Scapula Fractures: Discussion the Correct Path to Recovery
Introduction & Epidemiology
Scapula fractures represent a relatively uncommon injury, accounting for approximately 1% of all fractures and 3-5% of shoulder girdle injuries. Their infrequent occurrence is primarily due to the scapula's protected anatomical position, enveloped by a substantial musculature envelope (serratus anterior, subscapularis, infraspinatus, supraspinatus, teres major/minor, deltoid) and cushioned by the chest wall. Consequently, these fractures are typically indicative of high-energy trauma, necessitating a comprehensive trauma evaluation for associated injuries.
The mechanism of injury is usually blunt force trauma, such as motor vehicle accidents, falls from height, or direct blows. Given the significant forces involved, a high index of suspicion for concomitant injuries is paramount. Common associated injuries, often occurring in 80-90% of cases, include:
* Pulmonary contusions, pneumothorax, hemothorax
* Rib fractures
* Brachial plexus injuries
* Head injuries
* Splenic rupture
* Ipsilateral upper extremity fractures (clavicle, humerus, glenoid labrum)
* Vertebral fractures
The presence of a scapula fracture is sometimes termed "the body's seatbelt sign" due to its association with severe torso trauma. A meticulous diagnostic workup is essential to identify and address all potential life-threatening and limb-threatening injuries prior to definitive scapular fracture management.
Classification systems aid in describing fracture patterns and guiding treatment decisions. The most commonly utilized include:
*
AO/OTA Classification:
A comprehensive system detailing fracture location (body, spine, neck, glenoid, acromion, coracoid) and morphology.
*
Ideberg Classification:
Specifically for glenoid fossa fractures, categorizing them from Type I (anterior rim) to Type VI (combination with scapular body).
*
Orthopaedic Trauma Association (OTA) Classification:
A broader system that groups scapula fractures under 14-C.
Understanding these classifications is critical for accurate communication, prognostic assessment, and surgical planning among orthopedic trauma specialists.
Surgical Anatomy & Biomechanics
A thorough understanding of scapular anatomy and biomechanics is fundamental for optimal management of these complex fractures.
Surgical Anatomy
The scapula is a triangular flat bone positioned on the posterolateral aspect of the chest wall, articulating with the humerus at the glenoid fossa and with the clavicle at the acromioclavicular (AC) joint. Key anatomical regions relevant to fracture patterns and surgical approaches include:
*
Body:
The broad, flat portion, providing attachment for serratus anterior (medial border), subscapularis (anterior surface), infraspinatus (posterior surface), and teres major/minor (lateral border).
*
Spine:
A prominent ridge extending transversely across the posterior surface, terminating laterally as the acromion. It provides attachment for the trapezius and deltoid.
*
Acromion:
The lateral extension of the spine, forming the roof of the shoulder and articulating with the clavicle. It provides attachment for the deltoid and trapezius.
*
Coracoid Process:
A hook-like projection anteriorly, serving as the origin for the short head of the biceps, coracobrachialis, and pectoralis minor, and attachment for the coracoclavicular and coracoacromial ligaments.
*
Glenoid Fossa:
The shallow, pear-shaped articular surface that articulates with the humeral head. Its orientation and integrity are crucial for glenohumeral joint stability and function.
*
Scapular Neck:
The constricted area inferior to the glenoid, connecting it to the scapular body.
Neurovascular Structures of Concern:
*
Suprascapular Nerve:
Originates from the upper trunk of the brachial plexus (C5, C6). It passes through the suprascapular notch (inferior to the superior transverse scapular ligament) to innervate the supraspinatus muscle, then travels around the lateral border of the scapular spine (through the spinoglenoid notch) to innervate the infraspinatus muscle. It is vulnerable during posterior approaches, especially when plating the superior aspect of the scapular spine or neck.
*
Axillary Nerve:
Arises from the posterior cord (C5, C6). It courses through the quadrangular space (bounded by teres major inferiorly, teres minor superiorly, long head of triceps medially, and surgical neck of humerus laterally), innervating the deltoid and teres minor. It is at risk during inferior glenoid and lateral scapular body plating, particularly with a deltoid-splitting approach or when hardware extends laterally.
