Introduction & Epidemiology
Sternoclavicular (SC) joint dislocations, while rare, represent a distinct clinical challenge within orthopedic trauma. Constituting less than 3% of all shoulder girdle injuries and less than 1% of all dislocations, their infrequency belies their potential for significant morbidity. The mechanism of injury typically involves high-energy trauma, often from motor vehicle accidents or direct sports-related impact.
Dislocations are broadly classified based on the direction of clavicular displacement relative to the sternum:
*
Anterior Dislocations
: The most common type, accounting for approximately 90% of SC joint dislocations. The medial clavicle displaces anteriorly and superiorly. While generally considered less dangerous than posterior dislocations, they can cause chronic pain, instability, and cosmetic deformity.
*
Posterior Dislocations
: A critical injury, comprising approximately 10% of SC joint dislocations. The medial clavicle displaces posteriorly into the superior mediastinum. Due to the proximity of vital structures (trachea, esophagus, subclavian vessels, brachial plexus, pleura), posterior dislocations carry a substantial risk of life-threatening complications, including airway obstruction, vascular injury, and pneumothorax.
Further classifications include:
*
Acute
: Less than 3 weeks from injury.
*
Subacute
: Between 3 weeks and 3 months from injury.
*
Chronic
: Greater than 3 months from injury.
*
Complete vs. Incomplete
: Based on the degree of ligamentous disruption.
*
Open vs. Closed
: Open dislocations are surgical emergencies due to infection risk and potential for greater soft tissue damage.
Accurate diagnosis and timely intervention are paramount, particularly for posterior dislocations, to mitigate severe complications and optimize long-term functional outcomes.
Surgical Anatomy & Biomechanics
The sternoclavicular joint is a diarthrodial saddle joint, unique for its ability to provide significant mobility while maintaining remarkable stability. It is the sole bony articulation between the upper extremity and the axial skeleton.
Anatomical Components:
- Articular Surfaces : The medial end of the clavicle articulates with the manubrium sterni and the first costal cartilage. These surfaces are incongruent, with the clavicular facet being larger than the sternal facet.
- Articular Disc : A crucial biconcave fibrocartilaginous disc located within the joint. It acts as a shock absorber, improves joint congruity, and divides the joint into two separate synovial cavities. The disc attaches superiorly to the posterosuperior aspect of the clavicle and inferiorly to the first costal cartilage and anteriorly and posteriorly to the joint capsule.
- Joint Capsule : A robust fibrous capsule encloses the joint, reinforced by a number of ligaments.
-
Ligaments
: The primary stabilizers of the SC joint:
- Anterior Sternoclavicular Ligament : Thick, broad fibers coursing from the anterosuperior clavicle to the anterior manubrium. Resists anterior and superior displacement.
- Posterior Sternoclavicular Ligament : Thinner but stronger than the anterior ligament, extending from the posterosuperior clavicle to the posterior manubrium. It is the primary restraint against posterior displacement and thus critical in preventing mediastinal compromise.
- Interclavicular Ligament : Connects the superior aspects of the medial clavicles, crossing the superior aspect of the manubrial notch. Resists superior displacement of the clavicle and transmits forces between the two clavicles.
-
Costoclavicular Ligament (Rhomboid Ligament)
: This is arguably the most important primary stabilizer of the SC joint. It consists of anterior and posterior laminae, extending from the superior surface of the first rib and costal cartilage to the inferior surface of the medial clavicle. It restricts all clavicular movements except downward rotation and is critical in resisting superior, anterior, and posterior displacement.

- Muscular Relationships : The sternocleidomastoid muscle originates from the manubrium and medial clavicle, overlying the joint. The subclavius muscle lies inferior to the clavicle, offering some protection.
Biomechanics:
The SC joint permits movements in three planes:
1.
Elevation/Depression
: Approximately 35-45 degrees of elevation and 10 degrees of depression.
2.
Protraction/Retraction
: Approximately 35 degrees of combined movement.
3.
Axial Rotation
: Approximately 40-50 degrees of posterior rotation during full abduction.
The SC joint acts as a pivot, allowing the entire shoulder girdle to move relative to the trunk. The costoclavicular ligament serves as the fulcrum for clavicular rotation and translation. Injuries to this ligament significantly destabilize the joint, particularly against superior and posterior translation. The posterior sternoclavicular ligament is the main checkrein against posterior translation. Disruptions of these ligaments, especially the posterior sternoclavicular and costoclavicular ligaments, lead to the instability observed in dislocations. Understanding the sequential failure of these ligaments under specific load patterns is critical for appreciating the pathophysiology of dislocations.
