Patient Presentation & History
A 68-year-old male, right-hand dominant, presented to the Orthopedic Trauma Clinic complaining of persistent right shoulder pain and significant functional limitation for the past four months. He reported a fall directly onto his outstretched right arm while descending stairs approximately four months prior. Immediately following the injury, he experienced severe pain and inability to move his shoulder. He sought care at an urgent care facility where radiographs were reportedly normal, and he was advised to rest and use analgesics. Despite this, his pain persisted, and he noted a constant feeling of "something being out of place," coupled with progressive stiffness and inability to perform activities of daily living, particularly overhead reaching and sleeping on his right side.
His medical history is significant for well-controlled hypertension, Type 2 Diabetes Mellitus, and a remote history of shoulder impingement managed non-operatively. He is a retired accountant, living independently. There is no history of prior shoulder dislocations. He denies any acute neurological deficits or vascular compromise in the affected limb since the initial injury. The delay in definitive diagnosis and presentation to a specialized orthopedic trauma service highlights the challenges of chronic dislocations, often missed in initial assessments, especially in the elderly or those with atypical presentations.
Clinical Examination
Upon inspection of the right shoulder, a clear deformity was evident. The normal rounded contour of the deltoid muscle was flattened anteriorly, and there was a palpable prominence of the acromion laterally. The humeral head was noted to be displaced anteriorly and inferiorly, creating a bulge in the subcoracoid region. There was no significant skin discoloration, open wounds, or signs of acute inflammation. Muscle atrophy, particularly of the deltoid, supraspinatus, and infraspinatus, was notable, consistent with disuse over four months.
Palpation revealed tenderness over the anterior aspect of the glenohumeral joint and the subcoracoid area, corresponding to the displaced humeral head. The posterior aspect of the joint felt empty. No crepitus was elicited on gentle manipulation.
Range of Motion (ROM) was severely restricted and painful. Active and passive ROM measurements were:
*
Flexion:
45 degrees (normal 180)
*
Abduction:
30 degrees (normal 180)
*
External Rotation (at 0 degrees abduction):
0 degrees (normal 60-70)
*
Internal Rotation (at 0 degrees abduction):
20 degrees (normal 70-80)
All movements were guarded, with a firm, painful end-feel. Apprehension testing was positive on attempts at external rotation and abduction.
Neurological assessment revealed an intact axillary nerve clinically, with good deltoid and teres minor contraction against resistance and normal sensation over the regimental badge area. Suprascapular, musculocutaneous, radial, ulnar, and median nerve functions were also intact. Distal vascular status was confirmed with palpable radial and ulnar pulses, normal capillary refill, and warm extremities.
Assessment of the cervical spine was unremarkable, ruling out a concomitant cervical radiculopathy contributing to shoulder pain or dysfunction.
Imaging & Diagnostics
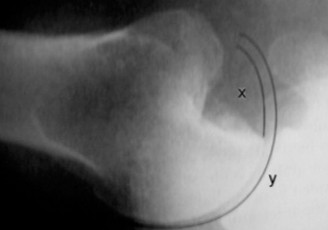
Initial radiographs, when reviewed, were indeed subtle but retrospectively demonstrated an anterior glenohumeral dislocation that was missed. A true AP glenoid view, an axillary view, and a scapular Y-view were obtained on current presentation.
*
AP Glenoid View:
Showed the humeral head displaced anteriorly and medially relative to the glenoid, lying inferior to the coracoid process.
*
Axillary View:
Crucial for confirming the direction of dislocation, clearly depicted the humeral head anterior to the glenoid. This view also allowed for a preliminary assessment of glenoid bone loss.
*
Scapular Y-View:
Demonstrated the humeral head lying anterior to the intersection of the Y, confirming anterior dislocation.

(Figure 1: Initial AP radiograph showing anterior inferior glenohumeral dislocation.)
