Introduction to Glenohumeral Instability
The shoulder, by virtue of its evolutionary design prioritizing global spatial positioning of the hand, sacrifices intrinsic osseous stability for an unparalleled range of motion. Consequently, it is one of the most unstable and frequently dislocated joints in the human body, accounting for nearly 50% of all major joint dislocations. The management of glenohumeral instability requires a profound understanding of the intricate balance between static ligamentous restraints and dynamic muscular forces.
Factors that heavily influence the probability of recurrent dislocations include the patient's age at the time of initial dislocation, return to contact or collision sports, and the presence of significant bipolar bone loss (glenoid or humeral head defects). The natural history of acute anterior shoulder dislocation in the young athlete is notoriously poor without surgical intervention. In the landmark study by McLaughlin and Cavallaro, which evaluated 101 acute dislocations, recurrence developed in 90% of patients younger than 20 years old, 60% of patients 20 to 40 years old, and only 10% of patients older than 40 years old. These findings were corroborated by McLaughlin and MacLellan, who noted a 95% recurrence rate in 580 acute dislocations in patients under 20, and by Rowe and Sakellarides, who reported a 94% recurrence rate in a cohort of 324 dislocations in the same age group.
Hovelius further emphasized the frequency of recurrence in younger patients, particularly athletes, noting that the duration of post-injury immobilization did not significantly alter the natural history of instability. Instead, the degree and location of the initial trauma strongly correlated with recurrence. While Itoi et al. suggested that immobilization in external rotation may theoretically reduce recurrence rates by tensioning the subscapularis and reducing the Bankart lesion, the presence of structural damage often dictates the outcome. Burkhart and DeBeer, Sugaya et al., and Itoi et al. have definitively shown that glenoid bone loss exceeding 20% results in critical bony instability. This critical bone loss diminishes the "safe arc" of humeral rotation provided by the glenoid, leading to catastrophic instability when the deficient anterior edge is loaded at extremes of motion.
Normal Functional Anatomy and Biomechanics
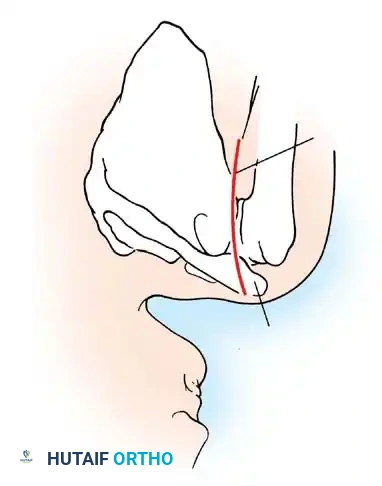
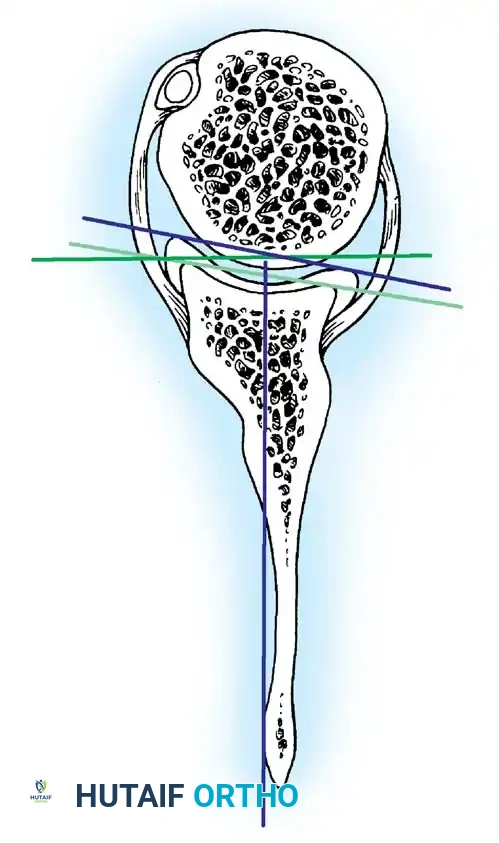
An exhaustive comprehension of normal functional anatomy is the cornerstone of diagnosing and surgically correcting shoulder instability. The bony architecture of the glenohumeral joint provides minimal inherent stability. The glenoid fossa is a flattened, dish-like structure, often compared to a golf tee. At any given time, only one-fourth to one-third of the large humeral head articulates with the glenoid. Unlike the deep acetabulum of the hip, this small, flat glenoid relies heavily on soft-tissue augmentations.
The Glenoid Labrum and Biceps Anchor
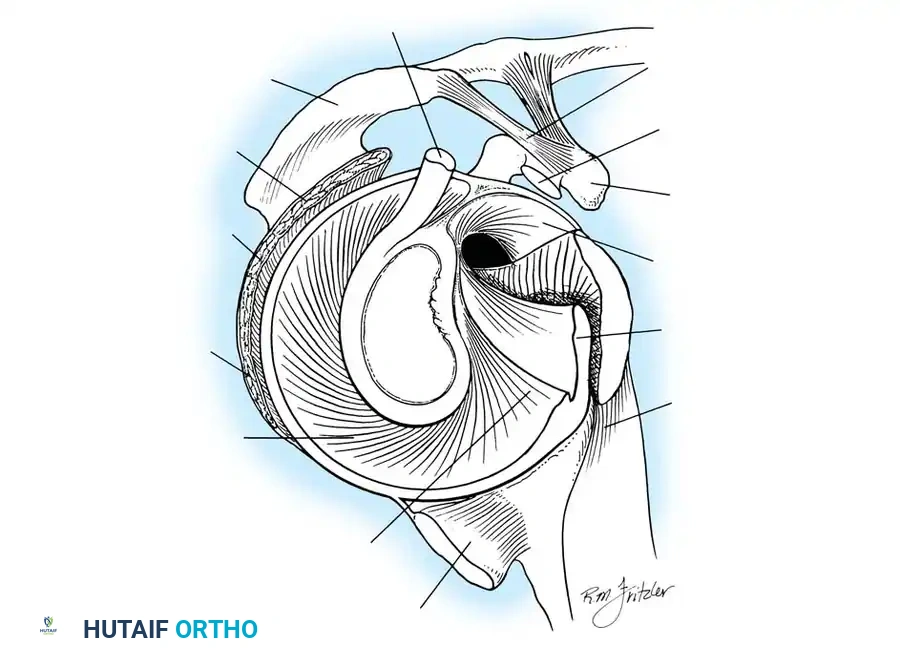
According to seminal studies by Howell et al., the effective depth of the glenoid is increased by 50% due to the presence of the fibrocartilaginous glenoid labrum. This structure acts as a bumper, increasing the humeral contact area to 75%. Integral to the superior glenoid labrum is the insertion of the long head of the biceps tendon, which blends indistinguishably into the posterior and anterior superior labrum. Matsen et al. conceptualized the labrum as a "chock block" that prevents excessive humeral head translation and rollback during physiological loading.
Capsuloligamentous Static Stabilizers
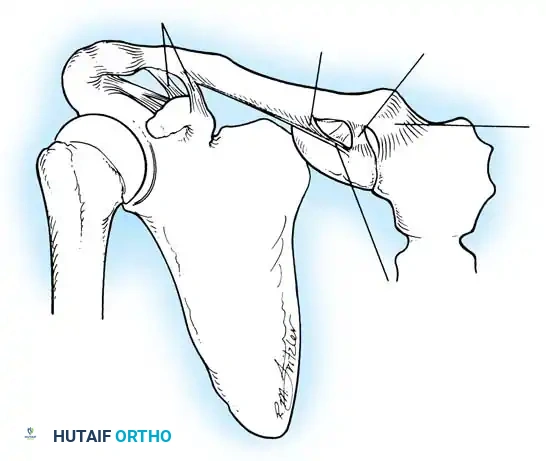
The shoulder joint capsule is inherently lax and thin, offering little resistance in isolation. However, it is reinforced anteriorly by three distinct capsular thickenings—the glenohumeral ligaments—which fuse intimately with the labral attachment on the glenoid rim. Turkel et al., alongside O’Brien, Warren, and Schwartz, have extensively mapped these structures.
- Superior Glenohumeral Ligament (SGHL): Attaches to the superior glenoid tubercle near the apex of the labrum, conjoined with the biceps anchor. It inserts onto the anterior aspect of the anatomical neck of the humerus. The SGHL is the primary restraint to inferior humeral subluxation at 0 degrees of abduction and serves as a primary stabilizer against anterior and posterior stress in the adducted arm. Harryman et al. demonstrated that tightening the rotator interval (which encompasses the SGHL and coracohumeral ligament) significantly decreases posterior and inferior translation.
- Middle Glenohumeral Ligament (MGHL): Features a wide origin extending from the SGHL along the anterior glenoid margin down to the junction of the middle and inferior thirds of the rim. It limits external rotation when the arm is in lower and middle ranges of abduction (45 degrees) but becomes redundant at 90 degrees of abduction.
- Inferior Glenohumeral Ligament (IGHL) Complex: The most critical static stabilizer. It attaches to the glenoid margin from the 2-o’clock to 3-o’clock positions anteriorly, extending to the 8-o’clock to 9-o’clock positions posteriorly. Its humeral attachment lies below the articular margin on the anatomical and surgical neck. O’Brien et al. described this complex as a "hammock-like" structure consisting of a thickened anterior band, a posterior band, and a thinner axillary pouch.