Indications & Contraindications
The decision-making for managing SC joint dislocations hinges on the type of dislocation (anterior vs. posterior), stability, acuity, and patient factors.
Operative vs. Non-Operative Indications
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Posterior Dislocations | Absolute : Any evidence of mediastinal compromise (e.g., dyspnea, dysphagia, vascular compromise, neurological deficit). Relative : Irreducible closed reduction, recurrent instability, open dislocation, significant displacement causing pain/dysfunction. | Rare : Only for stable, minimally symptomatic, incomplete posterior subluxations without signs of mediastinal compromise, and when vigilant observation is feasible. |
| Anterior Dislocations | Relative : Failed closed reduction (especially in acute cases), recurrent symptomatic instability (after failed non-operative treatment), chronic painful dislocation (especially with impingement or functional limitations), open dislocation. | Primary Treatment : Acute, stable, reducible anterior dislocations without significant pain or functional deficit. Often managed with sling immobilization and activity modification. Chronic, asymptomatic anterior dislocations. |
| Other Considerations | Any dislocation : Open injury (infection risk), neurovascular compromise, severe pain/dysfunction limiting activities of daily living (ADLs), associated fractures impeding reduction or stability. | Any dislocation : Patient comorbidities precluding surgery, patient preference for non-operative management despite instability (if no life-threatening complications), stable subluxations. |
| Timing | Acute Posterior : Emergency/urgent surgical intervention. Acute Anterior : If reduction fails or is unstable, early surgical consideration. Chronic Symptomatic : Elective surgery following failed conservative care. | Acute Posterior : Not typically recommended unless extremely stable incomplete injury without compromise and under strict observation. Acute Anterior : Immediate. Chronic Asymptomatic : Often no intervention. |
Contraindications
Absolute Contraindications for Surgery
:
* Active local or systemic infection.
* Severe medical comorbidities that preclude safe anesthesia or surgery (e.g., uncontrolled cardiac disease, severe coagulopathy).
Relative Contraindications for Surgery
:
* Non-displaced or stable subluxations that are asymptomatic.
* Patient preference for non-operative management (in non-emergent cases).
* Prior surgery with significant scarring that increases surgical risk, making revision surgery challenging (though this may be an indication for a more complex approach rather than a contraindication to surgery itself).
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is essential for optimizing outcomes and mitigating risks, especially given the proximity to vital structures.
Pre-Operative Planning:
-
Imaging Review
:
- Radiographs : AP, lateral, and specialized SC joint views (e.g., serendipity view, Heinig view) can be helpful but are often limited by overlying structures.
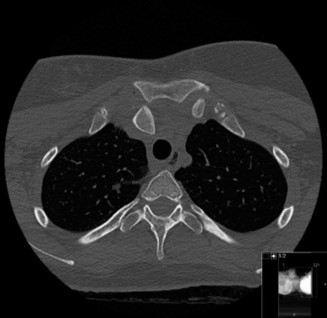
- Computed Tomography (CT) Scan : The gold standard for assessing SC joint dislocations. A high-resolution CT scan with 3D reconstructions provides detailed information on the direction and degree of displacement, articular congruity, and identifies associated fractures.
- CT Angiography (CTA) or Magnetic Resonance Angiography (MRA) : Mandatory for posterior dislocations to rule out mediastinal vascular injury (e.g., subclavian artery/vein, brachiocephalic artery) and delineate their relationship to the displaced clavicle.
- Magnetic Resonance Imaging (MRI) : Useful for evaluating soft tissue injury, including capsular and ligamentous structures (costoclavicular, sternoclavicular ligaments) and the articular disc, particularly in chronic cases or when internal derangement is suspected.
-
Consultations
:
- Thoracic Surgery/Vascular Surgery : Essential for posterior dislocations due to the high risk of mediastinal injury. Their presence should be mandatory in the operating room (OR) or immediately available.
- Anesthesia : To discuss potential challenges with airway management, especially if tracheal compression is present.
- Patient Education and Consent : Comprehensive discussion of risks, benefits, and alternatives, emphasizing the critical nature of posterior dislocations and potential for severe complications.
- Blood Products : Type and crossmatch, and have blood available, particularly for posterior dislocations where vascular injury is a significant risk.
- Operating Room Setup : Ensure appropriate retractors (e.g., vascular retractors, sternal spreaders), instrumentation for sternotomy or thoracotomy (if thoracic surgeons are involved), and vascular repair equipment are immediately available. Image intensifier for intraoperative fluoroscopy.