Given the chronic nature of the dislocation (over 3 weeks), a Computed Tomography (CT) scan with 3D reconstructions was mandated to accurately assess the extent of bone loss and guide surgical planning. The CT scan revealed:
*
Glenoid Bone Loss:
A significant anterior-inferior glenoid bone defect, estimated to be approximately 25-30% of the glenoid width, consistent with a bony Bankart lesion. The glenoid track was compromised.
*
Humeral Head Defect (Hill-Sachs Lesion):
A large, engaging Hill-Sachs lesion on the posterior-superior aspect of the humeral head, measuring approximately 2.5 cm in length and 1.0 cm in depth. This lesion was clearly "on-track" given the glenoid defect.
*
Joint Space:
Mild degenerative changes were observed in the glenohumeral joint, consistent with the chronicity of the dislocation.
*
Coracoid Process:
Intact and well-defined.

(Figure 2: Coronal CT reconstruction demonstrating glenoid bone loss (bony Bankart) and the anteriorly dislocated humeral head.)
An Magnetic Resonance Imaging (MRI) scan was also performed to evaluate soft tissue pathology, particularly the rotator cuff tendons, labrum, and joint capsule.
*
Rotator Cuff:
Intact rotator cuff tendons (supraspinatus, infraspinatus, subscapularis, teres minor) with no evidence of acute or chronic tears, though some signal changes consistent with tendinosis were noted.
*
Labrum:
The anterior-inferior labrum was avulsed with the bony Bankart fragment. The posterior labrum appeared intact.
*
Capsule:
Evidence of chronic capsular stretching and thickening, particularly anteriorly.
*
Articular Cartilage:
Chondral changes on both the glenoid and humeral head, but no full-thickness cartilage defects warranting immediate arthroplasty.
(Figure 3: 3D CT reconstruction highlighting the anterior glenoid defect and the corresponding Hill-Sachs lesion on the humeral head.)
Templating for Glenoid Bone Loss:
The CT findings were critical for templating. Using the "best-fit circle" method or comparing the affected glenoid with the contralateral healthy glenoid, the anterior glenoid bone loss was quantified at approximately 28%. This degree of bone loss typically falls into the category requiring bony augmentation rather than solely soft tissue repair. The Hill-Sachs lesion was also templated to assess its size and engagement with the compromised glenoid, confirming its significant nature.
Differential Diagnosis
Given the clinical presentation and imaging, the primary diagnosis is a chronic anterior glenohumeral dislocation. However, in the workup of a patient with shoulder pain, deformity, and severe ROM restriction, several other conditions must be considered and systematically ruled out.
| Feature | Chronic Anterior Glenohumeral Dislocation (Primary Diagnosis) | Adhesive Capsulitis (Frozen Shoulder) | Rotator Cuff Tear Arthropathy | Proximal Humerus Fracture-Dislocation (Missed/Malunited) |
|---|---|---|---|---|
| History | Traumatic event, persistent pain & deformity, inability to move, initial missed diagnosis. | Insidious onset, progressive pain & stiffness over weeks/months, often post-trauma/surgery | Chronic shoulder pain, weakness, crepitus, progressive ROM loss, older age group. | Significant trauma, initial pain/swelling, limited motion, often missed in elderly. |
| Inspection | Flattened deltoid, prominent acromion, anterior/inferior humeral head bulge (subcoracoid). | Normal contour, mild generalized atrophy. | Atrophy of supra/infraspinatus fossae, superior migration of humeral head (late stage). | Deformity (angulation/shortening), swelling, ecchymosis, sometimes palpable crepitus. |
| Palpation | Tenderness anteriorly, empty posterior aspect. | Diffuse tenderness, no specific palpable deformity. | Tenderness over greater tuberosity/subacromial space. | Localized tenderness over fracture site, crepitus on motion. |
| Range of Motion (Active/Passive) | Severely restricted, painful in all planes, firm end-feel due to mechanical block. | Severely restricted, painful in all planes, especially external rotation; global loss. | Severely restricted active ROM (pseudoparalysis), often better passive ROM (unless arthritic). | Severely restricted and painful. Active ROM may be absent depending on fracture type. |
