Introduction to Chronic Unreduced Shoulder Dislocations
Old, unreduced dislocations of the shoulder represent a formidable challenge in orthopedic surgery, demanding a profound understanding of altered glenohumeral pathoanatomy and biomechanics. By definition, a dislocation is considered "chronic" or "old" when it has remained unreduced for more than three to four weeks.
Epidemiologically, these injuries exhibit a bimodal distribution. They most frequently occur in patients older than 50 years. In this demographic, the dislocation is often traumatic but is frequently precipitated by a seemingly trivial injury. This susceptibility is largely due to the patient’s advancing age, inherent muscular weakness, and progressive degeneration of the soft tissues surrounding the glenohumeral joint, particularly the rotator cuff and the subscapularis tendon.
Conversely, in younger patient populations, chronic unreduced dislocations are highly correlated with specific comorbidities and high-energy mechanisms. They most often occur in individuals with a history of alcoholism, uncontrolled seizure disorders, or those who have sustained polytrauma where the shoulder injury was initially missed during the primary trauma survey.
Clinical Pearl: Always maintain a high index of suspicion for posterior shoulder dislocations in patients presenting with shoulder pain following a seizure or electrical shock. These are the most commonly missed major joint dislocations in emergency departments.
Clinical Presentation and Physical Examination
The hallmark complaints of a patient with a chronic unreduced shoulder dislocation are intractable pain and a profound limitation of motion.
Pain Mechanisms
The pain profile in chronic dislocations differs from acute trauma. The pain is usually mechanically induced, caused specifically by the patient's attempts to move the shoulder beyond its newly restricted, pathological range of motion. At rest, the shoulder may be relatively asymptomatic once the initial acute inflammatory phase has subsided, but functional demands provoke severe discomfort due to impingement and capsular tension.
Range of Motion Deficits
Loss of motion is the chief clinical finding, and the specific pattern of restriction is pathognomonic for the direction of the dislocation:
* Old Anterior Dislocations: Patients exhibit a severe restriction in abduction and internal rotation. The humeral head is locked anteriorly, preventing the normal rolling and gliding kinematics required for these arcs of motion.
* Old Posterior Dislocations: Patients demonstrate a marked restriction in abduction and external rotation. The arm is typically locked in internal rotation, and any attempt to externally rotate the humerus is met with a firm, mechanical block.
Neurological and Associated Complications
These injuries are rarely isolated. Many chronic dislocations are complicated by concomitant fractures of the glenoid cavity, the greater or lesser tuberosities, or the surgical neck of the humerus.
Surgical Warning: More than one-third (33%) of chronic unreduced shoulder dislocations are complicated by neurological deficits. The axillary nerve and the brachial plexus are at extreme risk due to chronic traction and encasement in dense fibrotic scar tissue. A meticulous preoperative neurological examination is mandatory.
Pathoanatomy and Biomechanics
Chronic dislocations produce profound, progressive pathological conditions in both the soft tissues and the osseous structures of the shoulder girdle. The natural anatomy is often markedly distorted, making surgical navigation hazardous.
Soft-Tissue Contractures and Capsular "Bowstringing"
Within a few weeks of the initial dislocation, dense fibrous and capsular contractures develop across the base of the glenoid. The rotator cuff muscles, deprived of their normal resting length, become severely contracted and fibrotic. This fibrosis is not limited to the joint capsule; it frequently extends into the axilla, enveloping critical neurovascular structures, including the axillary artery and axillary nerve.
Neviaser classically described a capsular “bowstringing” phenomenon that is critical to understand. The capsule itself becomes densely adherent to the empty glenoid fossa. This fibrotic obliteration of the joint space acts as a physical barrier, absolutely preventing closed reduction.

As illustrated above, in an old anterior dislocation, adhesions of the posterior capsule to the glenoid surface develop. Conversely, in an old posterior dislocation, adhesions of the anterior capsule to the glenoid surface develop.
Bony Pathological Changes
The osseous architecture undergoes significant remodeling and destruction due to the chronic abnormal articulation.
Anterior Dislocations:
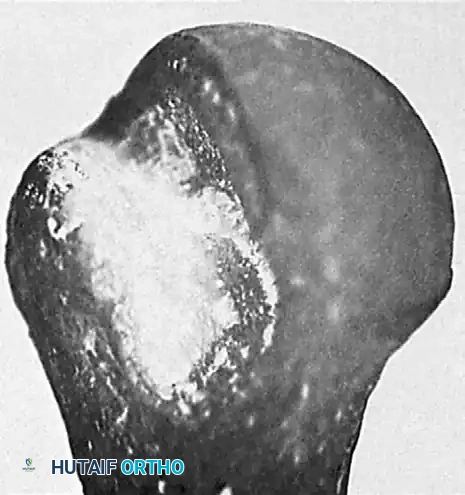
In chronic anterior dislocations, a massive compression fracture occurs in the posterolateral aspect of the humeral head where it continuously impinges against the hard anterior glenoid rim. Because of the repeated, forceful efforts of the patient to achieve normal motion in the locked joint, this lesion is often substantially larger than the classic Hill-Sachs lesion seen in recurrent, episodic anterior dislocations.