Patient Positioning:
- Anterior Dislocation : Typically supine on a standard operating table. A small bolster between the scapulae can facilitate reduction. The affected arm should be prepped and draped free to allow full range of motion for manipulative reduction.
-
Posterior Dislocation
:
- Supine Position : The patient is placed supine on the operating table.
- Shoulder Roll/Towel under Scapula : Crucial to allow the shoulder to fall posteriorly and inferiorly, facilitating initial closed reduction maneuvers and providing better exposure if open reduction is required.
- Arm Preparation : The entire arm on the affected side is prepped and draped free, allowing an assistant to manipulate the arm for reduction maneuvers (traction, abduction, extension).
- Chest Preparation : The entire anterior chest, neck, and shoulder should be prepped and draped, extending to the mid-axillary line to allow for potential extension of the incision or access for vascular/thoracic surgeons.
- Surgical Team Positioning : The primary surgeon typically stands on the affected side. An assistant for arm manipulation is essential.
- Consideration for Sternotomy : For complex posterior dislocations with definite or suspected vascular injury, the possibility of a median sternotomy should be anticipated, requiring appropriate surgical preparation and team presence.
Detailed Surgical Approach / Technique
Surgical intervention for SC joint dislocations aims to achieve anatomical reduction and stable fixation, prioritizing the safety of surrounding neurovascular structures, particularly in posterior dislocations.
Closed Reduction (Primarily for Posterior Dislocations)
Closed reduction should always be attempted first for acute posterior dislocations due provided no immediate hemodynamic instability related to mediastinal compression.
1.
Patient Positioning
: Supine with a bolster between the scapulae. Affected arm prepped and draped free.
2.
Anesthesia
: General anesthesia with muscle relaxation is typically required.
3.
Reduction Maneuver
:
* An assistant applies strong traction in line with the humerus, with the arm abducted to approximately 90-120 degrees and externally rotated.
* The surgeon simultaneously applies direct posterior pressure on the ipsilateral shoulder, pulling it posterolaterally to exaggerate the deformity and disengage the clavicle.
* While maintaining traction, the arm is then gently extended posteriorly, attempting to "lever" the medial clavicle back into place.
*
Towel Clip Technique
: If manual traction fails, a sterile towel clip can be used cautiously. It is placed under the medial clavicle (taking care to avoid vital structures) and used to gently lift the clavicle anteriorly while the arm is manipulated. This should be performed with extreme caution and only by experienced surgeons.
4.
Confirmation
: Post-reduction stability should be assessed. Intraoperative fluoroscopy (serendipity view) or portable chest X-ray can confirm reduction. A post-reduction CT scan is advisable to rule out subtle posterior displacement or associated injuries.
If closed reduction is unsuccessful or the joint is unstable after reduction, open reduction is indicated.
Open Reduction and Internal Fixation (ORIF)
Approach (General Principles):
- Incision : A curvilinear or transverse incision overlying the SC joint, parallel to Langer's lines for cosmesis. For posterior dislocations, a vertical incision over the joint or a "hockey stick" incision may offer better extensibility if vascular exposure or sternotomy is required.
-
Dissection
: Meticulous dissection is paramount.
- Incise skin and subcutaneous tissue.
- Identify and carefully divide the platysma muscle.
- Identify the anterior border of the sternocleidomastoid (SCM) muscle. The SCM can be partially released from its sternal head origin to improve exposure, particularly for posterior dislocations.
- Cautiously incise the periosteum over the medial clavicle and manubrium.
-
For Posterior Dislocations
: Great care must be taken when dissecting posteriorly. The posterior capsule and associated ligaments are usually torn. The subclavian vessels, brachial plexus, trachea, and esophagus lie directly posterior to the joint. Vascular/thoracic surgery backup is crucial.
- Dissect along the superior border of the medial clavicle.
- Identify the anterior SC ligaments and capsule, which are often torn.
- Identify the costoclavicular ligament.
- Gently use a blunt instrument (e.g., Freer elevator) to explore the posterior aspect of the clavicle to ensure no soft tissue interposition prevents reduction.
Reduction:
- Anterior Dislocation : Often reduced easily once tissues are cleared. Direct pressure on the medial clavicle while an assistant manipulates the arm can reduce it.
- Posterior Dislocation : Manual traction and manipulation of the arm (as in closed reduction) are usually performed while the surgeon directly guides the clavicle into its anatomical position using blunt instruments. In cases of irreducible dislocations, incarcerated soft tissue (e.g., articular disc, SCM fibers) may need to be excised or released.
Stabilization/Fixation:
Historically, K-wires were used for fixation but are associated with a high complication rate (e.g., pin migration into mediastinum, heart, great vessels) and are generally
contraindicated
. Current techniques focus on soft tissue reconstruction and augmentation.
-
Ligament Repair/Reconstruction
:
- Primary Repair : If the anterior/posterior sternoclavicular ligaments and costoclavicular ligament complex are acutely torn and of good quality, they can be directly repaired with strong, non-absorbable sutures (e.g., FiberWire, braided polyester). Anchor sutures can be placed into the sternum and clavicle.
-
Reconstruction (Autograft/Allograft)
: For chronic dislocations, comminuted ligament tears, or when primary repair is deemed insufficient, reconstruction using a graft is preferred.
- Autografts : Palmaris longus, semitendinosus, gracilis, or pectoralis minor tendon can be harvested.
- Allografts : Achilles tendon, tibialis anterior, or semitendinosus allografts are common.
- Technique : The graft is typically passed through drill holes or tunnels created in the medial clavicle and manubrium, recreating the anatomical course of the costoclavicular ligament and/or the posterior sternoclavicular ligament. The graft is then tensioned and secured with sutures or interference screws. Some techniques involve figure-of-eight or double-bundle configurations.
- Capsular Reinforcement : The remaining capsule should be repaired and reinforced with strong sutures if possible.
- Internal Bracing : Some surgeons advocate for internal bracing techniques using high-strength suture tape augmentation to protect the repair/reconstruction, particularly in high-demand patients.
- Plate Fixation : While rarely used due to challenges with contouring and stress shielding, some low-profile locking plates have been described for specific scenarios of sternal-clavicular junction fractures or highly unstable chronic dislocations. This is an advanced technique with potential for hardware-related complications.
- Pectoralis Major/Minor Transfer : For chronic anterior instability, a portion of the pectoralis major tendon can be transferred to reinforce the anterior joint capsule.
- Medial Clavicle Excision (for Chronic Painful Anterior Dislocation) : In select cases of chronic, painful, irreducible anterior dislocations, particularly in older, lower-demand patients where reconstruction has failed or is contraindicated, medial clavicle excision (Mumford procedure) can be considered. This typically involves removing 1-2 cm of the medial clavicle. This procedure alters the biomechanics significantly and is reserved for specific indications.
Wound Closure:
- The SCM muscle is repaired if it was released.
- Platysma and subcutaneous tissues are closed meticulously.
- Skin closure.
Key Considerations for Posterior Dislocations:
- Mediastinal Protection : Constant vigilance for mediastinal structures. A finger or blunt retractor can be placed posteriorly to protect these structures during reduction and fixation, particularly during drilling.
- Vascular Injury : If vascular injury is encountered or suspected, vascular surgery must manage it.
- Airway Management : If tracheal compression is a concern, consider an awake fiberoptic intubation or a tracheostomy tray readily available.
Complications & Management
SC joint dislocations, particularly posterior ones, carry a significant risk of complications, both acute and chronic. Proactive management and a thorough understanding of potential issues are critical for optimal patient care.