*
Brachial Plexus:
Located superior to the scapula, its trunks and divisions can be injured by severe displacement of superior scapular fractures or high-energy trauma.
*
Axillary Artery and Vein:
Positioned anterior and inferior to the glenoid, vulnerable during anterior glenoid rim fracture fixation or extreme dissection.
*
Circumflex Scapular Artery:
A branch of the subscapular artery, running along the lateral border of the scapula.
Biomechanics
The scapula's primary biomechanical roles include:
*
Glenohumeral Articulation:
Providing a mobile and stable platform for the humerus, facilitating a wide range of motion. The orientation of the glenoid directly impacts shoulder kinematics.
*
Scapulothoracic Rhythm:
Synchronized movement with the humerus during arm elevation, critical for preserving the subacromial space and optimizing deltoid mechanics.
*
Muscle Attachment:
Serving as a large anchor for 17 muscles, acting as an essential link in the kinetic chain of the upper extremity. These muscles contribute significantly to shoulder stability, strength, and proprioception.
Fractures of the scapula disrupt these biomechanical functions. Displaced glenoid fractures directly compromise articular congruity and lead to instability. Scapular neck fractures with significant angulation alter glenoid orientation, impacting rotator cuff efficiency and potentially leading to impingement. Body fractures, while often stable due to the muscle envelope, can affect the lever arm of muscles and contribute to long-term pain and dysfunction if grossly displaced. The muscle envelope can, however, also contribute to fracture displacement due to unopposed muscle pull, particularly in certain patterns.
Indications & Contraindications
The decision for operative versus non-operative management of scapula fractures is complex and depends on multiple factors, including fracture location, displacement, articular involvement, patient comorbidities, and associated injuries.
Non-Operative Management
The majority of scapula body fractures are amenable to non-operative treatment due to the substantial soft tissue envelope providing inherent stability.
*
Indications:
* Minimally displaced scapular body fractures (<1 cm displacement).
* Minimally displaced scapular neck fractures with <40 degrees of angulation and <1 cm translation.
* Stable glenoid rim fractures (Ideberg Type I) with minimal displacement (<5 mm) and no evidence of glenohumeral instability.
* Acromial and coracoid fractures without significant displacement or impingement.
* Patients with significant medical comorbidities precluding surgery.
* Severe polytrauma patients where the scapula fracture is not life- or limb-threatening and operative intervention would unduly prolong critical care.
*
Treatment:
Immobilization in a sling for 2-4 weeks, followed by early gentle range of motion exercises as pain allows.
Operative Management
Surgical intervention is generally reserved for fractures that significantly compromise shoulder function, stability, or pain control. The goal is anatomical reduction and stable internal fixation.
-
Indications:
-
Glenoid Fractures:
- Articular step-off >2-3 mm.
- Glenoid instability (e.g., in Ideberg Type II-V fractures with significant displacement or subluxation/dislocation of the humeral head).
- Glenoid rim fractures involving >25% of the articular surface.
- Open fractures.
-
Scapular Neck Fractures:
- Angulation >40 degrees.
- Medial/lateral displacement >1 cm.
- Disruption of the superior shoulder suspensory complex (SSSC), leading to a "floating shoulder" (fracture of ipsilateral clavicle and glenoid neck/scapular body). While some floating shoulders are treated non-operatively, displaced patterns often benefit from fixation to restore shoulder girdle integrity.
-
Scapular Body Fractures:
- Severe displacement (>2 cm).
- Gross rotational malalignment impacting scapulothoracic motion.
-
Acromion Fractures:
- Displacement causing subacromial impingement (>1 cm).
- AC joint instability.
-
Coracoid Fractures:
- Significant displacement (>1 cm) or involvement of the coracoclavicular ligaments, causing AC joint instability.
- Neurological impingement (rare).
-
Glenoid Fractures:
-
Contraindications:
- Severe overlying soft tissue compromise (e.g., large degloving injury, severe burns).
- Active infection.
