohumeral joint. (a) Patient and probe position for long-axis view of coracoid and anterior glenohumeral joint. (b) Long-axis image of coracoid (arrow), subscapularis (short arrows) and humeral head (asterisk).
Typically used for measuring the coracohumeral interval and performing anterior glenohumeral joint injections
Normal appearance:
There should be an absence of fluid inside the joint.
Posterior glenohumeral joint:
Patient position:
Performed with shoulder in neutral rotation, elbow flexed 90 degrees, and forearm supinated and resting on the patient’s lap.
Long-axis image (▶ Fig. 6.6a–c ):
Hold the probe in the same position as the long-axis image for the infraspinatus (i.e., along the longitudinal axis of the infraspinatus muscle fibers). While maintaining the probe in this axis, slide medially
Image is equivalent to an axial view on MRI
Typically used for posterior glenohumeral joint injections for conditions such as adhesive capsulitis or degenerative joint disease
Normal appearance:
There should be an absence of any fluid inside the joint.
Acromioclavicular (AC) joint:
Patient position:
Performed with shoulder in neutral rotation, elbow flexed 90 degrees, and forearm resting on the patient’s lap.
Fig. 6.6 Posterior glenohumeral joint. (a) Patient and probe position for long-axis view of the posterior glenohumeral joint. (b) Long-axis image of the posterior glenohumeral joint showing the humeral head (long arrow) and glenoid (asterisk) and labrum (short arrow). (c) Illustration of posterior glenohumeral joint.


Long-axis image (▶ Fig. 6.7a, b ):
Hold the probe so that it is aligned along the longitudinal axis of the distal end of the clavicle
Image is equivalent to a coronal view
Used for AC joint injections
Normal appearance:
There should be no abnormal joint widening or narrowing, joint
margin irregularity, step-off, or capsular bulging.

Fig. 6.7 Acromioclavicular(AC) joint. (a) Patient and probe position for long-axis view of the AC joint.
(b) Long-axis image of the AC joint (asterisk), distal clavicle (long arrow), acromion (short arrow).
Pathologic conditions
> LHBT:
> Long head biceps tendinosis:
> Thickening, loss of normal echogenicity, and loss of normal fibrillar pattern.
> Partial-thickness (longitudinal intrasubstance) tear:
> May occur due to chronic tendinosis
> Results in an anechoic void within the tendon, without complete discontinuity
> These tears are often longitudinally oriented.
> Full-thickness tear:
> Complete tear with distal retraction is characterized by nonvisualization of the tendon within the intertubercular groove (i.e., “empty groove”)
> Echogenic material may be present in the groove
> Clinically correlate with a Popeye deformity
> If an empty groove is visualized, assess for medial dislocation of the tendon which may signify a tear of the subscapularis tendon.
> Subscapularis tendon: > Subcoracoid impingement: > Dynamic scanning can be used to confirm impingement between the coracoid and the underlying subscapularis tendon by internally and externally rotating the shoulder.
> Full-thickness tear:
> Medial subluxation of the LHBT deep to the subscapularis tendon and into the glenohumeral joint signifies a full-thickness tear of the subscapularis tendon.
> Supraspinatus and infraspinatus:
> Rotator cuff tendinosis:
> Tendon appears heterogeneous or hypoechoic, with tendon thickening, and loss of the normal fibrillar pattern.
> Partial-thickness rotator cuff tears (▶ Fig. 6.8a–f ):
> Focal area of hypoechogenicity or mixed echogenicity involving one side
> of the tendon, but not extending through the entire thickness
> May be bursal-sided, articular-side, or intrasubstance.
> Full-thickness rotator cuff tears (▶ Fig. 6.8g, h ):
> Ultrasound is a reliable method for diagnosis of full-thickness rotator cuff tears, with sensitivity and specificity over 90%
> Ultrasound is less reliable to pick up partial-thickness tears
> Full-thickness tears are visualized as a hypoechoic or anechoic gap within the rotator cuff
> When looking at the sagittal view, the hyperechoic lines of the bursal border and articular head are parallel to each other; in the case of a rotator cuff, the bursal border may have a concave contour as the deltoid drops into the cuff defect
> Alternatively, a greatly retracted tear can result in nonvisualization of the rotator cuff tendon > Dynamic contraction test: Ask the patient to abduct his or her shoulder against resistance. This isometric contraction is used to uncover nondis-placed full-thickness tears, or significant partial-thickness tears. Subacromial-subdeltoid bursa: > Abnormalities of the bursa manifest with increased fluid within and distention of the bursa, and/or by bursal wall thickening.




Fig. 6.8 Pathologic conditions of the supraspinatus tendon. (a) Long-axis and (b) short-axis of articular-sided partial-thickness rotator cuff tear. (c) Long-axis and (d) short-axis of bursal-sided partial-thickness rotator cuff tear. (e) Long-axis and (f) short-axis illustration of interstitial partial-thickness rotator cuff tear. (g) Long-axis and (h) short-axis illustration of full-thickness rotator cuff tear. (Adapted from Jacobson JA. Fundamentals of Musculoskeletal Ultrasound.)
Scientific References
- 1. [Jacobson JA. Chapter 1, Introduction. In: Fundamentals of Musculoskeletal Ultrasound. Saunders W.B.;](#bookmark11) [View Source / PubMed]
- 2. [2017](#bookmark11) [View Source / PubMed]
- 3. [Ziegler DW. The use of in-office, orthopaedist-performed ultrasound of the shoulder to evaluate and manage rotator cuff disorders. J Shoulder Elbow Surg 2004;13(3):291–297](#bookmark11) [View Source / PubMed]
- 4. [Al-Shawi A, Badge R, Bunker T. The detection of full thickness rotator cuff tears using ultrasound. J Bone](#bookmark11) [View Source / PubMed]
- 5. [Joint Surg Br 2008;90(7):889–892](#bookmark11) [View Source / PubMed]
- 6. [Roy JS, Braën C, Leblond J, et al. Diagnostic accuracy of ultrasonography, MRI and MR arthrography in the characterisation of rotator cuff disorders: a systematic review and meta-analysis. Br J Sports Med 2015;49(20):1316–1328](#bookmark11) [View Source / PubMed]
- 7. [Iannotti JP, Ciccone J, Buss DD, et al. Accuracy of office-based ultrasonography of the shoulder for the diagnosis of rotator cuff tears. J Bone Joint Surg Am 2005;87(6):1305–1311](#bookmark11) [View Source / PubMed]
- 8. [Teefey SA, Hasan SA, Middleton WD, Patel M, Wright RW, Yamaguchi K. Ultrasonography of the rotator cuff: a comparison of ultrasonographic and arthroscopic findings in one hundred consecutive cases. J Bone Joint Surg Am 2000;82(4):498–504](#bookmark11) [View Source / PubMed]
- 9. [de Jesus, Parker L, Frangos AJ, Nazarian LN. Accuracy of MRI, MR arthrography, and ultrasound in the diagnosis of rotator cuff tears: a meta-analysis. AJR Am J Roentgenol 2009;192(6):1701–1707](#bookmark11) [View Source / PubMed]
- 10. [Prickett WD, Teefey SA, Galatz LM, Calfee RP, Middleton WD, Yamaguchi K. Accuracy of ultrasound imaging](#bookmark11) [View Source / PubMed]
- 11. [of the rotator cuff in shoulders that are painful postoperatively. J Bone Joint Surg Am 2003;85(6):1084–1089](#bookmark11) [View Source / PubMed]
- 12. [Alavekios DA, Dionysian E, Sodl J, Contreras R, Cho Y, Yian EH. Longitudinal analysis of effects of operator experience on accuracy for ultrasound detection of supraspinatus tears. J Shoulder Elbow Surg 2013;22(3):375–380](#bookmark11) [View Source / PubMed]
- 13. [Murphy RJ, Daines MT, Carr AJ, Rees JL. An independent learning method for orthopaedic surgeons performing shoulder ultrasound to identify full-thickness tears of the rotator cuff. J Bone Joint Surg Am 2013;95(3):266–272](#bookmark11) ## ## Shoulder Ultrasound MCQs [View Source / PubMed]
- 1. What is the most common indication for shoulder ultrasound? [View Source / PubMed]
- 1. Rotator cuff tear [View Source / PubMed]
- 2. Biceps tendon tear [View Source / PubMed]
- 3. Subacromial bursitis [View Source / PubMed]
- 4. Impingement syndrome The correct answer is** Rotator cuff tear**. [View Source / PubMed]
- 2. Which of the following is not a normal finding on shoulder ultrasound? [View Source / PubMed]
- 1. Anechoic subacromial bursa [View Source / PubMed]
- 2. Hyperechoic supraspinatus tendon [View Source / PubMed]
- 3. Hypoechoic infraspinatus tendon [View Source / PubMed]
- 4. Biceps tendon sheath with trace amount of fluid The correct answer is** Hypoechoic infraspinatus tendon**. [View Source / PubMed]
- 3. What is the best position for imaging the long head biceps tendon? [View Source / PubMed]
- 1. Short-axis view [View Source / PubMed]
- 2. Long-axis view [View Source / PubMed]
- 3. Transverse view [View Source / PubMed]
- 4. Coronal view The correct answer is** Long-axis view**. [View Source / PubMed]
- 4. What is the best position for imaging the supraspinatus tendon? [View Source / PubMed]
- 1. Short-axis view [View Source / PubMed]
- 2. Long-axis view [View Source / PubMed]
- 3. Transverse view [View Source / PubMed]
- 4. Coronal view The correct answer is** Long-axis view**. [View Source / PubMed]
- 5. What is the most common type [View Source / PubMed]