| Stability | Grossly unstable, fixed dislocation. | Stable. | May have superior instability (cuff tear) but not fixed dislocation. | May be unstable if poorly united, but fixed deformity is characteristic. |
| Neurological Exam | Axillary nerve palsy possible (acute or chronic), must be thoroughly assessed. | Typically normal. | Typically normal, but some may have associated nerve compression (e.g., suprascapular). | May have associated brachial plexus injury, especially axillary nerve. |
| Radiographs | Humeral head clearly not articulating with glenoid, displaced anterior/inferior. | Normal joint space, osteopenia. | Superior migration of humeral head, reduced acromiohumeral interval, glenohumeral arthritis. | Fracture lines/malunion, displacement of humeral head relative to glenoid (if dislocated). |
| CT Scan | Confirms dislocation, quantifies glenoid bone loss (bony Bankart), Hill-Sachs lesion. | Normal bony anatomy. | Erosive changes of acromion, glenoid, humeral head. Extensive cuff retraction. | Detailed fracture morphology, malunion, fragment displacement. |
| MRI Scan | Soft tissue assessment: labral tear, capsular injury, rotator cuff integrity. | Capsular thickening and contraction (especially inferior capsule), normal labrum/cuff. | Massive rotator cuff tear, cartilage loss, synovial hypertrophy. | Soft tissue injury associated with fracture, rotator cuff integrity (if not clear on CT). |
| Treatment Implications | Requires reduction, often with bone augmentation (Latarjet) and soft tissue repair (Remplissage) | Physiotherapy, NSAIDs, corticosteroid injections. MUA/arthroscopic capsular release (refractory). | Rotator cuff repair (if possible), reverse shoulder arthroplasty (for irreparable tears). | Open reduction internal fixation, shoulder arthroplasty (if severely comminuted/osteoporotic). |
Surgical Decision Making & Classification
The decision for operative intervention in this case was straightforward due to the chronic nature of the dislocation (4 months), the failure of any attempted closed reduction in the acute phase, significant patient disability, and critical imaging findings of substantial bony defects. Chronic glenohumeral dislocations rarely respond to closed reduction beyond 3 weeks, especially with large engaging bony lesions.
Classification:
1.
Based on Chronicity:
Chronic Glenohumeral Dislocation (defined as unreduced for >3 weeks).
2.
Based on Direction:
Anterior-Inferior Glenohumeral Dislocation.
3.
Based on Bone Loss (Glenoid):
The CT scan revealed ~28% glenoid bone loss, classifying it as severe. This magnitude of bone loss (typically >20-25%) strongly indicates the need for bony augmentation rather than isolated soft tissue repair (e.g., Bankart repair), which would be prone to high recurrence rates.
4.
Based on Humeral Head Defect (Hill-Sachs):
A large, engaging Hill-Sachs lesion was identified. The concept of the "glenoid track" is critical here. With a compromised glenoid (bone loss >20%), even a moderately sized Hill-Sachs lesion can become "off-track," leading to engagement and recurrent instability. In this case, the large Hill-Sachs lesion was on-track relative to the remaining glenoid, but it would engage the bone defect, contributing to instability.
Indications for Operative Management:
* Failed closed reduction (either attempted or deemed inappropriate due to chronicity/bone loss).
* Significant glenoid bone loss (>20-25%).
* Large, engaging Hill-Sachs lesion.
* Persistent pain and functional disability.
* Risk of progressive chondral damage and early osteoarthritis if left unreduced.
* Risk of neurovascular compromise due to chronic displacement.
Contraindications (relative):
* Significant medical comorbidities precluding surgery.
* Irreparable rotator cuff tear with advanced glenohumeral arthritis (may warrant arthroplasty).
* Patient unwilling to undergo surgery or adhere to rehabilitation protocol.