- Unstable medical comorbidities or patient unfit for anesthesia/surgery.
- Extremely comminuted fractures where stable fixation is unlikely to be achieved.
Summary Table: Operative vs. Non-Operative Indications
| Feature | Non-Operative Indications | Operative Indications |
|---|---|---|
| Scapular Body | Minimally displaced (<1 cm) | Gross displacement (>2 cm), significant rotational malalignment |
| Scapular Neck | Angulation <40°, translation <1 cm | Angulation >40°, translation >1 cm, displaced "floating shoulder" |
| Glenoid Fossa | Articular step-off <2-3 mm, stable, <25% articular involvement | Articular step-off >2-3 mm, glenohumeral instability, >25% articular involvement |
| Acromion | Nondisplaced, no impingement | Displacement >1 cm causing impingement, AC joint instability |
| Coracoid | Nondisplaced, stable AC joint | Displacement >1 cm, associated AC joint instability, neurological impingement (rare) |
| Associated Injuries | None requiring urgent surgical intervention | Displaced "floating shoulder" (clavicle + scapula neck/body fracture) |
| Patient Factors | Significant comorbidities, polytrauma not requiring urgent scapula fixation | Fit for surgery, younger active patients, desire for optimal shoulder function |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is crucial for successful outcomes in scapula fracture surgery, given the complex anatomy, vital neurovascular structures, and potential for associated injuries.
Pre-Operative Planning
-
Imaging Review:
- Standard Radiographs: Anteroposterior (AP), Y-view (scapular lateral), and axillary views are initial staples. These help characterize the basic fracture pattern and assess displacement.
-
Computed Tomography (CT) Scan:
This is indispensable.
CT with 3D reconstructions (including coronal, sagittal, and axial cuts) provides the most comprehensive evaluation of the fracture morphology, articular involvement, displacement, angulation, and comminution. It is critical for glenoid fractures (Ideberg classification) and for identifying associated fractures not evident on plain radiographs.
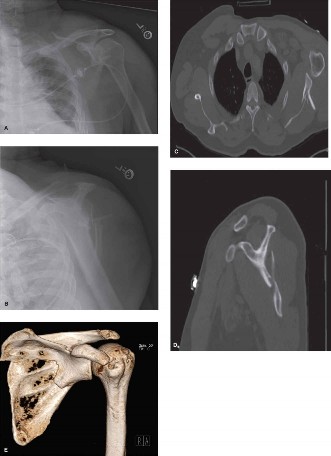
-
- Figure 1: Pre-operative CT scan with 3D reconstruction demonstrating a complex scapular body and neck fracture with significant displacement and angulation. Such detailed imaging is critical for accurate surgical planning and identifying the optimal approach.
-
- Magnetic Resonance Imaging (MRI): Rarely indicated acutely for fracture planning, but can be useful to assess rotator cuff integrity or brachial plexus involvement if suspected.
- Associated Injury Assessment: Reconfirm and review all associated injuries, ensuring they are managed appropriately. This may involve multidisciplinary consultations (neurosurgery, general surgery, thoracic surgery).
- Neurovascular Status: A thorough pre-operative neurovascular examination is mandatory, documenting motor and sensory function, and distal pulses. Baseline documentation is vital for post-operative comparison.
- Surgical Approach Selection: Based on the fracture pattern and 3D CT analysis, select the optimal surgical approach. Posterior (Judet) approaches are most common, but anterolateral, superior, or combined approaches may be necessary.
- Implant Selection: Plan for appropriate plate and screw constructs (e.g., 2.7mm, 3.5mm locking/non-locking plates, lag screws) to achieve stable fixation for the specific fracture pattern. Ensure a range of plate lengths and types are available.
- Surgeon Experience: Given the complexity, these surgeries are best performed by experienced orthopedic trauma surgeons.
Patient Positioning
Proper patient positioning is paramount for adequate exposure, fracture reduction, and protection of neurovascular structures.
1.
Lateral Decubitus Position:
*
Advantages:
Excellent exposure of the posterior scapula (glenoid, neck, body, spine). Allows for easy arm manipulation by an assistant to facilitate fracture reduction and assess glenohumeral stability. Often preferred for posterior approaches.