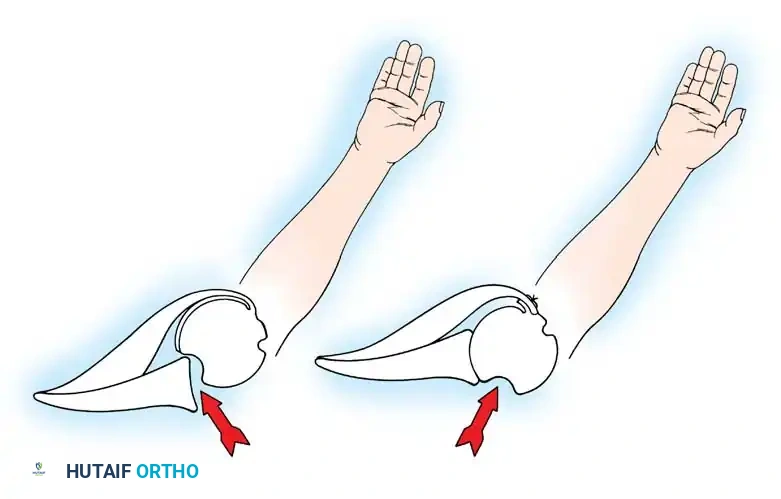
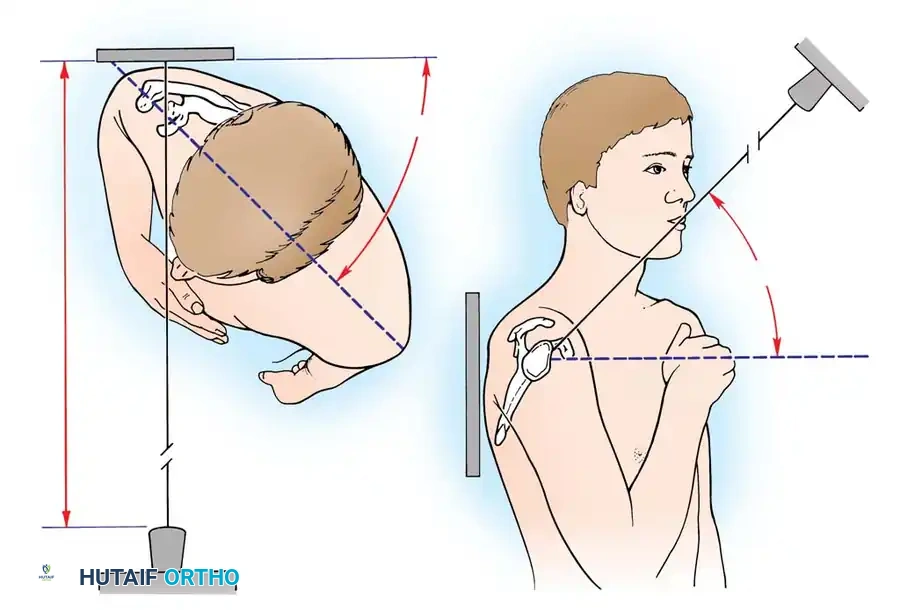
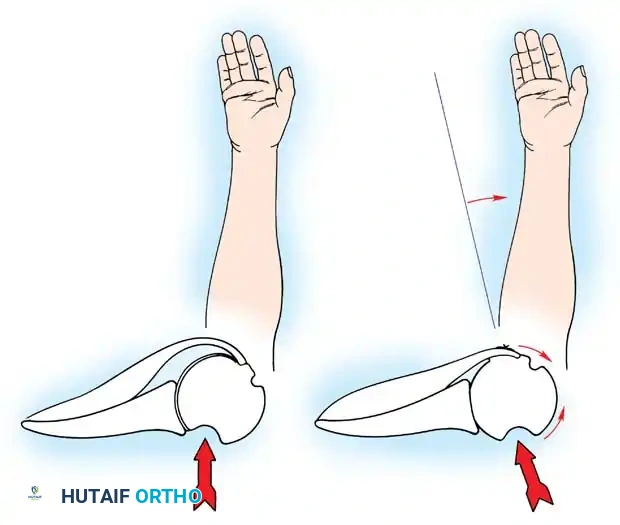
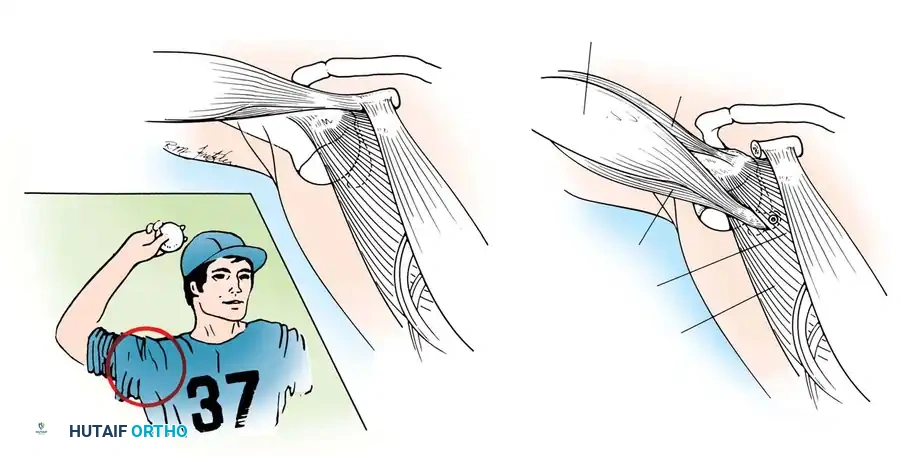
CLINICAL PEARL: The biomechanics of the IGHL complex are dynamic. With external rotation and abduction, the hammock shifts anteriorly and superiorly; the anterior band tightens to prevent anterior translation, while the posterior band fans out. Conversely, internal rotation tightens the posterior band. The anteroinferior band is the primary restraint to anterior translation at 90 degrees of abduction and external rotation (the classic apprehension position).
Turkel et al. demonstrated that true anterior dislocation cannot occur if the IGHL remains intact. Furthermore, Warren introduced the "circle concept," proving that for significant anterior translation to occur, there must be concomitant disruption or plastic deformation of the posterior capsular structures.
Dynamic Stabilizers and Concavity Compression
The musculature surrounding the shoulder provides essential dynamic stability. The deltoid produces primarily vertical shear forces, tending to displace the humeral head superiorly. To counteract this, the intrinsic muscles of the rotator cuff provide compressive forces. Lippitt and Matsen described "concavity compression," wherein the dynamic contraction of the rotator cuff compresses the humeral head into the concave glenoid socket. Loss of the labrum reduces this stabilizing effect by up to 20%.
Glousman et al. highlighted that synchronous eccentric deceleration and concentric contraction of the rotator cuff and biceps are vital for stability during mid-ranges of motion. Asynchronous fatigue from overuse or incompetent ligaments leads to microtrauma. MRI studies frequently reveal fatty infiltration and thinning of the subscapularis tendon in chronic recurrent anterior instability.
Furthermore, scapulothoracic kinematics play a massive role. Rowe, Kummel, and later Lippitt and Matsen emphasized that synchronous mobility of the scapula ensures the glenoid is optimally positioned beneath the humeral head, converting potential shear forces into compressive forces. Jobe and Glousman advocated for rigorous strengthening of scapular stabilizers (serratus anterior, trapezius, rhomboids) in overhead athletes. Proprioceptive feedback, mediated by Ruffini end organs and Pacinian corpuscles within the capsule (as demonstrated by Vangsness et al.), is also critical for dynamic neuromuscular control.
Pathological Anatomy of Recurrent Instability
No single "essential" lesion accounts for all recurrent shoulder instability; rather, it is a spectrum of structural failures.
The Bankart Lesion and Capsular Failure
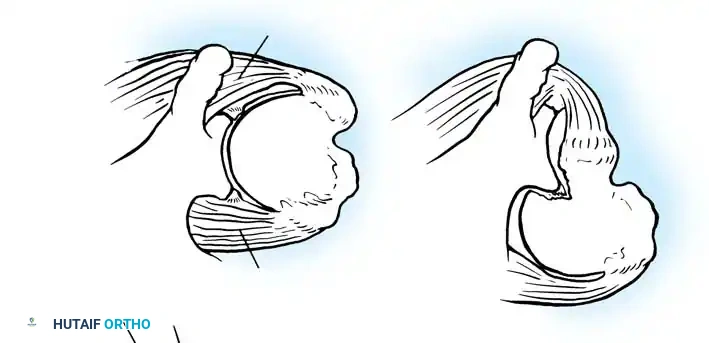
In 1906, Perthes first described the detachment of the anteroinferior labrum. In 1938, Bankart popularized the concept, describing the traumatic detachment of the fibrocartilaginous labrum and anterior capsule from the glenoid rim—now universally known as the Bankart lesion. Rowe et al. identified Bankart lesions in 85% of traumatic recurrent dislocations.
However, capsular laxity is equally detrimental. Rowe found excessive laxity in 28% of traumatic dislocations and 86% of failed surgical stabilization procedures. This laxity can stem from congenital collagen deficiencies (e.g., Ehlers-Danlos, Marfan syndrome) or plastic deformation from repetitive microtrauma.
Baker et al. arthroscopically evaluated acute dislocations, finding that 38% involved intrasubstance ligamentous failures, while 62% were avulsions from the glenoid. Bigliani et al. biomechanically tested the IGHL complex, revealing that failure occurs at the glenoid insertion (40%), midsubstance (35%), or the humeral insertion (25%). Humeral avulsion of the glenohumeral ligament (HAGL lesion), noted by Wolf et al. in 9% of acute dislocations, is a critical pathology that must not be missed, as standard Bankart repairs will fail to address it.
Bipolar Bone Loss
SURGICAL WARNING: Failure to recognize and address significant bipolar bone loss is the leading cause of recurrent instability following soft-tissue stabilization.
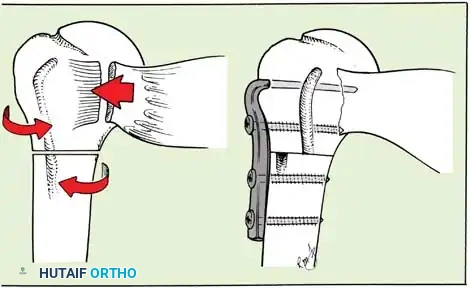
A Hill-Sachs lesion is an impaction fracture of the posterolateral humeral head, created when the head is driven against the hard anterior glenoid rim during dislocation. Burkhart and DeBeer introduced the concept of the "engaging" Hill-Sachs lesion, which levers the humeral head out of the joint when the arm is abducted and externally rotated.
Concurrently, anterior glenoid rim fractures or attritional bone loss can occur. Itoi demonstrated that a 20% loss of the anterior glenoid width critically compromises stability, rendering soft-tissue repairs (like an isolated Bankart repair) biomechanically insufficient. Advanced imaging (3D CT or MRI arthrography) is mandatory to quantify bone loss.
Surgical Management: Open Anterior Stabilization
While arthroscopic stabilization has become the gold standard for isolated soft-tissue Bankart lesions, open anterior stabilization remains a critical technique for revision cases, patients with poor capsular tissue, or those requiring concomitant bony augmentation (e.g., Latarjet procedure).
Indications for Open Surgery
- Recurrent instability with significant capsular deficiency or plastic deformation requiring a robust inferior capsular shift.
- HAGL lesions that are technically challenging to repair arthroscopically.
- Revision stabilization following a failed arthroscopic Bankart repair.
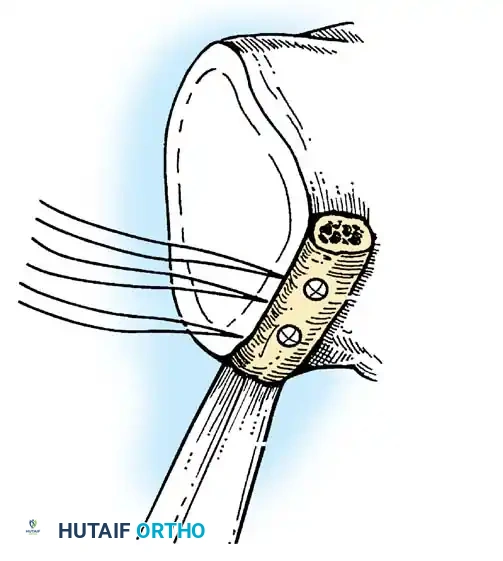
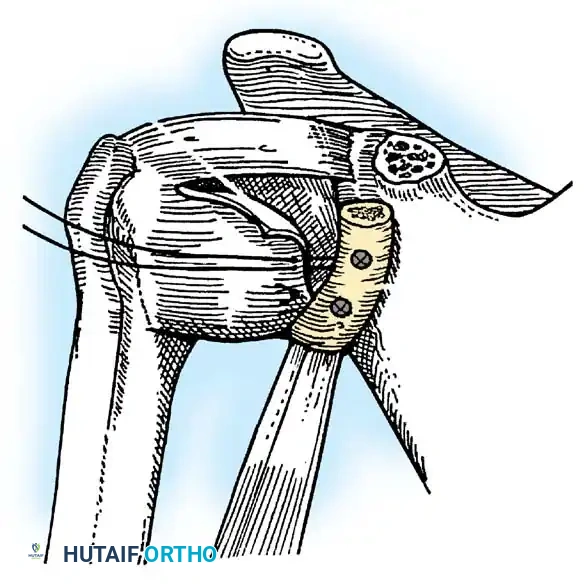
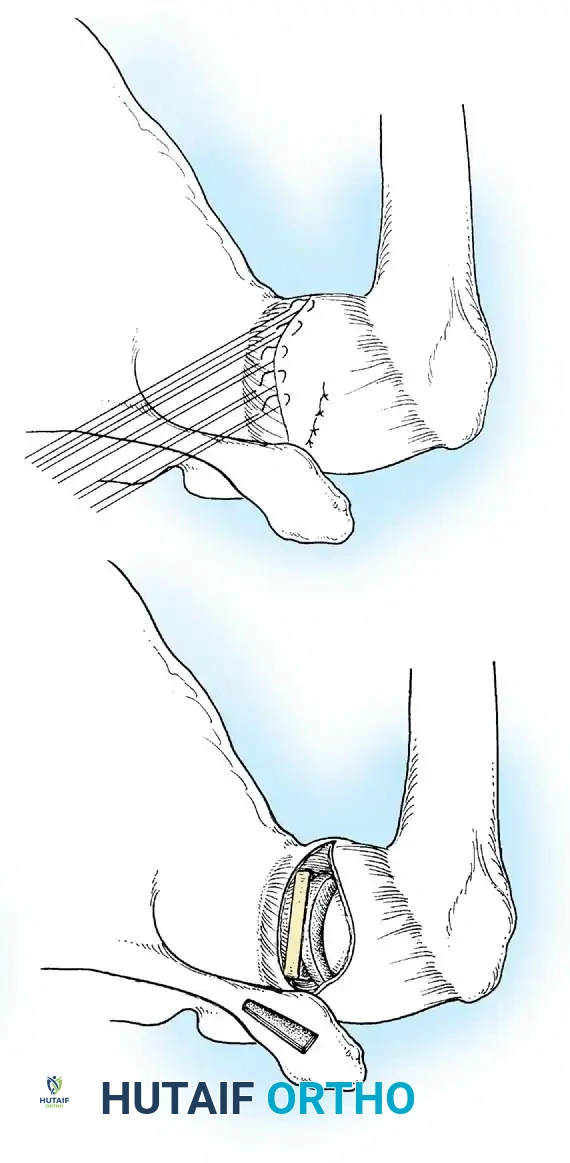
- Presence of glenoid bone loss (>15-20%) necessitating a coracoid transfer (Latarjet) or bone block.
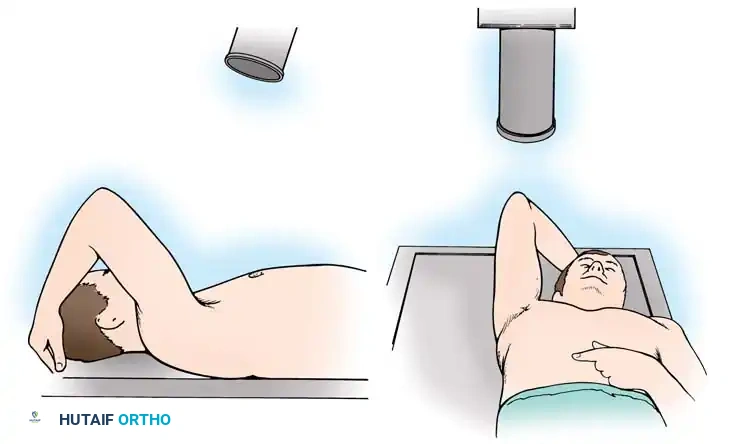
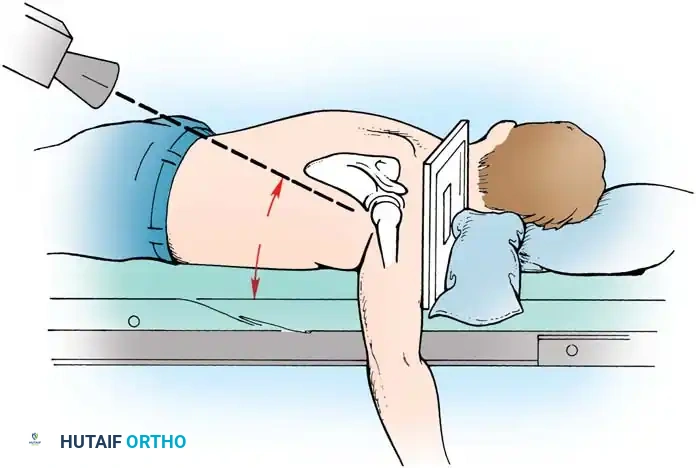
Patient Positioning and Anesthesia
The procedure is typically performed under general anesthesia supplemented with an interscalene regional nerve block for postoperative analgesia. The patient is placed in the beach-chair position with the head secured and the operative arm draped free to allow full manipulation. A mechanical arm holder is highly recommended to control rotation and abduction during the capsular shift.
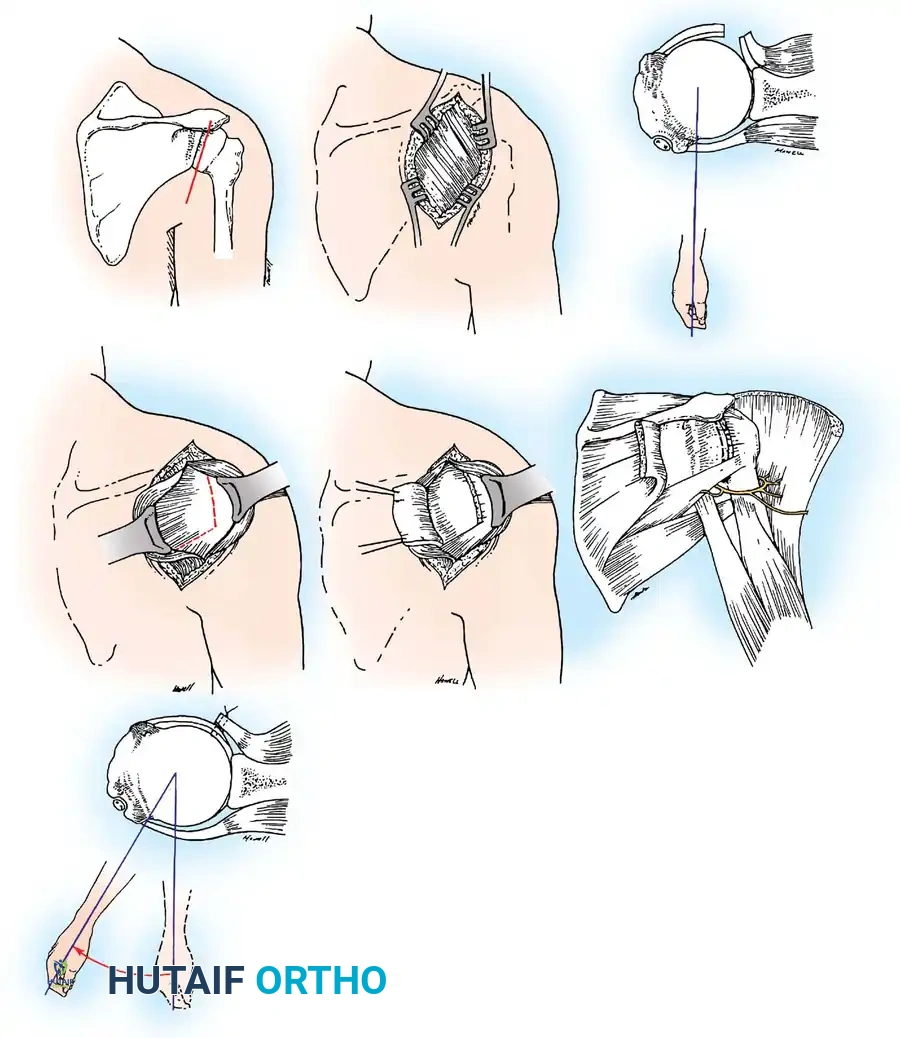
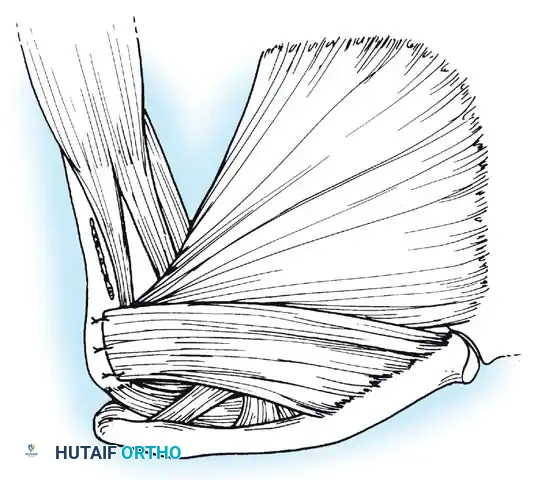
Surgical Approach: The Deltopectoral Interval
- Incision: A standard 5 to 7 cm incision is made starting from the tip of the coracoid process, extending distally and laterally toward the deltoid insertion.
- Superficial Dissection: The cephalic vein is identified within the deltopectoral groove. It is generally retracted laterally with the deltoid to preserve its venous drainage, though medial retraction with the pectoralis major is acceptable if lateral tributaries are sparse.