Common Complications and Management
| Complication | Incidence | Description & Etiology | Management & Salvage Strategies |
|---|---|---|---|
| Recurrence / Instability | Variable (up to 50% for anterior, less for posterior post-ORIF) | Most common after non-operative management of anterior dislocations or inadequate fixation/repair. Can be painful and limit function. | Non-operative : Re-immobilization, physical therapy for periscapular strengthening. Operative : Revision stabilization using stronger autograft/allograft reconstruction, internal bracing, or pectoralis major transfer. For chronic anterior instability, medial clavicle excision might be considered in low-demand patients, though with inherent biomechanical compromise. For posterior, revision reconstruction is the gold standard. |
| Pain (Chronic) | Common | Persistent pain, often exacerbated by movement, due to unreduced displacement, instability, arthritis, hardware irritation, or nerve entrapment. | Conservative : NSAIDs, physical therapy, corticosteroid injections. Surgical : If due to instability, address instability as above. If due to hardware, removal of symptomatic hardware. If due to degenerative changes in a chronic painful anterior dislocation, medial clavicle excision can provide relief. |
| Neurovascular Injury | High for posterior dislocations | Vascular : Injury to subclavian artery/vein, brachiocephalic vessels, carotid artery. Can lead to hemorrhage, pseudoaneurysm, thrombosis. Neurological : Brachial plexus injury (stretch or direct trauma), phrenic nerve palsy. | Acute : Immediate surgical exploration (often with vascular surgeon) and repair of injured vessels. Hemostasis. Chronic : Management of sequelae (e.g., pseudoaneurysm repair, nerve grafting/neurolysis, management of Horner's syndrome if sympathetic chain affected). Pre-operative CTA/MRA is crucial to identify potential injuries. |
| Airway Compromise | Significant for posterior dislocations | Tracheal compression, especially in posterior dislocations, leading to dyspnea, stridor, or even respiratory arrest. Esophageal compression can cause dysphagia. | Acute : Urgent reduction (closed or open). Tracheal intubation may be required. Emergency tracheostomy may be indicated in severe cases. Thoracic/vascular surgery consultation is essential. |
| Infection | Low (1-5%) | Superficial wound infection or deep joint infection. More common with open injuries or prolonged surgical times. | Superficial : Oral antibiotics, local wound care. Deep : Surgical debridement, intravenous antibiotics based on culture, hardware removal (if applicable and joint stable), irrigation, and possibly negative pressure wound therapy. For severe cases, debridement and delayed reconstruction may be necessary. |
| Hardware-Related Complications | Variable | K-wire migration : (Historically, but still relevant if used) life-threatening migration into mediastinal structures (heart, great vessels, trachea). Suture/Graft failure : Rarity of rupture, but can lead to recurrent instability. Plate irritation : Prominence, pain. | K-wire migration : Immediate surgical removal, often requiring cardiothoracic/vascular surgery. Suture/Graft failure : Revision surgery with stronger reconstruction. Plate irritation : Symptomatic hardware removal after adequate healing (typically 6-12 months). |
| Non-Union / Malunion | Rare at SC joint | More common with associated medial clavicle fractures or if reduction is not anatomical, leading to persistent pain, deformity, or restricted motion. | Non-union : Excision of fibrous tissue, bone grafting, and internal fixation/reconstruction. Malunion : Corrective osteotomy or medial clavicle excision in symptomatic cases. |
| Arthrosis / Degenerative Changes | Common in long-term | Post-traumatic arthritis due to articular cartilage damage, chronic instability, or altered biomechanics. Leads to chronic pain and stiffness. | Conservative : NSAIDs, physical therapy, intra-articular injections. Surgical : For severe, debilitating symptoms, medial clavicle excision (arthroplasty) can be considered, especially in older, low-demand patients. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for restoring function, preventing stiffness, and protecting the surgical repair. Protocols vary based on the type of injury, surgical technique, and surgeon preference, but generally follow a phased approach focused on gradual progression.
Phase I: Immediate Post-Operative (Weeks 0-6)
- Goals : Pain and swelling control, protect the repair, maintain distal joint mobility.
-
Immobilization
:
- Anterior Dislocations : Sling immobilization for 3-4 weeks. May allow gentle pendulum exercises.
- Posterior Dislocations (after ORIF) : Sling immobilization for 4-6 weeks to protect the soft tissue reconstruction. No active shoulder flexion/abduction above 45-60 degrees.
- Pain Management : NSAIDs, analgesics.
-
Activity
:
- Avoid any direct pressure on the SC joint.
- No lifting, pushing, or pulling with the affected arm.
- Encourage active range of motion (AROM) of the elbow, wrist, and hand.
- Gentle pendulum exercises for the shoulder (if allowed by surgeon for anterior dislocations).
- Maintain good posture.
- Precautions : Avoid any movements that cause pain or stress the SC joint. No overhead activities.
Phase II: Early Motion & Gradual Strengthening (Weeks 6-12)
- Goals : Gradually restore full passive range of motion (PROM), initiate active range of motion (AROM), begin light strengthening.
-
Mobilization
:
- Discontinue sling as tolerated.
- Begin gentle PROM for shoulder flexion, abduction, and rotation, progressing slowly to AROM.
- Crucial for posterior repairs : Limit elevation and abduction to 90 degrees initially.
- Gentle scapular stabilization exercises (e.g., scapular retractions, protractions).
-
Strengthening
:
- Isometric exercises for the shoulder girdle muscles (rotator cuff, deltoid) with the arm at the side.
- Theraband exercises with low resistance.
- Focus on posture and scapular control.
- Precautions : Avoid heavy lifting, sudden movements, or activities that place direct stress on the SC joint. No overhead activities against resistance.
Phase III: Progressive Strengthening & Functional Return (Weeks 12-24)
- Goals : Restore full strength, power, and endurance; prepare for return to sport/activity.
-
Strengthening
:
- Progressive resistive exercises for all shoulder girdle muscles, including eccentric and concentric training.
- Focus on functional movements relevant to the patient's occupation or sport.
- Incorporate core stability exercises.
- Neuromuscular Control : Proprioceptive training, balance exercises.
-
Activity
:
- Gradual return to light daily activities.
-
Sport-specific drills and plyometric exercises (if applicable) can be initiated cautiously.

- Precautions : Continue to avoid contact sports or activities with high risk of re-injury until full recovery and clearance by the surgeon.
Phase IV: Return to Sport / Activity (Month 6+)
- Goals : Full return to unrestricted activities, including contact sports.
-
Criteria for Return to Sport
:
- Full, pain-free range of motion.
- Symmetry in strength (at least 90-95% compared to contralateral side).
- Absence of pain or instability during functional activities.
- Completion of sport-specific training.
- Surgeon's clearance based on clinical examination and patient confidence.
- Considerations : For high-demand athletes, return to contact sports may be delayed until 6-9 months or even longer, especially after complex reconstructions for posterior dislocations.
Summary of Key Literature / Guidelines
The management of sternoclavicular joint dislocations has evolved, moving away from problematic hardware toward biologically based soft tissue reconstruction. Due to the rarity of these injuries, high-level evidence from randomized controlled trials is scarce, and much of the current understanding is derived from case series, expert opinion, and biomechanical studies.
Key Insights from the Literature:
- Posterior Dislocations: Always a Priority : There is a universal consensus on the urgent nature of acute posterior dislocations due to the risk of mediastinal compromise. Early closed reduction is the initial treatment of choice. If unsuccessful or unstable, open reduction and stabilization are warranted, often with multidisciplinary involvement (vascular/thoracic surgery).
- K-wires are Contraindicated : The historical use of K-wires for SC joint fixation has been largely abandoned due due to well-documented, potentially catastrophic migration into vital mediastinal structures.
- Soft Tissue Reconstruction for Stability : Current surgical trends favor anatomical or near-anatomical reconstruction of the sternoclavicular and costoclavicular ligaments using autografts or allografts. Techniques often involve drilling tunnels in the clavicle and sternum to secure the graft in a figure-of-eight or double-bundle fashion. The aim is to restore the native biomechanics and provide robust stability.
- Anterior Dislocations: Conservative First : For acute, reducible, and stable anterior dislocations, non-operative management (sling immobilization and gradual rehabilitation) remains the initial treatment. Surgical intervention is typically reserved for symptomatic chronic instability, failed conservative management, or irreducible acute dislocations.
- Chronic Painful Anterior Dislocations : Medial clavicle excision (Mumford procedure) is a viable option for select older, lower-demand patients with chronic painful anterior dislocations where conservative measures and potentially reconstruction have failed. However, this alters joint mechanics and should be considered judiciously.
- Imaging Modalities : CT scans with 3D reconstructions are considered the gold standard for diagnosis and pre-operative planning, especially to determine the direction and degree of displacement. CTA is indispensable for posterior dislocations to rule out vascular involvement.
- Long-Term Outcomes : While surgical intervention for posterior dislocations generally yields good to excellent functional outcomes, the potential for long-term arthrosis and recurrence, particularly for anterior dislocations, remains a concern. Patient satisfaction is often tied to pain control and functional restoration.
-
Controversies and Future Directions
:
- Optimal Graft Choice : While various autografts and allografts are used, a definitive "best" graft material or technique has not been established.
- Role of Plates : Low-profile locking plates offer rigid fixation but their role in primary SC joint dislocations is limited due to contouring challenges, potential for hardware prominence, and stress shielding. They may be considered for specific fracture-dislocation patterns.
- Internal Bracing : The utility of augmenting soft tissue repairs with internal bracing (suture tape) is an evolving area, with promising early results in other joint instability surgeries.
- Biologic Augmentation : Future research may explore the use of growth factors or stem cells to enhance ligament healing and reconstruction.
In conclusion, the successful management of SC joint dislocations requires a thorough understanding of surgical anatomy, meticulous pre-operative planning, precise surgical technique focusing on biological reconstruction, and a well-structured post-operative rehabilitation program. Vigilance for complications, particularly neurovascular compromise in posterior dislocations, is paramount.