*
Setup:
Patient placed on their unaffected side. Axillary roll positioned to protect the contralateral brachial plexus. The affected arm is prepped free. Beanbag or specific positioning devices used for stability. Adequate padding for pressure points (fibular head, olecranon, dependent arm).
2.
Prone Position:
*
Advantages:
Also provides good exposure for posterior approaches. Avoids the need for an axillary roll.
*
Setup:
Patient is prone on a radiolucent table. Chest rolls or a specialty frame (e.g., Wilson frame) are used to allow free abdominal excursion and prevent diaphragmatic splinting. Head is positioned to avoid pressure on eyes and ears. Affected arm is prepped free, often draped over an arm board.
*
Disadvantages:
Arm manipulation can be more challenging compared to lateral decubitus, potentially hindering reduction maneuvers or assessment of glenohumeral stability.
3.
Beach Chair Position:
* Rarely used for extensive scapular fracture ORIF due to limited posterior access. May be considered for superior acromion or anterior coracoid fixation, or when an anterior approach is predominantly required (e.g., specific anterior glenoid rim fractures).
*
Setup:
Similar to arthroscopy positioning, ensuring appropriate head and neck support.
Regardless of the chosen position, thorough padding, meticulous draping, and careful monitoring of vital signs and potential pressure points are critical throughout the procedure. Fluoroscopy should be readily available and draped for intraoperative imaging.
Detailed Surgical Approach / Technique
Surgical treatment of scapula fractures aims for anatomical reduction of articular surfaces, restoration of glenoid orientation, and stable fixation to allow early functional rehabilitation. The choice of surgical approach depends on the fracture pattern and location.
General Principles
- Associated Injury Management: Address life-threatening injuries first.
- Timing: Definitive fixation can be delayed until soft tissue swelling subsides (usually 7-10 days), especially in polytrauma patients, unless neurovascular compromise or open fracture dictates emergent intervention.
- Anatomic Reduction: Crucial for articular fractures; anatomical or near-anatomical reduction for neck and body fractures to restore glenoid version and translation.
- Stable Fixation: Employ small fragment plates (2.7mm, 3.5mm) and screws, often locking, to create a stable construct capable of withstanding early rehabilitation forces. Bicortical screw purchase is generally preferred.
- Neurovascular Protection: Meticulous dissection and careful use of retractors are essential to protect the suprascapular and axillary nerves.
Surgical Approaches and Techniques
1. Posterior Approaches (Judet Approaches)
These are the workhorse approaches for fractures of the glenoid, scapular neck, spine, and body.
A. Posterior Approach (Judet): Deltoid-Splitting / Infraspinatus-Splitting
*
Incision:
A curvilinear or straight incision is made from the posterior aspect of the acromion, extending distally along the scapular spine, then curving inferomedially along the medial border of the scapula. The length depends on the fracture extent.
*
Layered Dissection:
1.
Skin and Subcutaneous Tissue:
Elevate full-thickness skin flaps.
2.
Fascia:
Incise the fascia overlying the deltoid and trapezius.
3.
Deltoid-Splitting (Proximal Exposure):
For fractures involving the glenoid, neck, and proximal body. The deltoid muscle fibers are carefully split in line with their fibers, originating from the scapular spine. The interval between the deltoid and infraspinatus is developed. Care must be taken to avoid violating the axillary nerve, which lies approximately 5-7 cm distal to the acromion tip.
4.
Internervous Plane (Main Exposure):
The primary internervous plane for accessing the posterior scapula lies between the
deltoid
(innervated by the axillary nerve) and the
infraspinatus
(innervated by the suprascapular nerve).
* The deltoid is elevated off the scapular spine laterally.
* The infraspinatus is elevated off the posterior aspect of the scapular body, revealing the bone. This elevation is performed subperiosteally.
5.
Supraspinatus (Proximal Exposure):
To expose the superior glenoid, neck, and suprascapular notch, the supraspinatus can be elevated from the supraspinous fossa. Extreme caution is needed to protect the suprascapular nerve as it enters the fossa via the suprascapular notch.