Considering the patient's age, activity level, significant bone loss, and the unlikelihood of successful closed reduction, the decision was made for an open reduction of the glenohumeral joint combined with an anterior glenoid bony augmentation (Latarjet procedure) and a remplissage procedure to address the Hill-Sachs lesion. This comprehensive approach aims to restore glenohumeral stability, address bone defects, and prevent recurrence.
Surgical Technique / Intervention
The patient was positioned in the supine beach chair position on a specialized shoulder operating table. The head was secured, and the torso was tilted to allow full access to the shoulder. The right arm was draped free to allow full range of motion intraoperatively. Standard anesthetic protocol was followed, including a regional interscalene block for post-operative analgesia.
Surgical Approach
A standard deltopectoral approach was utilized.
1.
Incision:
A curvilinear incision was made along the deltopectoral groove, starting just medial to the coracoid tip and extending distally approximately 8-10 cm.
2.
Interval:
The cephalic vein was identified and retracted laterally with the deltoid, exposing the pectoralis major tendon. The clavipectoral fascia was incised lateral to the conjoined tendon.
3.
Identification of Structures:
The conjoined tendon (coracobrachialis and short head of biceps) was identified. The subscapularis muscle was then visualized.
4.
Exposure of Joint:
Due to the chronic nature of the dislocation, the normal anatomy was significantly distorted. Extensive adhesions and fibrous tissue had formed around the dislocated humeral head. The anterior capsule was thickened and contracted. The subscapularis muscle was often retracted and adhered to the humeral neck.
Reduction Technique
- Capsular Release: A T-shaped capsulotomy was performed. The horizontal limb was along the neck of the humerus, and the vertical limb extended inferiorly. The anterior capsule and associated adhesions were carefully released.
- Subscapularis Mobilization: The subscapularis tendon was identified. Due to chronicity and potential contracture, a subscapularis tenotomy was performed to allow adequate exposure and mobilization. The tendon was tagged for later repair.
- Humeral Head Mobilization: The dislocated humeral head was encircled with an elevator or a blunt instrument to carefully free it from surrounding fibrous tissue and adhesions. Gentle traction was applied to the arm in abduction and external rotation, while an assistant applied posterior pressure to the humeral head. This maneuver aimed to bring the humeral head superiorly and laterally towards the glenoid.
- Reduction: With careful manipulation and persistent traction, the humeral head was reduced back into the glenoid fossa. This was often challenging due to muscle spasm, capsular contracture, and the large Hill-Sachs defect. Once reduced, the stability was assessed. The reduced position was maintained by internally rotating the arm.
Latarjet Procedure for Glenoid Bone Loss
Given the significant anterior glenoid bone loss (~28%), a Latarjet procedure was chosen to reconstruct the anterior glenoid rim and provide a muscular sling effect.
1.
Coracoid Harvest:
The coracoid process was carefully exposed. Its tip was osteotomized, along with the attached conjoined tendon and pectoralis minor insertion, maintaining soft tissue attachments. A 2.7 mm drill hole was typically placed in the base of the coracoid graft.
2.
Glenoid Preparation:
The anterior glenoid rim was debrided, and a bleeding bony bed was prepared. The location for the coracoid graft was marked, typically flush with the articular cartilage of the glenoid.
3.
Graft Fixation:
The harvested coracoid graft was rotated 90 degrees and positioned flush against the anterior-inferior glenoid defect. Two cortical screws (typically 3.5 mm fully threaded, cannulated) were passed through the coracoid graft, through the remnant glenoid bone, and into the scapular neck. Intraoperative fluoroscopy was used to confirm appropriate screw length and position, ensuring bicortical purchase and avoiding neurovascular structures. The screws were countersunk to prevent hardware prominence.
4.
Capsular Repair:
The remaining anterior capsule and labrum were repaired over the Latarjet graft, further augmenting stability.
Remplissage Procedure for Hill-Sachs Lesion
To address the engaging Hill-Sachs lesion and prevent future engagement, a remplissage (filling) procedure was performed.
1.
Exposure:
The posterior aspect of the humeral head was visualized by internally rotating the arm.
2.
Capsulotenodesis:
The infraspinatus tendon and posterior capsule were advanced into the Hill-Sachs defect and sutured into place using suture anchors. Typically, 2-3 anchors were placed into the base of the Hill-Sachs lesion, and sutures were passed through the infraspinatus tendon and posterior capsule, effectively obliterating the defect and converting an "on-track" (but engaging) lesion into an "off-track" functional lesion.
Closure
- Subscapularis Repair: The subscapularis tendon, if tenotomized, was meticulously repaired using strong non-absorbable sutures in a pants-over-vest or side-to-side fashion.
- Wound Closure: The wound was irrigated thoroughly. The deltopectoral fascia was closed. Subcutaneous tissues and skin were closed in layers. A sterile dressing was applied, and the arm was placed in a shoulder immobilizer sling with the arm in a neutral rotation.
Post-Operative Protocol & Rehabilitation
The post-operative protocol is crucial for successful outcomes following complex reconstructive procedures for chronic shoulder dislocations. This protocol is typically more conservative than for acute repairs due to the extensive soft tissue release, bone grafting, and the need for graft integration.
Phase I: Immobilization & Protection (0-6 weeks)
- Immobilization: The arm is immobilized in a shoulder immobilizer sling with neutral rotation for 4-6 weeks, worn continuously except for hygiene and prescribed exercises.
- Pain Management: Multimodal analgesia including regional nerve blocks, NSAIDs, and opioid analgesics.
-
Early ROM (Passive):
- Weeks 0-2: Pendulum exercises initiated on post-operative day 1. Passive forward flexion to 60-70 degrees and external rotation to 0-10 degrees (with care not to stress the Latarjet graft or remplissage). No abduction, active ROM, or internal rotation beyond neutral.
- Weeks 2-6: Gradual increase in passive forward flexion to 90-120 degrees, and external rotation to 20-30 degrees. Passive internal rotation to 30 degrees. Manual therapy by a physical therapist to prevent stiffness. Scapular mobilization.
- No Weight Bearing/Lifting: No lifting, pushing, pulling, or sudden movements.
- Activities of Daily Living (ADLs): Assistance with dressing, showering, and other ADLs.
Phase II: Early Active & Progressive ROM (6-12 weeks)
- Sling Discontinuation: Gradual weaning from the sling, typically around 6 weeks, as tolerated.
-
Active-Assisted ROM (AAROM):
Begin active-assisted range of motion, progressing to active ROM as tolerated.
- Weeks 6-8: AAROM to full flexion and abduction. Active external rotation up to 45 degrees.
- Weeks 8-12: Progress to full active ROM in all planes. Gentle isometric strengthening for rotator cuff and deltoid.
- Subscapularis Precautions: Avoid resisted internal rotation for the first 8-10 weeks to protect the subscapularis repair.
- Scapular Strengthening: Focus on periscapular stabilization exercises.
- Gentle Stretching: PNF stretching, pulley exercises.
- Functional Activities: Light ADLs without resistance.
Phase III: Strengthening & Advanced Rehabilitation (12-24 weeks)
-
Progressive Strengthening:
Advance to isotonic strengthening with light resistance bands and weights. Focus on all major muscle groups:
- Rotator cuff (internal/external rotators, abductors)
- Deltoid
- Scapular stabilizers (rhomboids, serratus anterior, trapezius)
- Proprioception and Neuromuscular Control: Begin exercises for balance and coordination (e.g., rhythmic stabilization).
- Endurance Training: Low-impact cardiovascular activities.
- Sport-Specific (if applicable): Initiate sport-specific drills, emphasizing controlled movements.
- Avoidance of High-Risk Activities: Still avoid forceful overhead activities, heavy lifting, or contact sports.
Phase IV: Return to Activity (6+ months)
- Gradual Return: Gradual return to full activity, including overhead sports or heavy manual labor, typically around 6-9 months, contingent on achieving full, pain-free ROM and adequate strength (usually 90% strength compared to the contralateral side).
- Continued Strengthening: Maintain a regular strengthening and conditioning program.