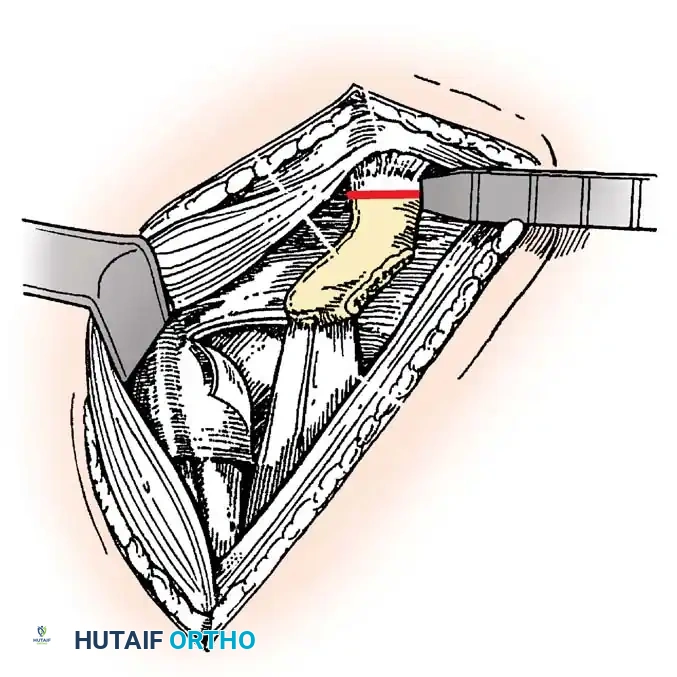
- Deep Dissection: The clavipectoral fascia is incised lateral to the conjoint tendon (short head of biceps and coracobrachialis). The conjoint tendon is retracted medially. Care must be taken to avoid aggressive medial retraction, which can cause a neurapraxia to the musculocutaneous nerve (typically entering the coracobrachialis 3-5 cm distal to the coracoid).
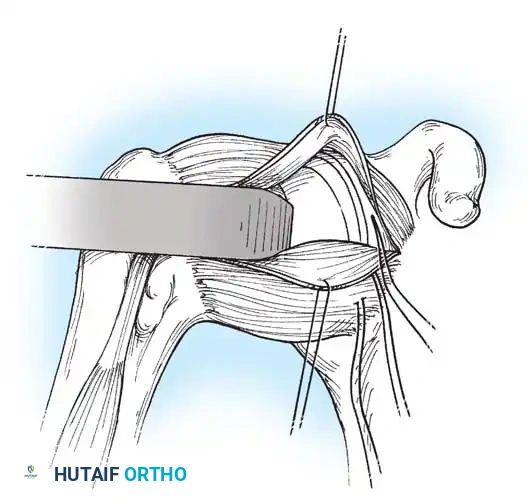
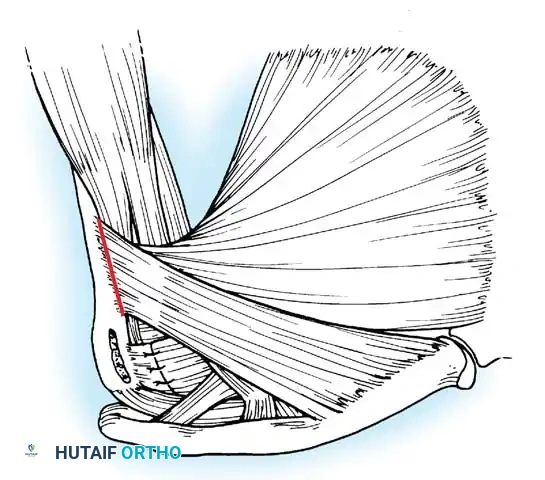
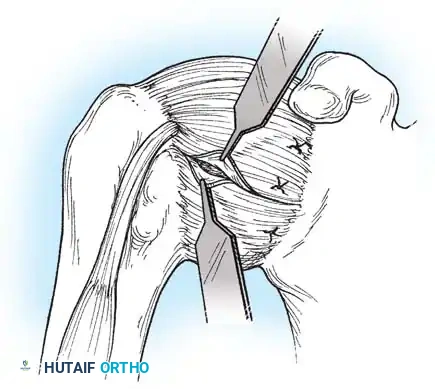
Subscapularis Management
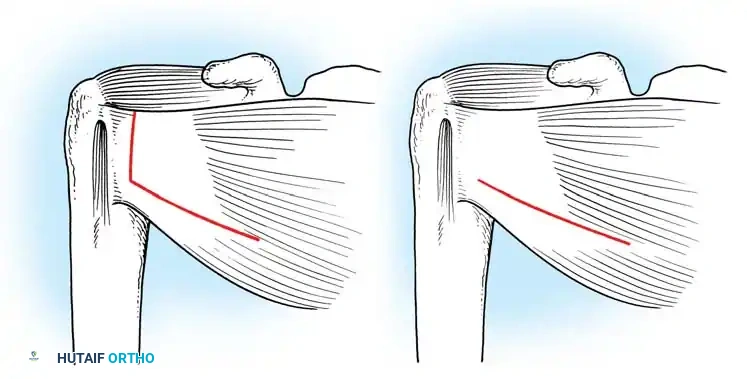
Exposure of the anterior capsule requires navigating the subscapularis muscle. Historically, a vertical tenotomy was performed; however, modern techniques favor a subscapularis split or a peel to preserve the integrity of the muscle belly and its tendinous insertion.
- The Split: A horizontal split is made in the subscapularis at the junction of its middle and inferior thirds, extending from the lesser tuberosity medially.
- Separation: The subscapularis is carefully elevated off the underlying anterior joint capsule. This plane can be scarred in revision cases, requiring meticulous sharp dissection to avoid inadvertent capsulotomy.
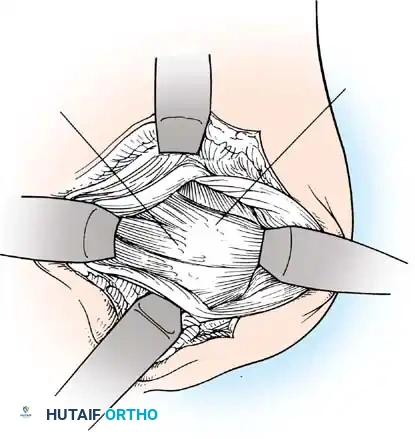
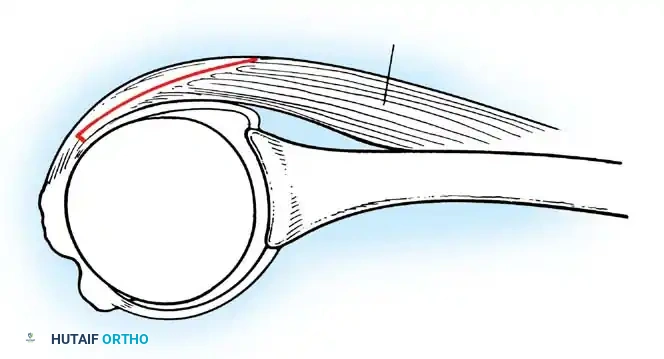
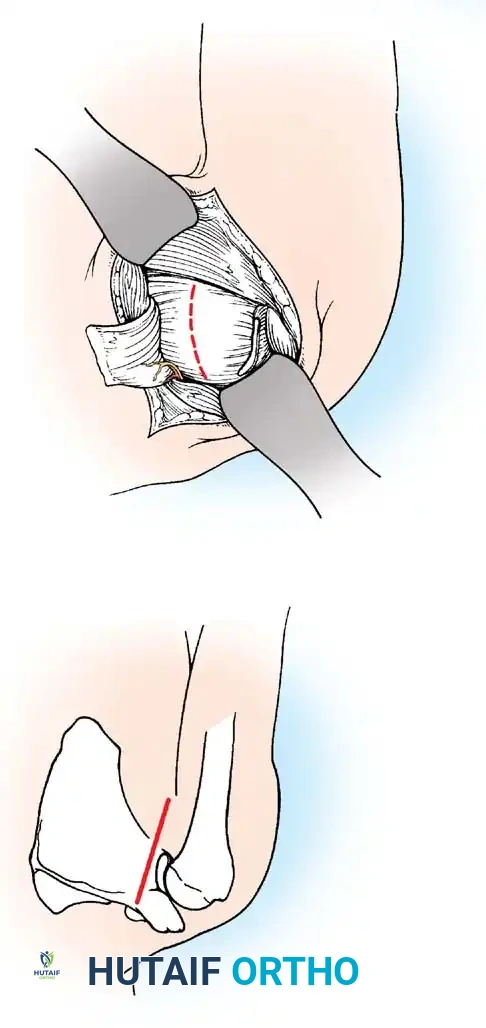
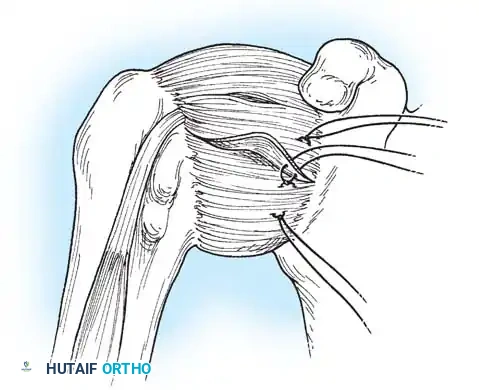
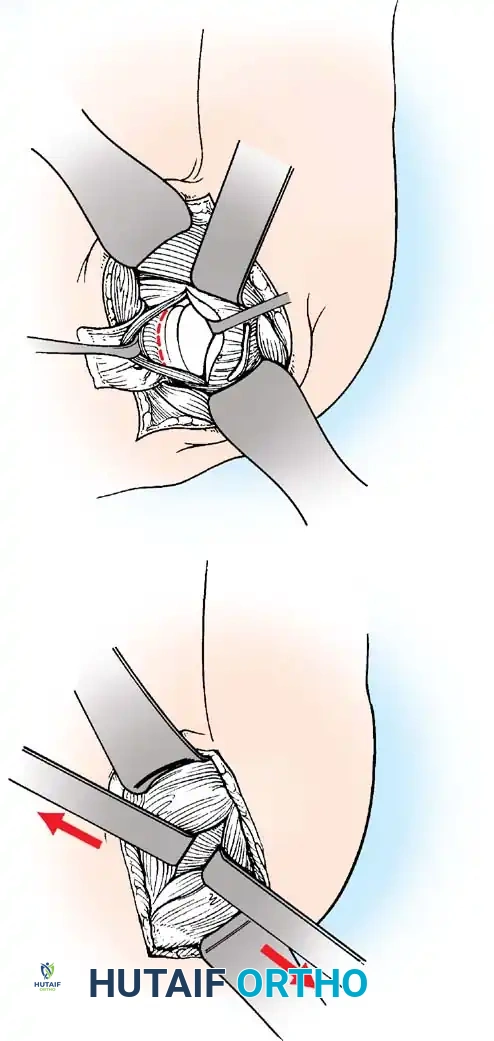
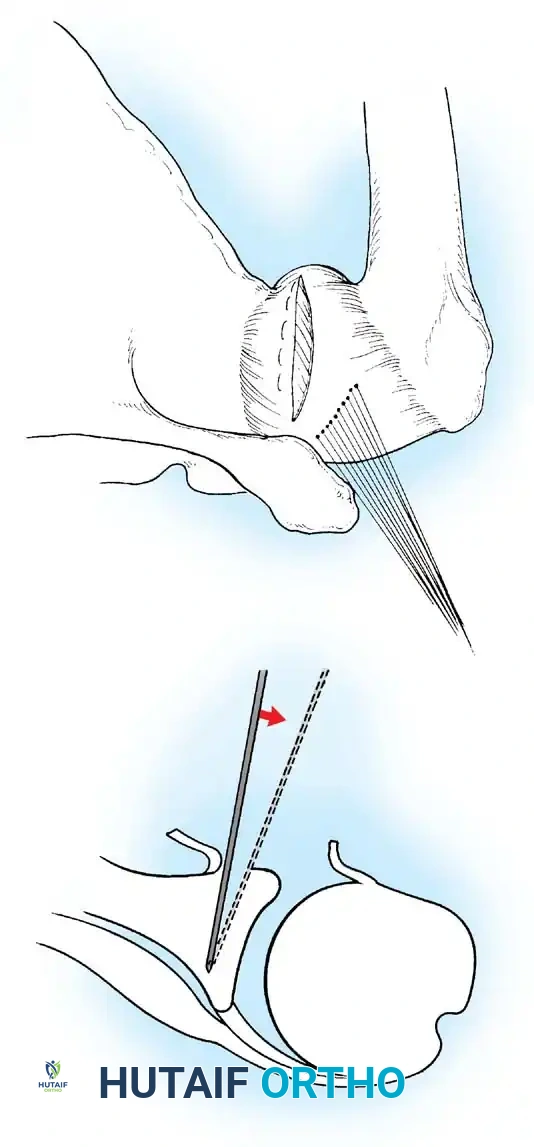
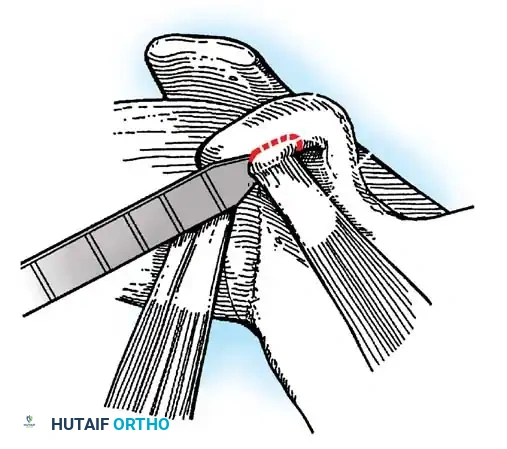
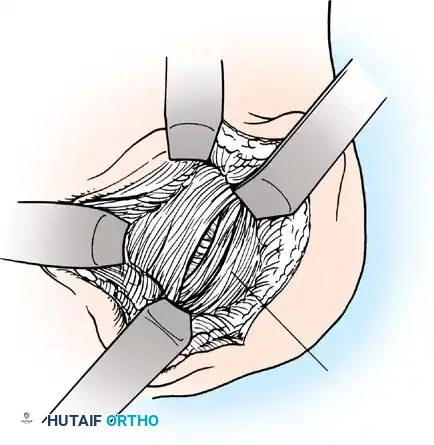
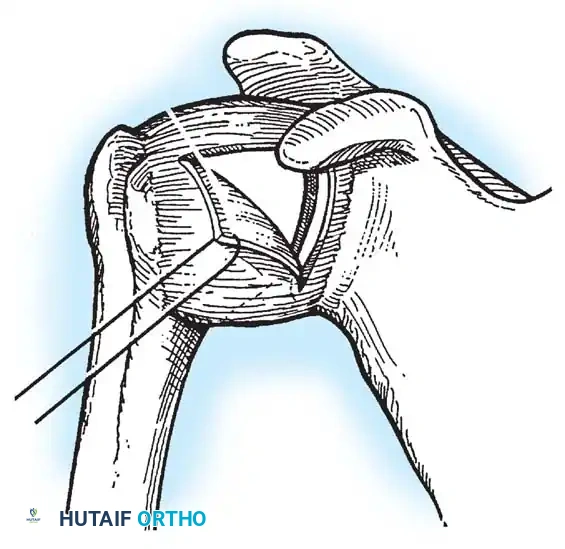
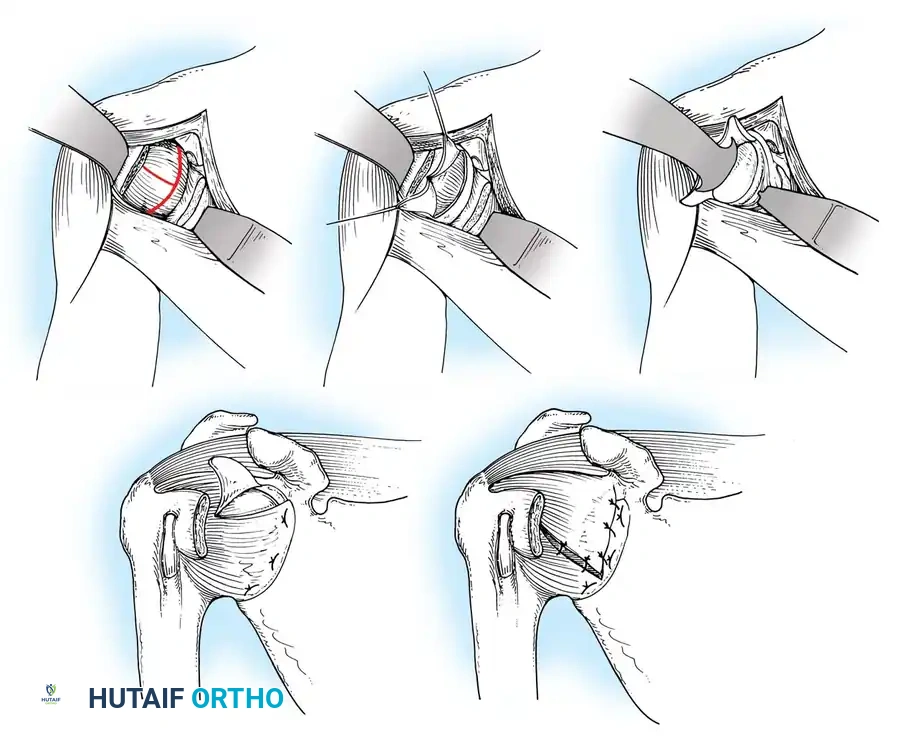
Capsulotomy and Joint Inspection
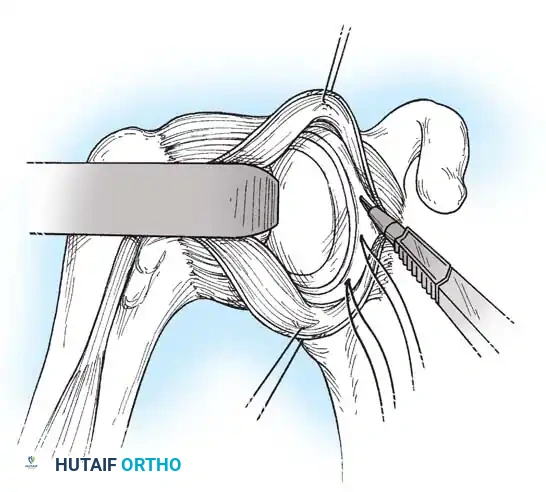
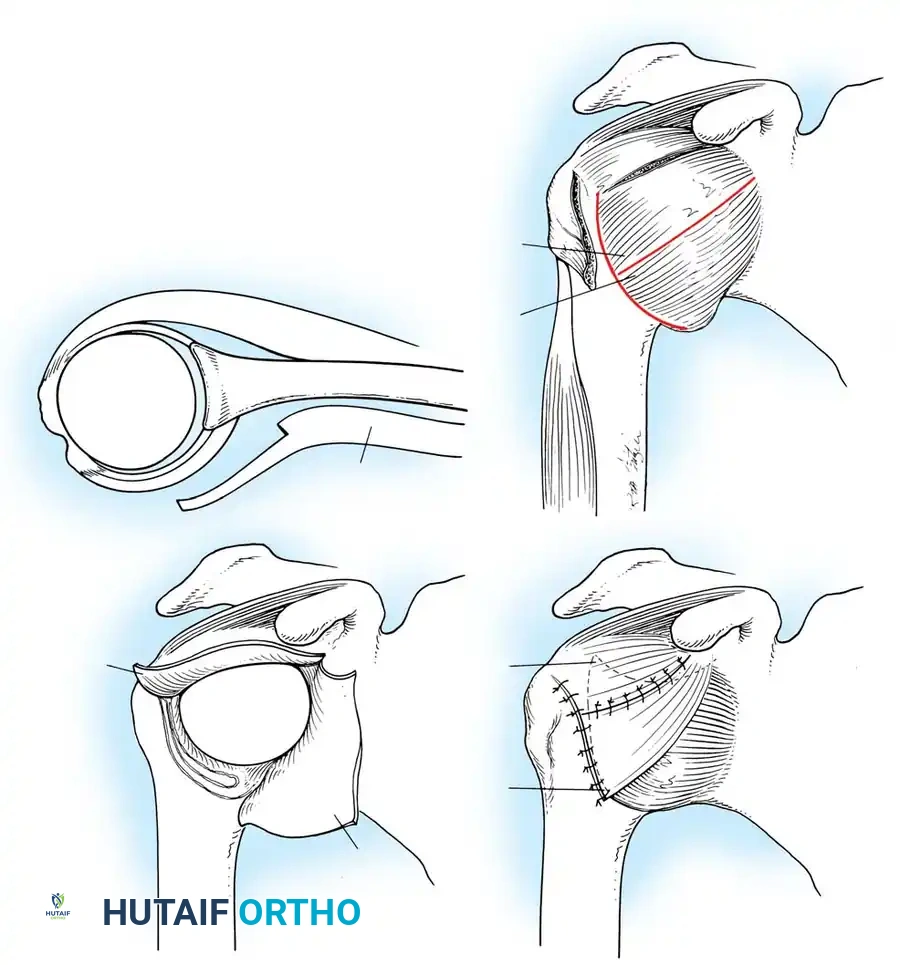
A vertical or T-shaped capsulotomy is performed based on the degree of capsular laxity and the planned shift.
- For a standard Bankart repair with an inferior capsular shift, a vertical incision is made 1 cm medial to the humeral articular margin. A horizontal limb can be added to create superior and inferior capsular flaps.
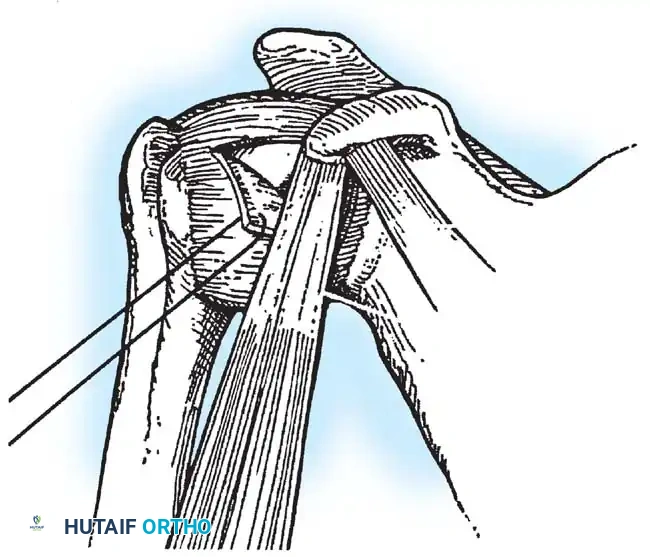
- Tagging sutures are placed in the capsular flaps for traction.
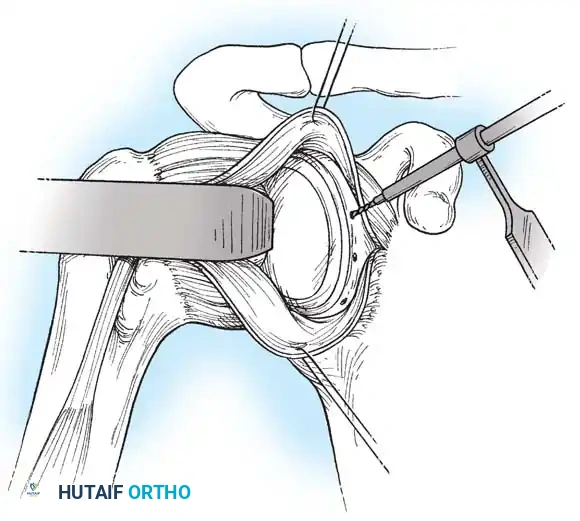
- A Fukuda retractor is placed within the joint to retract the humeral head laterally and posteriorly, exposing the anterior glenoid rim and labrum.
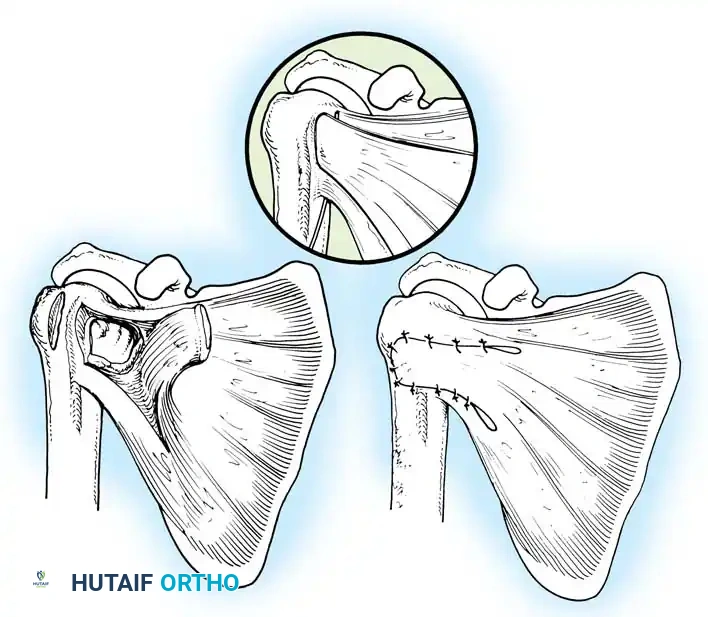
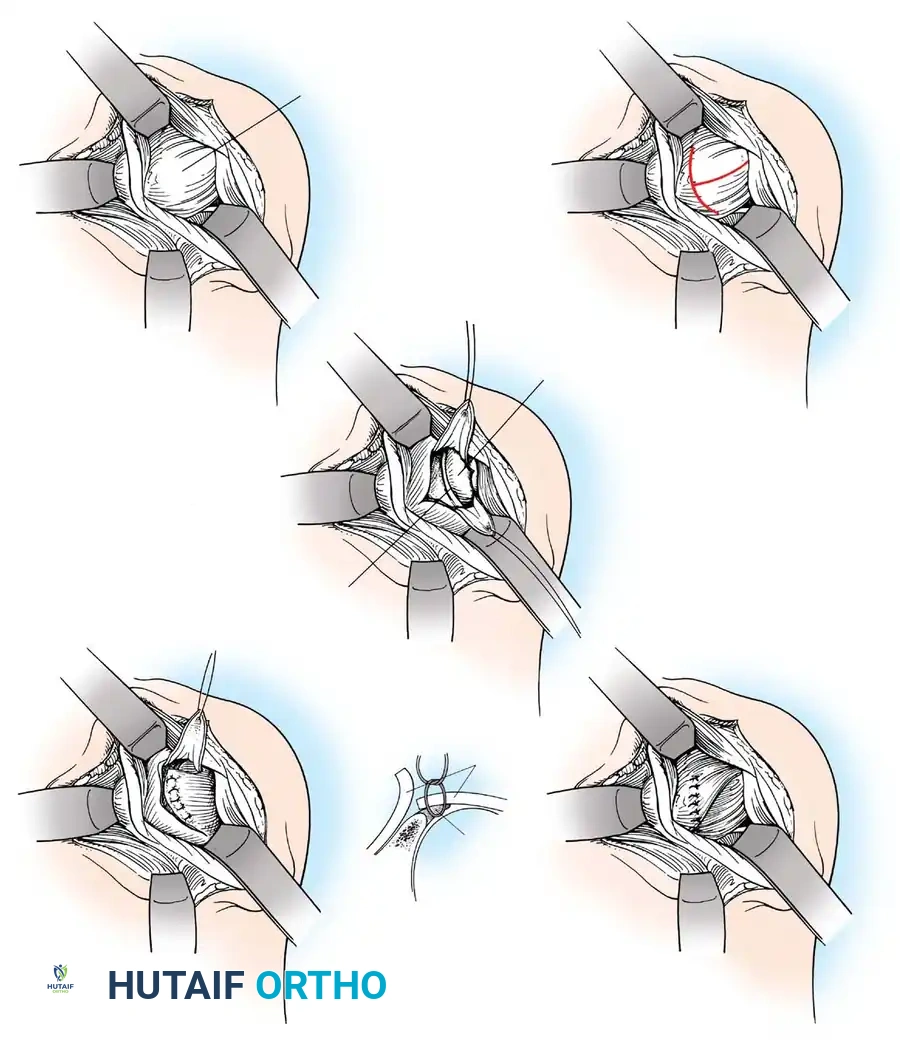
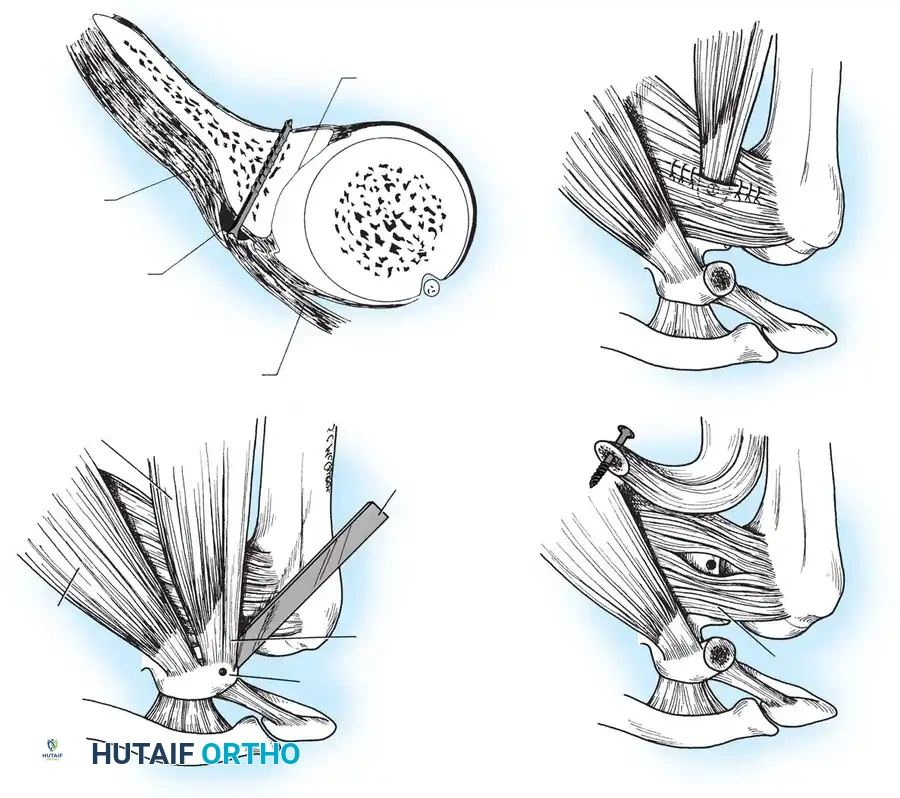
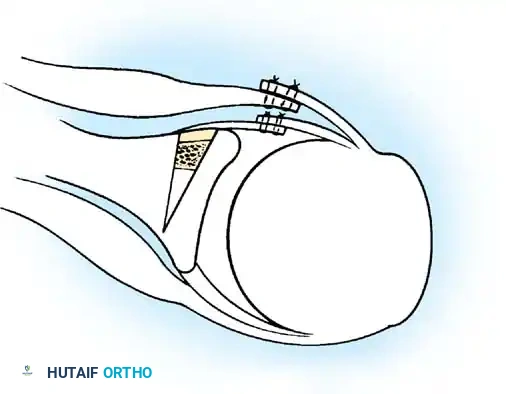
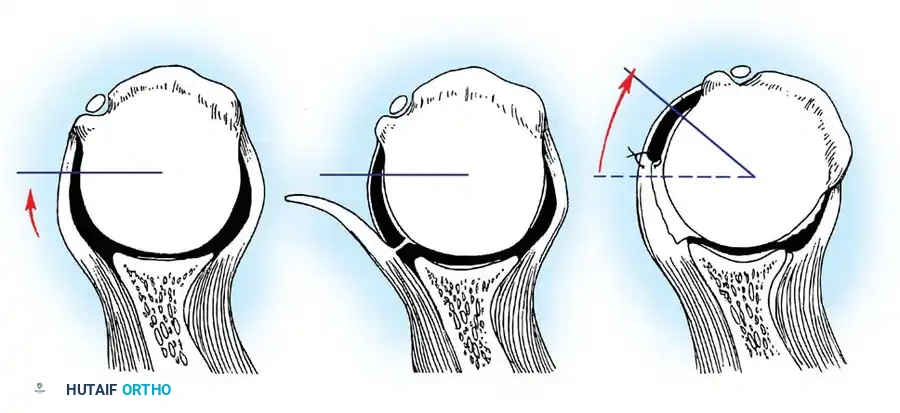
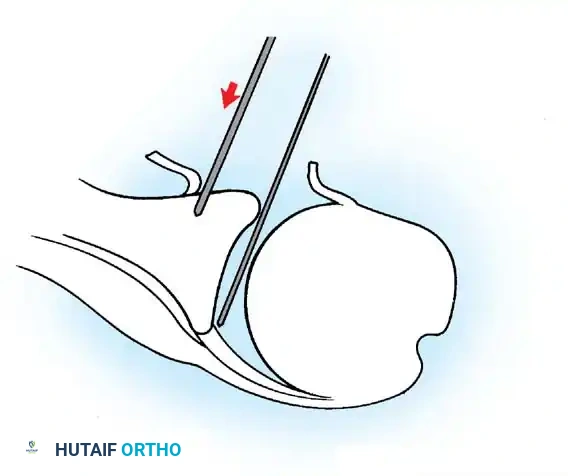
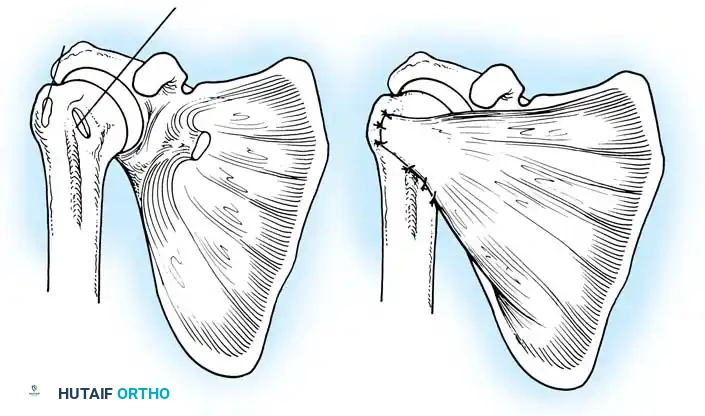
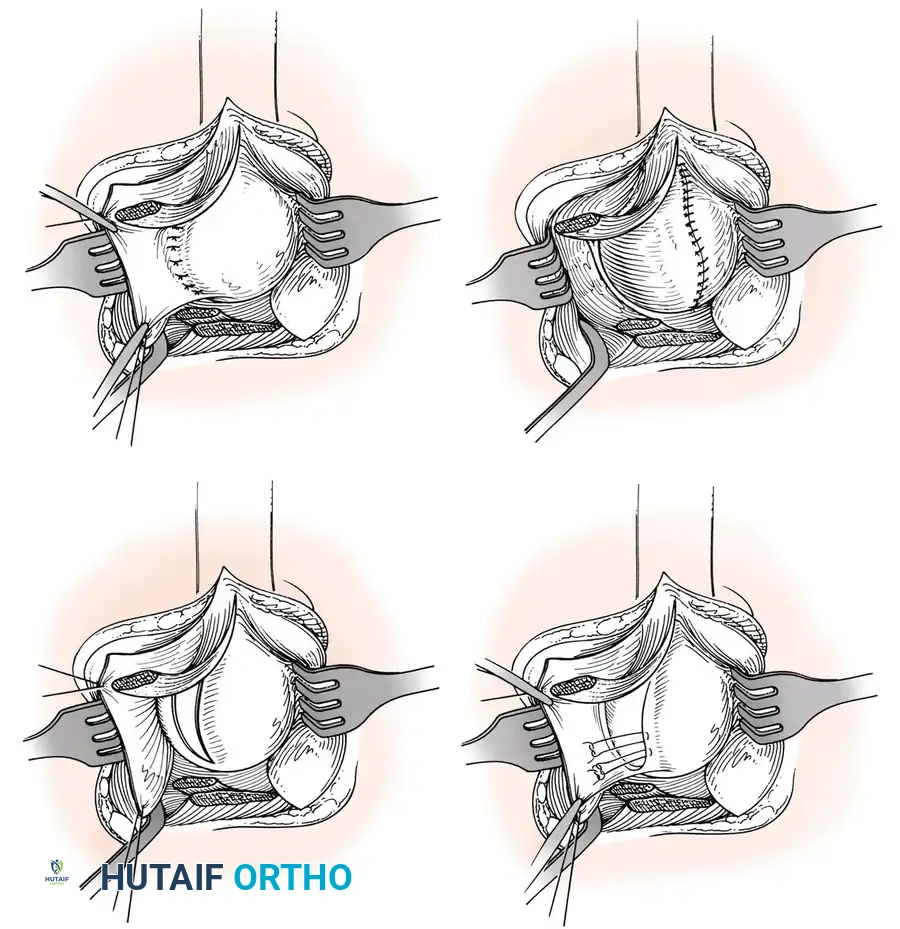
Glenoid Preparation and Labral Repair
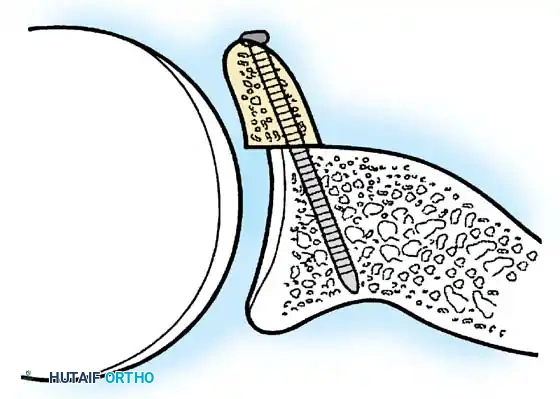
The essential step in restoring stability is the anatomical reduction of the capsulolabral complex to a bleeding bone bed on the anterior glenoid rim.
- Debridement: The anterior glenoid neck is decorticated using a motorized burr, rasp, or osteotome to create a bleeding cancellous bed. This promotes robust biological healing of the repaired labrum.
- Mobilization: The scarred, medially displaced labrum (ALPSA lesion) must be fully mobilized using a periosteal elevator until the subscapularis muscle belly is visible anteriorly. The tissue must float freely to be shifted superiorly and laterally.
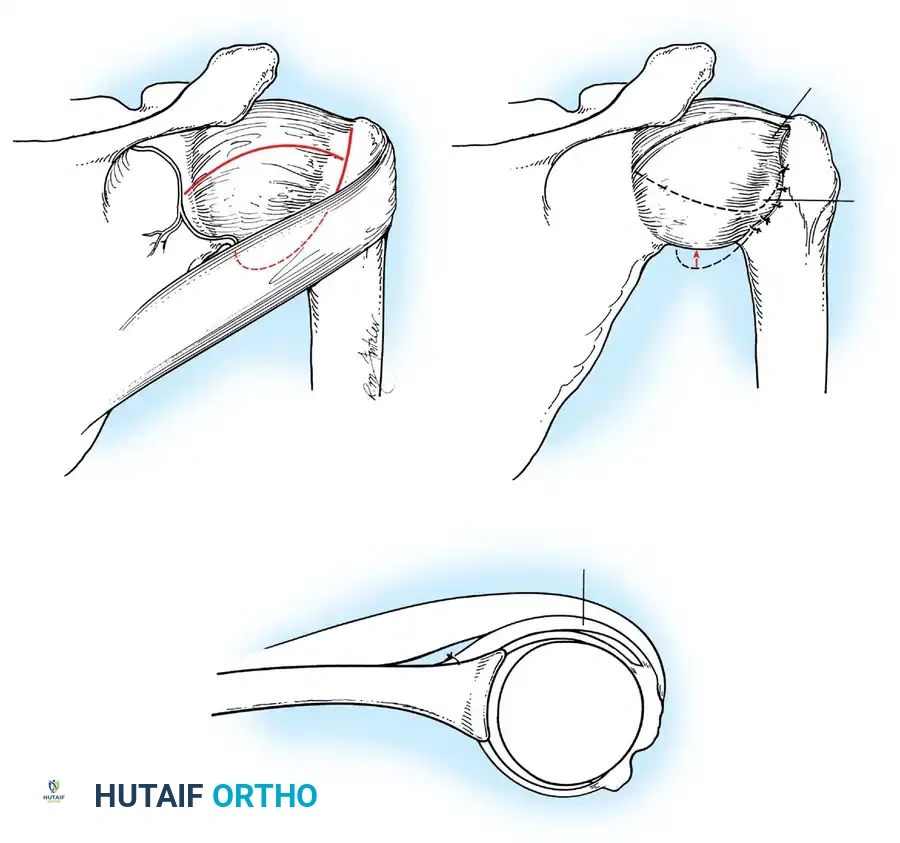
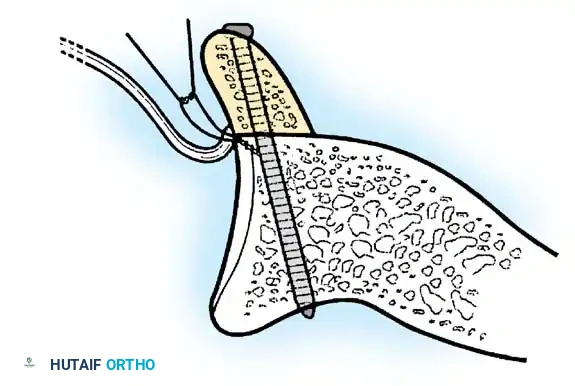
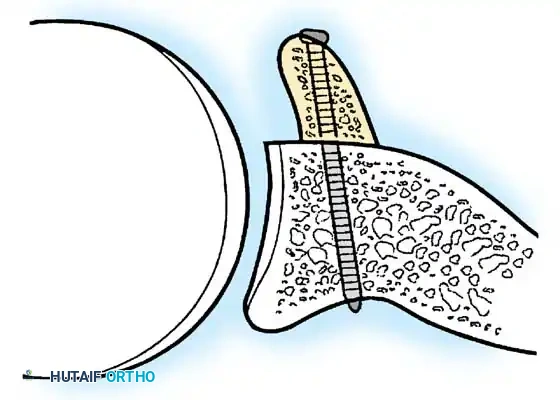
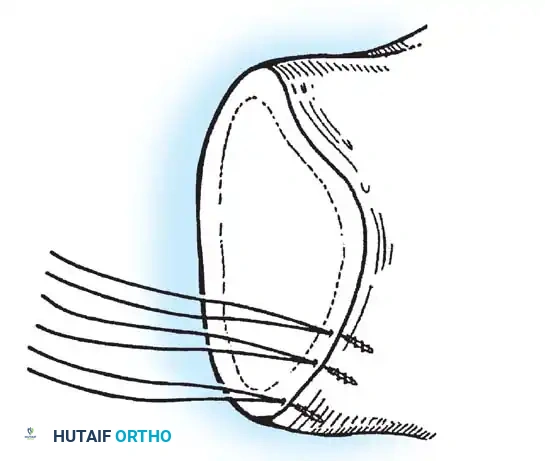
- Anchor Placement: Suture anchors (typically 3 to 4) are placed along the articular margin of the anteroinferior glenoid (from the 5:30 to 3:00 positions for a right shoulder). Anchors must be inserted at a 45-degree angle to the articular surface to maximize pullout strength and avoid joint penetration.