6.
Teres Minor (Inferior Exposure):
The interval between the infraspinatus and teres minor can be developed for more inferior body/neck exposure. The axillary nerve passes deep to the teres minor at the quadrangular space.
*
Glenoid Exposure:
*
Posterior Rim:
Direct visualization is typically good.
*
Anterior Glenoid and Articular Surface:
Requires more extensive soft tissue release, often involving partial capsular incision. Use a posterior Hohmann retractor around the glenoid neck to expose the articular surface. The arm is internally rotated to bring the glenoid into view.
*
Reduction and Fixation:
1.
Indirect Reduction:
Initial gentle traction on the arm may aid in partial reduction via ligamentotaxis.
2.
Direct Reduction:
Use pointed reduction clamps, bone hooks, or K-wires as joysticks to manipulate fracture fragments. Temporary K-wire fixation can hold reduction.
3.
Glenoid Fractures:
* Anatomic reduction of the articular surface is paramount.
* Fixation typically involves small fragment screws (2.7mm or 3.5mm) oriented perpendicular to the fracture line (lag screw technique) or small plates (e.g., 2.7mm locking plates) as buttress plates.
* Consider the trajectory of screws to avoid joint penetration (fluoroscopic control essential).
4.
Scapular Neck Fractures:
* Restore the length, angulation, and version of the glenoid.
* Fixation often involves a contoured 3.5mm locking plate placed along the lateral border of the scapula, extending onto the glenoid neck and scapular body. Another plate can be placed along the scapular spine for additional stability, creating an angle or "L" construct.
5.
Scapular Body Fractures:
* Reduction focuses on restoring overall scapular morphology and preventing significant angulation.
* Plate fixation typically uses 3.5mm locking plates bridging the comminution or providing compression. Longer plates are preferred to distribute stress.
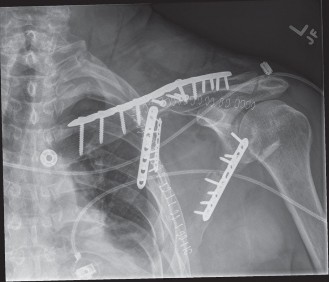
*
*
Figure 2: Intraoperative image demonstrating stable internal fixation of a scapular neck and body fracture with a contoured locking plate along the lateral border of the scapula. Note the screw trajectories and soft tissue protection.
6.
Acromion Fractures:
* If displaced and causing impingement, reduction and fixation with small plates, tension band wiring, or screws may be used.
7.
Coracoid Fractures:
* Accessed via an anterolateral approach (deltopectoral) for displaced fractures. Fixation with small screws or plates.
2. Anterolateral / Deltopectoral Approach
- Indications: Fractures of the coracoid, anterior glenoid rim, or when combined with clavicle fixation in a "floating shoulder" injury.
- Incision: A curvilinear incision extending from the coracoid process inferiorly along the deltopectoral groove.
- Internervous Plane: Between the deltoid (axillary nerve) and pectoralis major (medial and lateral pectoral nerves).
- Dissection: Identify the cephalic vein, which can be retracted medially or laterally. Ligate and divide perforating vessels. Retract the deltoid laterally and pectoralis major medially. The coracoid process and its attachments are visualized. For anterior glenoid exposure, further dissection inferiorly and laterally through the subscapularis tendon or capsule is required. Care must be taken to protect the musculocutaneous nerve (entering the coracobrachialis) and the axillary nerve (posterior to the joint capsule).
3. Superior Approach
- Indications: Isolated acromial fractures, superior glenoid rim fractures.
- Incision: Transverse incision over the acromion or curved incision along the spine to the acromion.
- Dissection: Careful dissection through the deltoid and trapezius attachments. Protection of the suprascapular nerve (which passes medially to the acromial base) is crucial.
Intraoperative Fluoroscopy
Essential for confirming reduction and assessing implant placement, especially for glenoid fractures to ensure articular congruity and avoid intra-articular screw penetration.