- Patient Education: Emphasize the importance of protecting the shoulder and avoiding provocative positions.
Throughout all phases, close collaboration between the surgeon and physical therapist is essential. Regular clinical assessments and objective strength measurements guide progression.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls
- High Index of Suspicion: For any shoulder injury presenting with limited ROM, always suspect dislocation, even if initial radiographs are reported as normal. Obtain multiple views (AP, Y-scapular, axillary) and insist on review. The axillary view is non-negotiable for diagnosing and characterizing dislocation.
- Chronicity Definition: Dislocation unreduced for >3 weeks is considered chronic. This significantly alters management.
- Imaging for Bone Loss: For chronic dislocations, a CT scan with 3D reconstruction is mandatory. It's the gold standard for quantifying glenoid bone loss and characterizing Hill-Sachs lesions (size, depth, engagement). This directly guides surgical strategy (soft tissue vs. bone block).
- Glenoid Track Concept: Understand how the Hill-Sachs lesion interacts with the glenoid rim. A critical glenoid bone defect (usually >20-25%) effectively moves the "on-track" zone medially, making many Hill-Sachs lesions effectively "off-track" or engaging even if they appear "on-track" on a normal glenoid. This necessitates addressing both lesions.
- Latarjet's Dual Effect: The Latarjet procedure provides both a bony block (coracoid graft) and a dynamic sling effect (conjoined tendon). It is highly effective for severe glenoid bone loss and high-risk patients (contact athletes, revision cases).
- Remplissage for Hill-Sachs: The remplissage procedure (infraspinatus tenodesis into the Hill-Sachs defect) is a useful adjunct for engaging Hill-Sachs lesions, converting them into non-engaging lesions. It can be performed arthroscopically or through the open approach with a Latarjet.
- Neurovascular Assessment: Meticulous pre- and post-operative neurovascular assessment, especially for the axillary nerve, is paramount due to the proximity of the brachial plexus to the dislocated humeral head. Chronic compression can lead to neuropraxia.
- Pre-operative Planning: Thorough templating of bone loss and choice of graft (autograft vs. allograft) or procedure (Latarjet, distal tibia allograft, iliac crest graft) is critical.
Pitfalls
- Missed Diagnosis: The most common pitfall. Often due to inadequate imaging or misinterpretation of radiographs, especially in poly-trauma or elderly patients.
- Attempting Forceful Closed Reduction: In chronic dislocations (>3 weeks) or those with significant bone loss, forceful closed reduction carries a high risk of iatrogenic fracture (humeral head, glenoid), rotator cuff tears, or neurovascular injury. Such attempts are generally contraindicated.
- Underestimating Bone Loss: Relying solely on radiographs for bone loss assessment is insufficient and can lead to inadequate treatment and recurrent instability.
- Inadequate Graft Fixation (Latarjet): Poorly positioned or inadequately fixed coracoid graft can lead to non-union, malunion, or recurrence. Screws must be bicortical and well-positioned.
- Ignoring the Hill-Sachs Lesion: Even with a successful glenoid reconstruction, an unaddressed engaging Hill-Sachs lesion can lead to persistent apprehension or recurrence.
- Overly Aggressive Rehabilitation: Especially in the early post-operative phase, aggressive range of motion or strengthening can jeopardize graft healing, soft tissue repair (subscapularis), or Latarjet graft integrity. A protected, gradual rehabilitation protocol is essential.
- Recurrence: Despite meticulous surgery, recurrence is always a possibility, particularly in high-risk patients, those with persistent risk factors, or if technical errors occur. Early recognition and re-evaluation are critical.
- Stiffness/Arthrosis: While stability is the primary goal, excessive capsular tightening or prolonged immobilization can lead to post-operative stiffness or accelerate arthritic changes, especially in chronic cases with pre-existing cartilage damage.
- Infection: As with any open surgery, infection is a potential complication, requiring meticulous sterile technique and appropriate prophylactic antibiotics.
Clinical & Radiographic Imaging