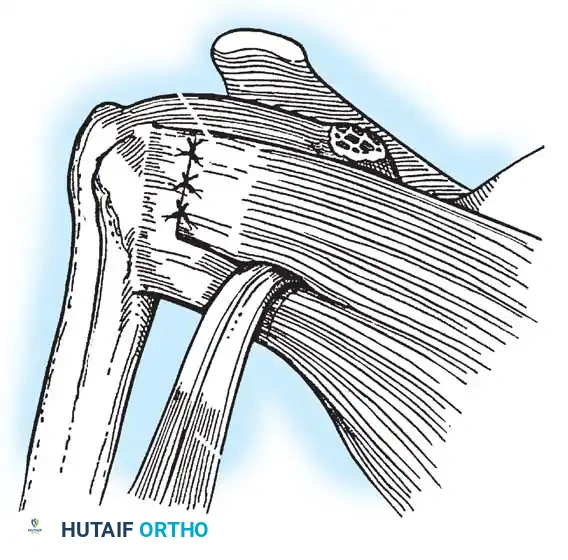
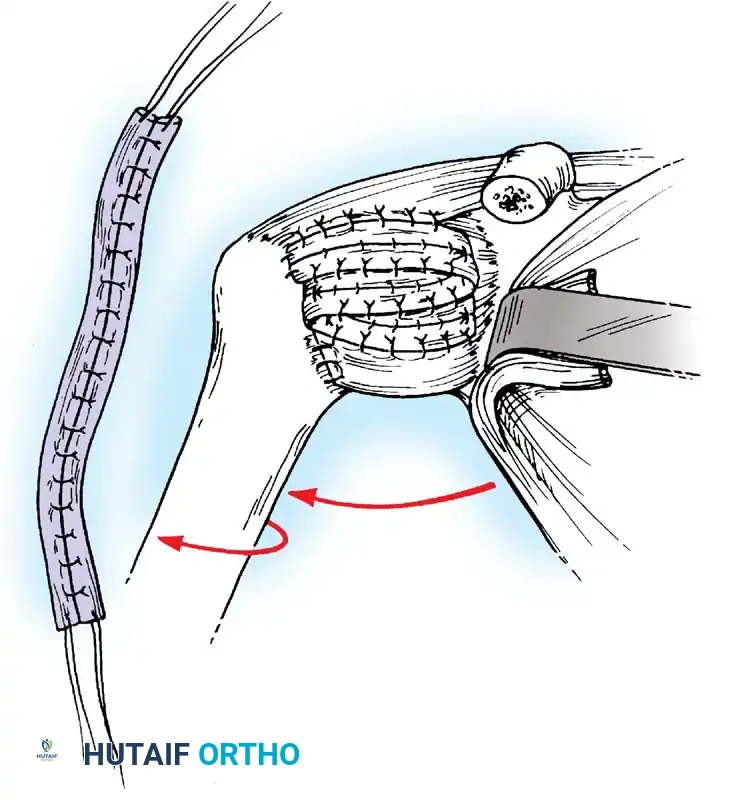
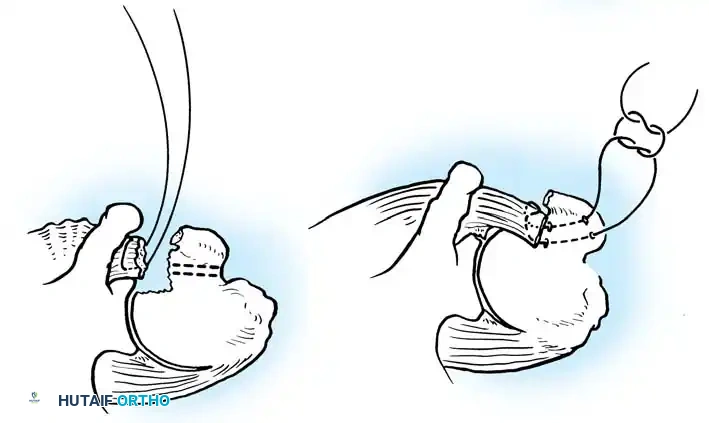
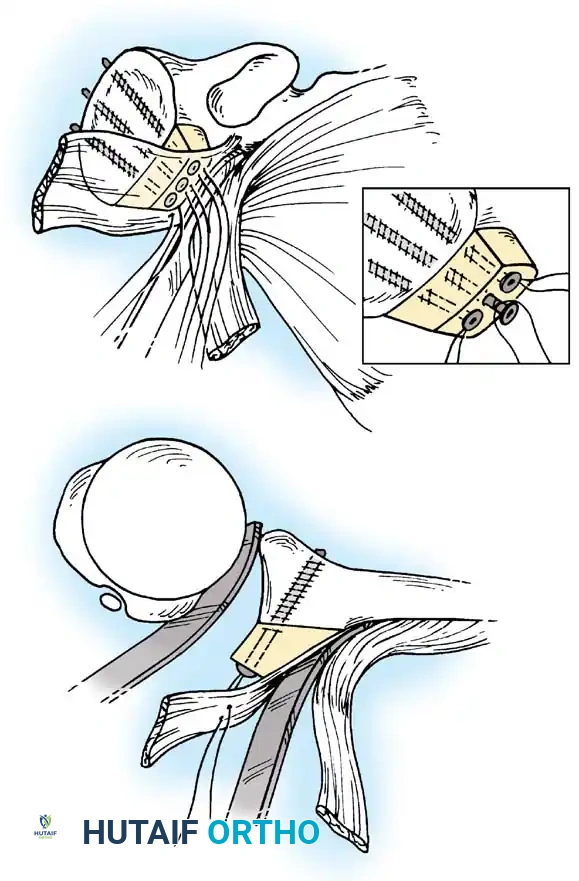
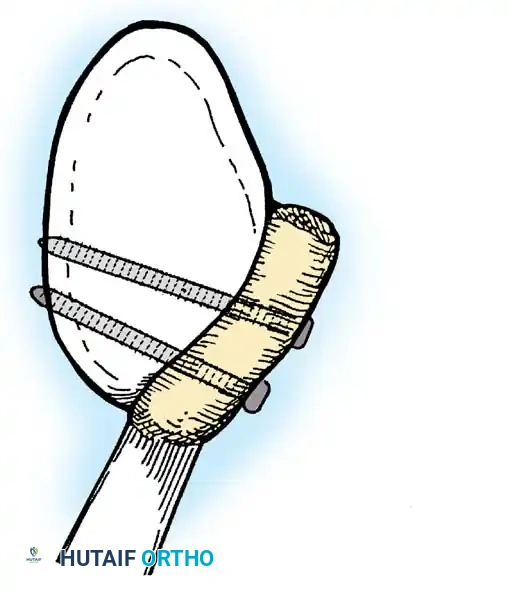
Capsular Shift and Closure
To address capsular redundancy, an inferior capsular shift is performed.
- The arm is positioned in 30 to 45 degrees of abduction and 20 degrees of external rotation.
- The inferior capsular flap is advanced superiorly and laterally, tensioning the IGHL complex. The sutures from the anchors are passed through the shifted capsule and tied.
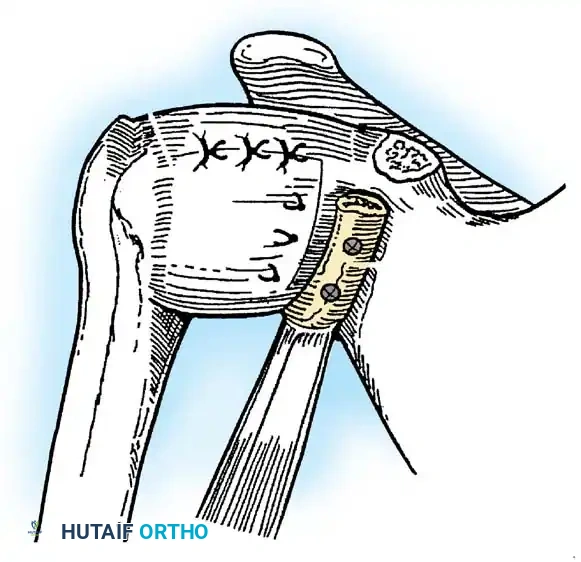
- The superior flap is then brought down over the inferior flap in a "pants-over-vest" fashion to reinforce the anterior wall and close the rotator interval.
- The subscapularis split is loosely approximated with absorbable sutures. The deltopectoral interval is closed over a suction drain (if necessary), followed by routine subcutaneous and skin closure.
Postoperative Protocol and Rehabilitation
Successful surgical stabilization is heavily reliant on a structured, phased rehabilitation program that protects the healing capsulolabral tissues while preventing debilitating stiffness.
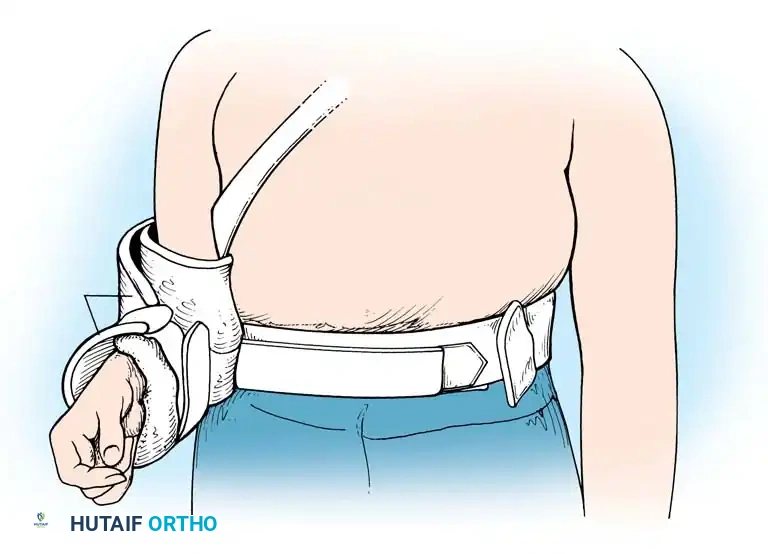
Phase I: Protection (Weeks 0-4)
* The shoulder is immobilized in a sling, often with a small abduction pillow to relieve tension on the superior repair.
* Pendulum exercises and passive forward elevation (up to 90 degrees) are initiated.
* External rotation is strictly limited to neutral (0 degrees) to protect the anterior capsular repair and subscapularis.
Phase II: Intermediate Motion (Weeks 4-8)
* The sling is discontinued.
* Active-assisted and active range of motion begins.
* External rotation is gradually progressed (e.g., 30 degrees by week 6, full by week 8).
* Scapular stabilizer strengthening (rhomboids, trapezius) is emphasized to restore synchronous glenohumeral rhythm.
Phase III: Strengthening (Weeks 8-12)
* Isotonic strengthening of the rotator cuff and deltoid begins.
* Proprioceptive neuromuscular facilitation (PNF) exercises are integrated to restore dynamic joint stability.
Phase IV: Return to Play (Months 4-6)
* Sport-specific drills are introduced.
* Return to contact sports is generally permitted at 5 to 6 months postoperatively, provided the patient has achieved full, painless range of motion, symmetrical strength, and negative apprehension signs.
In conclusion, the management of shoulder instability demands a meticulous evaluation of both static and dynamic restraints. By accurately identifying the specific pathological anatomy—whether it be a classic Bankart lesion, capsular redundancy, or critical bone loss—the orthopedic surgeon can execute a tailored, biomechanically sound reconstruction that restores the delicate balance between mobility and stability.
Associated Surgical & Radiographic Imaging