Wound Closure
Layered closure over a drain if significant dead space is created.
Complications & Management
Despite meticulous surgical technique, complications can occur following scapula fracture fixation. Understanding these potential issues and their management is crucial for optimal patient care.
Common Complications
-
Neurovascular Injury:
- Incidence: Varies, but suprascapular nerve palsy reported in 10-30% of cases, often transient. Axillary nerve injury is less common but more devastating.
- Mechanism: Direct trauma from the fracture fragments, traction injury during reduction maneuvers, entrapment by hardware, or iatrogenic injury during dissection. The suprascapular nerve is particularly vulnerable at the suprascapular and spinoglenoid notches. The axillary nerve is at risk with aggressive retraction or lateral plating.
- Management: Meticulous surgical technique, careful use of retractors, precise screw trajectory, and intraoperative nerve monitoring can mitigate risk. If identified intraoperatively, remove/reposition hardware. Postoperatively, observe for recovery. If no improvement, EMG studies can confirm injury, and nerve exploration may be considered.
-
Infection:
- Incidence: 2-5%.
- Mechanism: Surgical site contamination. Higher risk in open fractures, prolonged surgery, or in immunocompromised patients.
- Management: Prophylactic antibiotics. If superficial, local wound care and oral antibiotics. Deep infections require surgical debridement, intravenous antibiotics, and potentially hardware removal (after fracture healing).
-
Hardware Failure / Prominence:
- Incidence: 5-10%.
- Mechanism: Nonunion, inadequate fixation for early motion, poorly contoured plates, stress shielding. Hardware may become prominent and cause discomfort, especially under thin soft tissue coverage (e.g., along the scapular spine).
- Management: Revision surgery for nonunion or symptomatic hardware. Hardware removal after fracture healing is common if bothersome.
-
Malunion / Nonunion:
- Incidence: Nonunion is rare for scapular body fractures (<1%), but higher for neck/glenoid (up to 5-10% in complex cases). Malunion can occur, particularly with glenoid articular displacement or scapular neck angulation.
- Mechanism: Inadequate reduction, unstable fixation, poor bone biology, persistent instability.
- Management: Asymptomatic malunion may be observed. Symptomatic malunion or nonunion often requires revision surgery with osteotomy, bone grafting, and more robust fixation.
-
Stiffness / Limited Range of Motion:
- Incidence: Common, especially if rehabilitation is delayed or if there's extensive soft tissue scarring.
- Mechanism: Adhesions, capsular contracture, deltoid inhibition.
- Management: Aggressive physical therapy. If conservative measures fail, consider manipulation under anesthesia or arthroscopic/open capsular release.
-
Post-Traumatic Arthritis:
- Incidence: Higher in glenoid articular fractures, particularly with residual step-off or incongruity. Can take years to develop.
- Mechanism: Damage to articular cartilage, altered joint mechanics.
- Management: Initial management is conservative (pain control, activity modification). For severe, symptomatic arthritis, glenohumeral arthroplasty (total shoulder or reverse total shoulder) may be indicated.
-
Chronic Pain:
- Incidence: Variable, can be multifactorial.
- Mechanism: Residual instability, malunion, hardware irritation, nerve injury, myofascial pain.
- Management: Multidisciplinary approach including physical therapy, pain management specialists, and potentially revision surgery to address specific etiologies.
Summary Table: Common Complications & Management
| Complication | Typical Incidence | Salvage Strategies / Management |
|---|---|---|
| Suprascapular Nerve Palsy | 10-30% (often transient) | Observation, EMG studies, nerve exploration if no recovery |
| Axillary Nerve Palsy | <5% | Observation, EMG studies, nerve exploration if no recovery |
| Surgical Site Infection | 2-5% | Debridement, IV antibiotics, hardware removal (if deep and healed) |
| Hardware Prominence | 5-10% | Hardware removal after fracture healing if symptomatic |
| Malunion | Variable | Observation (if asymptomatic), corrective osteotomy, revision fixation |
| Nonunion | <5% (body), 5-10% (neck/glenoid) | