Introduction & Epidemiology
Pectoralis major muscle injuries, particularly complete ruptures, represent a significant, albeit relatively uncommon, pathology predominantly affecting active males during their second to fourth decades of life. Once considered rare, the incidence of these injuries has increased with the growing participation in resistance training, particularly the bench press exercise, and contact sports. These injuries typically involve a sudden, forceful eccentric contraction of the pectoralis major muscle while the shoulder is in abduction and external rotation, followed by a powerful adduction and internal rotation movement. This mechanism places extreme tension on the musculotendinous unit, leading to failure.
Clinical presentation typically involves acute pain, a palpable defect, ecchymosis extending down the arm and across the chest, and significant weakness in shoulder adduction and internal rotation. Early diagnosis is critical, as acute surgical repair within the first few weeks offers superior functional and cosmetic outcomes compared to delayed or chronic reconstructions.
Ruptures are commonly classified by their anatomical location:
*
Humeral insertion:
Most common site of complete rupture (60-80%).
*
Musculotendinous junction:
Approximately 10-20%.
*
Muscle belly:
Less common, typically due to direct trauma or severe eccentric load.
*
Origin (sternal or clavicular):
Rare.
Partial tears are also observed, with their management often dictated by the percentage of tendon involvement, patient symptoms, and functional demands. The increasing understanding of the pectoralis major's complex anatomy and biomechanics has refined diagnostic and treatment algorithms, emphasizing early intervention for appropriate candidates.
Surgical Anatomy & Biomechanics
A thorough understanding of the pectoralis major's surgical anatomy and biomechanics is paramount for effective diagnosis and successful repair.
Anatomy
The pectoralis major is a broad, fan-shaped muscle comprising two distinct heads:
1.
Clavicular Head:
Originates from the anterior surface of the medial half of the clavicle.
2.
Sternocostal Head:
Originates from the anterior surface of the sternum, the superior six costal cartilages, and the aponeurosis of the external oblique muscle.
These two heads converge to form a flattened tendon that inserts into the lateral lip of the bicipital groove of the humerus. A critical anatomical feature is the bilaminar and twisted nature of its insertion . The fibers of the sternocostal head insert more inferiorly and posteriorly on the humerus, effectively twisting beneath the clavicular head fibers which insert more superiorly and anteriorly. This unique arrangement optimizes its mechanical advantage for adduction and internal rotation across a wide range of shoulder positions.
- Innervation: The pectoralis major is innervated by both the medial pectoral nerve (C8, T1) and the lateral pectoral nerve (C5, C6, C7), branches of the brachial plexus. The lateral pectoral nerve primarily innervates the clavicular head, while the medial pectoral nerve supplies both heads, predominantly the sternocostal head. These nerves pierce the clavipectoral fascia.
- Blood Supply: The primary arterial supply is the pectoral branch of the thoracoacromial artery , which arises from the second part of the axillary artery. Additional supply comes from perforating branches of the internal thoracic artery.
- Relationships: The pectoralis major forms the anterior wall of the axilla. Deep to it lies the pectoralis minor, separated by the clavipectoral fascia. The cephalic vein runs in the deltopectoral groove, providing a useful landmark for surgical approach.
Biomechanics
The pectoralis major is a powerful muscle responsible for:
*
Shoulder Adduction:
Bringing the arm towards the midline.
*
Shoulder Internal Rotation:
Rotating the arm medially.
*
Shoulder Flexion:
Primarily the clavicular head, assisting in elevating the arm.
The unique twisted insertion contributes significantly to its functional versatility. When the arm is abducted and externally rotated, this twisted configuration becomes untwisted and taut, rendering the tendon highly vulnerable to rupture, especially during powerful eccentric contractions. This is classically seen in the "bottom" position of a bench press, where the muscle is maximally stretched while attempting to resist a downward force. The sternal head, due to its longer fibers and more posterior insertion, is often implicated in complete ruptures.
Understanding the typical rupture pattern – often an avulsion from the humeral insertion – dictates the surgical strategy, focusing on robust reattachment to the bicipital groove. The extent of muscle retraction depends on the location of the tear and the integrity of the surrounding fascia.
Indications & Contraindications
The decision for operative versus non-operative management of pectoralis major ruptures is based on several factors, including the type of injury, patient's activity level, functional demands, age, and comorbidities.
Indications for Operative Management
- Acute Complete Ruptures: In active individuals, athletes, or those engaged in manual labor, surgical repair within 3-6 weeks of injury is generally recommended. This approach aims to restore strength, minimize functional deficits, and improve cosmesis.
- Partial Ruptures >50% Cross-Sectional Area: For symptomatic patients with significant disruption of the tendon or muscle, particularly if conservative management fails.
- Chronic Ruptures in Symptomatic, Active Individuals: While outcomes are diminished compared to acute repairs, reconstruction (often with graft augmentation) may be considered to improve strength, function, and aesthetics. This decision is made on a case-by-case basis, balancing potential benefits against the challenges of scar tissue, muscle atrophy, and retraction.
- Functional Instability or Significant Weakness: If non-operative management of any tear type leads to unacceptable functional deficits.
Indications for Non-Operative Management
- Partial Tears (<50% Cross-Sectional Area): Especially in low-demand individuals, elderly, or those with minimal symptoms.
- Complete Tears in Sedentary or Elderly Patients: Individuals with low functional demands or significant medical comorbidities precluding surgery may opt for conservative management.
- Contraindications to Surgery: As listed below.
Contraindications
-
Absolute Contraindications:
- Active infection (local or systemic).
- Severe medical comorbidities that prohibit safe anesthesia and surgical intervention.
-
Relative Contraindications:
- Chronic ruptures (>6-12 months post-injury) with extensive muscle atrophy, fatty degeneration, severe retraction, and significant scarring. While not an absolute contraindication, the complexity and prognosis for full recovery are significantly reduced, often necessitating complex reconstructive techniques with allografts or autografts.
- Unrealistic patient expectations regarding functional recovery or cosmetic outcome, particularly in chronic cases.
- Patients unwilling or unable to adhere to a strict post-operative rehabilitation protocol.
Operative vs. Non-Operative Indications
| Feature | Operative Indications | Non-Operative Indications |
|---|---|---|
| Injury Type | Acute complete rupture | Acute partial rupture (<50% cross-sectional involvement) |
| Symptomatic partial rupture (>50% cross-sectional involvement) | Atraumatic pectoralis strain or minor contusion | |
| Patient Demands | Active individuals, competitive athletes, manual laborers | Sedentary individuals, low-demand patients, elderly |
| Timing of Injury | Acute (<3-6 weeks from injury) for direct repair | Chronic rupture with minimal symptoms or extensive retraction/atrophy, poor tissue quality |
| Chronic rupture in select active patients (reconstruction) | ||
| Functional Goal | Restoration of strength, endurance, cosmesis, full function | Pain control, maintenance of baseline function, activities of daily living |
| Medical Status | Medically fit for general anesthesia and surgery | Significant medical comorbidities precluding surgery |
| Imaging Findings | Complete avulsion from humerus, significant retraction, musculotendinous junction tears | Minor fiber disruption, intramuscle hematoma |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential for a successful pectoralis major repair, involving comprehensive patient evaluation, detailed imaging review, and precise intra-operative setup.
Pre-Operative Evaluation
- History and Physical Examination: Confirm the diagnosis, assess the timing of injury, patient's functional demands, and identify any associated shoulder pathology. Key findings include ecchymosis, a palpable defect (especially with active adduction), pain with resisted adduction and internal rotation, and often a visible asymmetry or contour deformity.
-
Imaging:
- MRI (Magnetic Resonance Imaging): The gold standard. MRI precisely identifies the location of rupture (humeral avulsion, musculotendinous, muscle belly), extent of retraction, degree of muscle degeneration (fatty infiltration in chronic cases), and associated injuries. It also helps differentiate partial from complete tears.
- Ultrasound: Can be a useful dynamic tool in experienced hands for acute tears to assess the rupture site and retraction, though it is operator-dependent.
- Radiographs: Primarily to rule out concomitant osseous injuries or avulsion fractures, though these are rare.

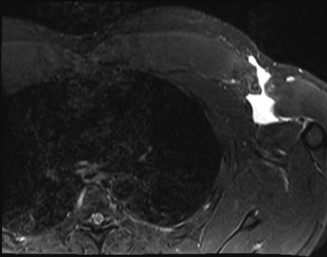
A pre-operative MRI axial view demonstrating a complete pectoralis major tendon avulsion from the humeral insertion (white arrow) with significant retraction. -
Medical Clearance: Standard pre-operative assessment for general anesthesia, including blood work, ECG, and consultation with internal medicine or cardiology as needed.
- Informed Consent: Discuss the surgical procedure, potential risks (infection, nerve injury, re-rupture, stiffness, cosmetic deformity), expected recovery course, and alternative treatments.
Anesthesia
General anesthesia is typically employed. A regional interscalene brachial plexus block can be a valuable adjunct for post-operative pain management, though it must be carefully weighed against the risk of obscuring neurologic deficits.
Patient Positioning
- Supine Position: The patient is positioned supine on the operating table. This allows for excellent access to the anterior chest and proximal arm.
- Arm Positioning: The ipsilateral arm is often prepped and draped free on a sterile hand table or an adjustable arm board. This allows for intra-operative manipulation of the shoulder, which is critical for tensioning the repair and assessing range of motion. The arm should be able to move freely from full abduction and external rotation to full adduction and internal rotation.
- Torso Positioning: The torso can be slightly elevated to a semi-Fowler position or placed in a "beach chair" position, though a flat supine position is often preferred for optimal exposure and stability.
- Padding and Strapping: Ensure adequate padding for all bony prominences (heels, sacrum, ulnar nerve at the elbow) and safety straps over the hips and knees to prevent inadvertent movement.
- Tourniquet: A pneumatic tourniquet may be applied high on the ipsilateral arm for regional ischemia, although many surgeons prefer to operate without a tourniquet to maintain muscle viability and assess perfusion, relying on meticulous hemostasis.
Detailed Surgical Approach / Technique
The goal of surgical repair is to anatomically reattach the ruptured pectoralis major tendon to its humeral insertion with appropriate tension, restoring strength and contour. The technique varies slightly depending on the tear location and chronicity.
Incision
A curvilinear incision is made in the deltopectoral groove, typically extending from the anterior axillary fold proximally towards the mid-clavicle, or distally towards the deltoid insertion. This allows for extensile exposure of both the humeral insertion site and the retracted muscle belly. The incision should be planned to optimize cosmetic outcome while providing sufficient access.
Dissection & Internervous Planes
- Skin and Subcutaneous Tissue: Carefully incise the skin and subcutaneous fat. Meticulous hemostasis is maintained.
- Deltopectoral Interval: Identify the interval between the deltoid (laterally) and the pectoralis major (medially). The cephalic vein typically runs in this groove. Efforts should be made to preserve the cephalic vein, retracting it laterally with the deltoid. If necessary for exposure, it can be ligated, though this may increase post-operative swelling.
- Hematoma and Scar Tissue: In acute injuries, a significant hematoma will be encountered. This is evacuated. In chronic injuries, dense scar tissue will need to be carefully dissected to mobilize the muscle belly.
- Locate Ruptured Tendon/Muscle Belly: The ruptured tendon stump is typically retracted medially and inferiorly. The sternocostal head often retracts further than the clavicular head due to its longer fiber length and often more extensive involvement in the tear. Identify the distinct borders of the muscle and its retracted tendon.
- Mobilization: The muscle belly must be adequately mobilized to allow for tension-free repair to the humerus. This often involves releasing adhesions from the chest wall and underlying structures. Care must be taken to avoid injury to the medial and lateral pectoral nerves entering the deep surface of the muscle.
Reduction & Fixation
A. Acute Repair (Humeral Avulsion)
This is the most common scenario and offers the best outcomes.
1.
Prepare Humeral Footprint:
The original insertion site on the lateral lip of the bicipital groove is identified. Any remaining tendon remnants are debrided, and the bone is decorticated with a burr or osteotome to expose cancellous bone and promote healing.
2.
Suture Passage through Tendon:
Strong, non-absorbable sutures are passed through the avulsed tendon stump. Commonly used techniques include:
*
Modified Krackow Stitch:
Provides a robust grip on the tendon fibers, resisting pull-out.
*
Locking Loop Suture:
Similar benefits to Krackow.
* Usually 4-6 strands of robust suture (e.g., #2 FiberWire or similar) are used to create a strong tendon-suture construct.
* The sutures are placed in a staggered fashion, often through both the superior and inferior aspects of the tendon to capture the bilaminar structure effectively.
3.
Anchor Placement:
Suture anchors (biocomposite or PEEK) are placed in the prepared humeral footprint. Typically, 2-4 anchors are used, often in a single-row or double-row configuration to maximize the contact area and provide strong fixation.
*
Single-Row:
Anchors are placed along the bicipital groove.
*
Double-Row (Suture Bridge):
A row of anchors is placed more medially, and a second row more laterally, with the sutures from the first row passed over the tendon and tied to the second row. This technique aims to provide a broader compression of the tendon to the bone, theoretically improving healing.
4.
Tensioning and Fixation:
The arm is placed in a position of 0-30 degrees of abduction and slight internal rotation to achieve appropriate tension. The sutures are then sequentially tied, ensuring firm compression of the tendon to the humerus. The tension should be sufficient to prevent gapping but not so tight as to risk strangulation or subsequent re-rupture with motion. The repair is tested gently through a full range of motion.
``
*Intra-operative photograph showing a repaired pectoralis major tendon (blue arrow) reattached to the humerus using multiple suture anchors (black arrows) at the bicipital groove.*
B. Acute Repair (Musculotendinous Junction or Muscle Belly)
- Direct Repair: Strong non-absorbable sutures (e.g., #2 FiberWire) are used in a locking loop or modified Krackow fashion to directly approximate the torn muscle or musculotendinous junction.
- Augmentation: If the tissue quality is poor or the tear is extensive, augmentation with a biological graft (e.g., acellular dermal matrix, Achilles tendon allograft) or synthetic mesh may be considered to reinforce the repair.
C. Chronic Repair/Reconstruction
Chronic tears (typically >6-8 weeks) present significant challenges due to muscle retraction, atrophy, fatty degeneration, and dense scarring.
1.
Extensive Mobilization:
This is the most crucial step. Adhesions are released from the chest wall, pectoralis minor, and surrounding structures to mobilize the muscle belly laterally. Neurovascular structures must be carefully protected.
2.
Direct Repair (Rare):
Only possible if the muscle can be mobilized to allow for tension-free reattachment.
3.
Allograft/Autograft Reconstruction:
More commonly required.
*
Graft Choice:
Achilles tendon allograft (with calcaneal bone block), semitendinosus allograft/autograft, or other suitable tendons.
*
Preparation:
The graft is prepared ex-vivo. For Achilles, the bone block is shaped to fit into a bone tunnel or trough in the humerus, or fixed with a screw.
*
Attachment to Humerus:
The distal end of the graft is fixed to the humeral insertion site using either a bone tunnel technique (bone block secured with interference screw) or suture anchors.
*
Weaving into Muscle Stump:
The proximal end of the graft is then woven into the retracted pectoralis major muscle stump using multiple robust whipstitches (e.g., Krackow technique). The repair is tensioned with the arm in slight abduction and internal rotation.
*
Tensioning:
Achieving appropriate tension is critical but challenging in chronic cases. Over-tensioning can lead to re-rupture, while under-tensioning results in persistent weakness.
Layered Closure
After confirming adequate hemostasis, the wound is closed in layers:
* Deep fascia (if disrupted)
* Subcutaneous tissue
* Skin (with absorbable sutures or staples)
A drain may be placed, especially in larger or chronic cases, to prevent hematoma/seroma formation. A sterile dressing is applied, and the arm is placed in a sling or brace as per post-operative protocol.
Complications & Management
While pectoralis major repair generally has good outcomes, a range of complications can occur. Vigilance and appropriate management are essential.
| Complication | Incidence (Approximate) | Management / Salvage Strategy |
|---|---|---|
| Re-rupture | 2-5% | Acute: Revision repair, often with careful assessment of tissue quality and potential augmentation (e.g., biologic graft). Chronic: Reconstruction using allograft or autograft, addressing underlying factors like inadequate tension or poor initial fixation. |
| Infection | <1% (superficial) | Superficial: Oral antibiotics, local wound care. Deep: Surgical debridement, intravenous antibiotics, removal of hardware/graft if involved, and delayed reconstruction if necessary after infection clearance. |
| Adhesions / Stiffness | Variable (10-20%) | Aggressive physical therapy, stretching, modalities. Manipulation Under Anesthesia (MUA) for persistent stiffness after 3-6 months. Rarely, surgical arthrolysis or release of adhesions may be considered. |
| Nerve Injury | Rare (<0.5%) | Pectoral Nerves: Usually neuropraxia. Observe, electrodiagnostic studies (EMG/NCS) if no improvement. Brachial Plexus (Interscalene Block): Transient deficits, usually resolve. Persistent deficits may warrant neurology consult or exploration. |
| Hematoma / Seroma | 2-10% | Observation, aspiration if symptomatic or large. Compression dressing. Surgical drainage may be required for large, expanding hematomas or those resistant to aspiration. |
| Cosmetic Deformity | Variable (5-15%) | Patient education and counseling pre-operatively. For significant persistent contour defects, revision surgery may be considered, but often difficult and may involve fat grafting or tissue reconstruction. |
| Persistent Pain | Variable | Pharmacological management (NSAIDs, analgesics), physical therapy. Rule out other etiologies (e.g., nerve irritation, shoulder pathology). Pain due to hardware may require anchor removal. |
| Weakness / Fatigue | Variable | Continued physical therapy focusing on strengthening. For significant, persistent weakness post-rehab, consider further imaging (MRI) to assess integrity of repair. May necessitate revision if re-rupture is identified. |
| Heterotopic Ossification | Rare | Prophylaxis in high-risk patients (e.g., post-traumatic brain injury, prior HO) with NSAIDs or radiation. Excision if mature and symptomatic, but recurrence is possible. |
| Anchor Pull-out / Failure | Rare | Revision surgery with larger or additional anchors, or conversion to a different fixation strategy (e.g., bone tunnels). |
Preventive Strategies:
*
Aseptic Technique:
Strict adherence to surgical sterility protocols to minimize infection risk.
*
Meticulous Hemostasis:
Thorough coagulation and optional drain placement to reduce hematoma/seroma formation.
*
Appropriate Tensioning:
Balancing anatomical reduction with tension-free repair to prevent gapping or excessive stress on the repair.
*
Robust Fixation:
Utilizing strong suture constructs and adequate numbers of suture anchors to withstand early mobilization forces.
*
Neurovascular Protection:
Careful dissection and identification of vital structures, especially pectoral nerves and axillary vessels.
*
Early, Protected Rehabilitation:
Adherence to a structured post-operative protocol to prevent stiffness while protecting the repair.
Post-Operative Rehabilitation Protocols
A carefully structured and progressive post-operative rehabilitation protocol is critical for optimizing outcomes following pectoralis major repair. The protocol aims to protect the repair while gradually restoring range of motion, strength, and function. Close communication between the surgeon and physical therapist is paramount.
Phase I: Protection (Weeks 0-6)
- Goals: Protect the surgical repair, minimize pain and inflammation, prevent stiffness in uninvolved joints.
-
Immobilization:
- Arm placed in a sling or abduction brace with the shoulder adducted and internally rotated. Duration varies (typically 3-6 weeks) based on surgeon preference, repair integrity, and patient compliance.
-
Motion:
- Passive Range of Motion (PROM): Gentle, pain-free PROM for the shoulder within a protected range (e.g., flexion to 90 degrees, external rotation to 0 degrees or neutral, avoiding abduction beyond 45 degrees, and strict avoidance of active adduction, internal rotation, and extension ). Scapular mobilization and pendulum exercises.
- Elbow, Wrist, Hand: Active range of motion (AROM) exercises to prevent stiffness and maintain circulation.
-
Activities:
- No active contraction of the pectoralis major.
- No lifting, pushing, pulling with the affected arm.
- Avoidance of strenuous activities.
- Pain & Swelling Management: Ice, NSAIDs, appropriate analgesics.
Phase II: Controlled Motion & Early Strengthening (Weeks 6-12)
- Goals: Gradually increase shoulder range of motion, initiate gentle isometric strengthening, improve neuromuscular control.
-
Immobilization:
- Sling weaned off, typically by week 6-8, as tolerated.
-
Motion:
- Assisted Active Range of Motion (AAROM): Progressing to full AROM for shoulder flexion, abduction, and external rotation as pain allows.
- Continue with PROM if AROM is limited.
- Gentle pectoralis major stretching within pain limits, avoiding aggressive or ballistic stretches.
-
Strengthening:
- Isometric Exercises: Light, pain-free isometrics for rotator cuff muscles (external rotation, internal rotation), deltoid, biceps, and triceps. Strict avoidance of isometric pectoralis major contraction (e.g., resisted adduction) for the initial part of this phase.
- Scapular stabilization exercises.
-
Activities:
- Light activities of daily living (ADLs) are permissible.
- No heavy lifting, pushing, or pulling.
Phase III: Progressive Strengthening (Weeks 12-24)
- Goals: Restore full pain-free range of motion, progressively increase strength and endurance, prepare for functional activities.
-
Motion:
- Achieve full, pain-free AROM in all planes.
-
Strengthening:
- Progressive Resistance Exercises (PREs): Gradually introduce light resistance for all shoulder girdle muscles, including controlled, low-load exercises for the pectoralis major (e.g., light cable adduction, dumbbell flyes with limited range).
- Focus on eccentric control and concentric strength.
- Core strengthening and postural exercises.
-
Activities:
- Return to light work duties (non-manual).
- Avoidance of heavy lifting, contact sports, or activities that place high stress on the pectoralis major.
- Introduction of light, controlled functional movements.
Phase IV: Return to Activity/Sport (Weeks 24+)
- Goals: Achieve maximal functional strength and endurance, gradually return to sport-specific activities, prevent re-injury.
-
Strengthening:
- Advanced PREs, sport-specific drills, plyometrics, and power training for the shoulder girdle and core.
- Gradual increase in load and intensity for pectoralis major exercises.
- Emphasis on proper lifting mechanics and technique.
-
Return to Sport:
- A gradual, supervised return to full activity or contact sports is initiated, typically at 6 months post-surgery, but often closer to 9-12 months for high-demand athletes. This decision is based on objective strength measures (e.g., isokinetic testing), functional testing, and clinical assessment of pain and stability.
- Patient education on avoiding high-risk movements (e.g., maximal bench press with wide grip, deep eccentric loading) during initial return.
Key Considerations:
*
Individualization:
Protocols must be individualized based on the patient's age, injury severity, repair quality, and functional goals.
*
Pain-Guided Progression:
Progression should always be pain-free and guided by the patient's tolerance.
*
Compliance:
Patient adherence to the protocol is crucial for successful outcomes.
*
Surgeon Oversight:
Regular follow-up appointments to monitor progress and address any concerns.
Summary of Key Literature / Guidelines
The understanding and management of pectoralis major ruptures have evolved significantly, with robust literature supporting modern surgical techniques and rehabilitation protocols.
-
Early Surgical Repair for Complete Tears: There is a strong consensus in the orthopedic literature that acute complete tears of the pectoralis major, particularly those involving the humeral insertion in active individuals, should be surgically repaired. Studies consistently demonstrate superior outcomes in terms of strength, endurance, return to sport, and cosmetic appearance with early repair compared to non-operative management or delayed reconstruction.
- Schepsis et al. (2006) provided a comprehensive review highlighting the success of surgical repair in athletes, emphasizing the restoration of strength and function.
- Bak et al. (2000) showed significantly better results in patients treated surgically compared to conservatively, particularly regarding strength deficits and cosmetic deformity.
-
Chronic Ruptures and Reconstruction: While acute repairs yield better results, surgical reconstruction for chronic tears can still be beneficial for symptomatic patients, though outcomes are generally inferior. The challenge lies in managing muscle retraction, atrophy, and scar tissue.
- Providenti et al. (2014) reviewed various graft options for chronic tears, noting that while functional gains are achieved, full restoration of strength and contour is less predictable than with acute repair. Allografts (e.g., Achilles tendon, semitendinosus) are commonly used for augmentation or bridging defects.
-
Repair Techniques: Humeral avulsion tears are most commonly repaired using transosseous sutures or suture anchors.
- Aarons et al. (2015) and other biomechanical studies have investigated various anchor configurations, with double-row or suture bridge techniques theoretically offering improved footprint coverage and superior biomechanical properties compared to single-row techniques, though clinical superiority is still debated.
- The use of robust locking stitches (e.g., Krackow) for tendon-suture interface has been well-established to resist pull-out.
-
Partial Tears: Management of partial tears is less standardized. Most literature suggests non-operative management for smaller tears (<50% involvement) in low-demand individuals. However, larger partial tears or those in symptomatic, high-demand patients often warrant surgical consideration, given the risk of progression to complete rupture or persistent functional deficit.
-
Rehabilitation Protocols: While specific timelines vary, a general consensus supports a phased approach:
- Initial Immobilization: To protect the repair.
- Gradual Passive/Assisted Range of Motion: To prevent stiffness.
- Progressive Strengthening: Beginning with isometric exercises and slowly advancing to isotonic and functional training.
- Return to Sport: A protracted period (6-12 months) is typically recommended before full return to high-demand activities to allow for adequate tendon-to-bone healing and muscle remodeling.
-
Diagnostic Imaging: MRI remains the gold standard for accurately diagnosing the location, extent, and chronicity of pectoralis major ruptures, guiding surgical planning.
In conclusion, the prevailing evidence strongly advocates for prompt surgical intervention for acute complete pectoralis major ruptures in active individuals to achieve optimal functional and cosmetic outcomes. Ongoing research continues to refine surgical techniques and rehabilitation strategies, particularly for complex chronic cases, aiming to bridge the gap in outcomes between acute and delayed repairs.
Clinical & Radiographic Imaging