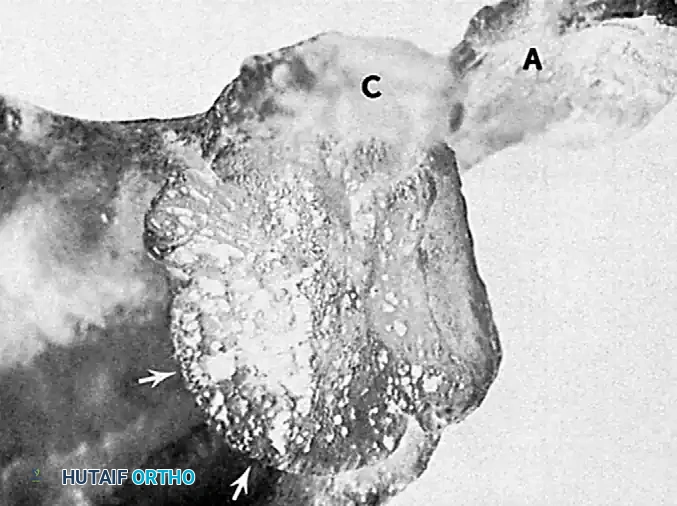
Furthermore, the constant friction and pressure lead to compression fractures and severe wear of the apposing anterior glenoid rim. In long-standing cases, the body attempts to adapt by forming a pseudoarticulation (false joint) between the displaced humeral head and the anterior aspect of the scapula.
Posterior Dislocations:
In chronic posterior dislocations, a similar but reversed bony lesion is found. This is a compression fracture caused by the impingement of the posterior rim of the glenoid on the anteromedial aspect of the humeral head (often termed a "reverse Hill-Sachs" or McLaughlin lesion). Like their anterior counterparts, these lesions are usually massive due to the patient’s continual attempts to increase the range of motion against a fixed bony block.
Radiographic and Advanced Imaging Evaluation
A complete and exhaustive radiographic evaluation is the cornerstone of preoperative planning.
Standard Radiography
Initial evaluation must include a true anteroposterior (Grashey) view and an axillary view of the shoulder. The axillary view is non-negotiable, as it definitively confirms the direction of the dislocation and provides an initial assessment of the articular defects. If pain precludes a standard axillary view, a Velpeau axillary view should be obtained.
Advanced Cross-Sectional Imaging
Computed Tomography (CT), particularly with three-dimensional (3D) reconstruction techniques, is mandatory. CT is highly helpful in evaluating the complex bony injuries, quantifying glenoid bone loss, and precisely measuring the extent of damage to the articular surface of the humeral head.
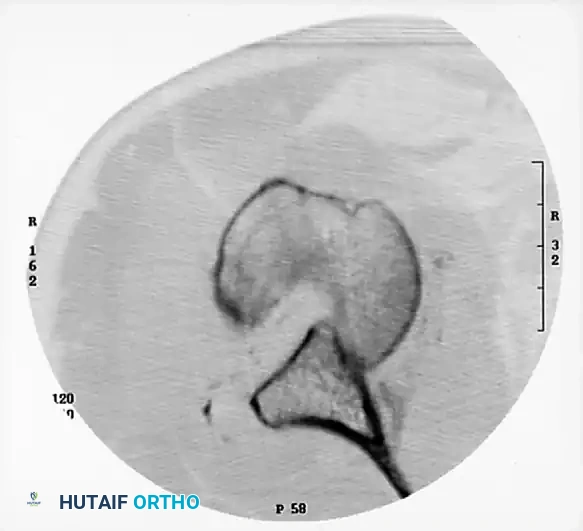
Surgical Pearl: The degree of damage to the articular surface, as quantified on the preoperative CT scan, is the major determining factor in the surgical procedure selected. Defects involving less than 20-25% of the articular surface may be amenable to joint-preserving procedures (e.g., allograft reconstruction, transfer of the lesser tuberosity). Defects exceeding 40-50% typically necessitate prosthetic arthroplasty.
Surgical Management and Operative Techniques
The surgical management of chronic unreduced dislocations is a major undertaking. Closed reduction should never be forcefully attempted in a truly chronic setting (>3-4 weeks) due to the high risk of iatrogenic humeral neck fracture, axillary artery rupture, or brachial plexus avulsion.
Patient Positioning and Anesthesia
The procedure is typically performed under general anesthesia supplemented with an interscalene regional block for postoperative pain control. The patient is placed in the beach-chair position, allowing full access to the anterior shoulder and the ability to manipulate the arm freely. The arm is draped free, and a sterile Mayo stand may be used to support the limb.
The Surgical Approach
An extended deltopectoral approach is the workhorse for chronic anterior dislocations.
1. Incision: A standard incision is made from the coracoid process extending distally toward the deltoid tuberosity.
2. Interval: The cephalic vein is identified and usually retracted laterally with the deltoid to preserve its venous drainage, though medial retraction is acceptable if necessary.
3. Deep Dissection: The clavipectoral fascia is incised. The conjoined tendon is identified and retracted medially. In chronic cases, the anatomy here is often obliterated by scar tissue.
Soft-Tissue Release and Neurolysis
This is the most critical and dangerous phase of the operation.
1. Identify the Axillary Nerve: Before any capsular release is performed, the axillary nerve must be identified and protected. It is often tethered by inferior capsular fibrosis. A "tug test" on the nerve should be avoided; instead, meticulous sharp dissection is required to free it from the surrounding scar.
2. Subscapularis Management: The subscapularis is often severely contracted. It may be managed via a tenotomy, a lesser tuberosity osteotomy, or a Z-lengthening, depending on the degree of contracture and the planned reconstruction.
3. Capsulectomy: The adherent capsule (Neviaser's bowstringing) must be excised from the glenoid fossa. A complete 360-degree capsular release is often necessary to mobilize the humeral head.
Joint Reduction and Bony Reconstruction
Once the soft tissues are fully mobilized, the humeral head is gently levered into the glenoid fossa.
* If the humeral head defect is small, the joint may be stable after reduction.
* If a large defect is present, it must be addressed to prevent immediate re-dislocation. Options include structural allografting of the defect, or in older patients with severe articular destruction, hemiarthroplasty or total shoulder arthroplasty.
Management of Concomitant Shoulder Girdle Trauma
In patients with multiple trauma, chronic shoulder dislocations may be accompanied by other unreduced injuries of the shoulder girdle, such as chronic acromioclavicular (AC) joint disruptions or distal clavicle fractures. If concurrent reconstruction of the AC complex is indicated during the same anesthetic event, modern suspensory fixation techniques are employed:
* Reduction and Fixation: Reduce the distal clavicle remnant and fix it with an EndoButton (Smith & Nephew, Andover, MA) or similar cortical suspensory device to restore the coracoclavicular interval.
* Ligament Transfer: Transfer the coracoacromial ligament to the resected end of the clavicle (modified Weaver-Dunn technique) and fix it securely with heavy non-absorbable sutures to the EndoButton construct to provide biological augmentation to the mechanical fixation.
Postoperative Care and Rehabilitation Protocol
The postoperative rehabilitation protocol must balance the need for tissue healing with the prevention of recurrent stiffness, which is a major risk in these patients.
Phase I: Protection (Weeks 0 to 4)
* The arm is placed in a secure sling or shoulder immobilizer for 3 to 4 weeks postoperatively.
* During this period, normal use of the elbow, wrist, and hand is strongly encouraged to prevent distal stiffness and complex regional pain syndrome.
* The sling is removed only for gentle, gravity-assisted pendulum exercises and for bathing. Active shoulder motion is strictly prohibited.
Phase II: Early Motion (Weeks 4 to 8)
* The sling is discontinued.
* Passive range of motion (PROM) and active-assisted range of motion (AAROM) exercises are initiated under the guidance of a physical therapist.
* External rotation is carefully titrated based on the intraoperative tension of the subscapularis repair.
Phase III: Strengthening and Return to Function (Months 2 to 6)
* Progressive strengthening exercises (isometrics advancing to isotonic bands and light weights) are begun at 2 months postoperatively.
* Emphasis is placed on rotator cuff and periscapular stabilizer strengthening.
* Depending on the patient's age and the stability of the reconstruction, the patient can generally return to heavy labor or contact sports at 3 to 6 months postoperatively, provided full strength and dynamic stability have been restored.
Complications and Prognosis
The prognosis for chronic unreduced dislocations is guarded compared to acute injuries. Patients must be counseled preoperatively that a return to a completely "normal" shoulder is unlikely.
* Stiffness: The most common complication is postoperative stiffness, secondary to the extensive scar tissue formation and necessary capsular reconstruction.
* Avascular Necrosis (AVN): The risk of AVN of the humeral head is elevated due to the initial trauma and the extensive soft-tissue stripping required for reduction.
* Neurological Injury: Transient or permanent neurapraxia of the axillary or musculocutaneous nerves can occur despite meticulous surgical technique.
* Arthrosis: Progressive glenohumeral osteoarthritis is almost inevitable in cases of prolonged dislocation, often necessitating future arthroplasty if joint-preserving techniques were initially chosen.
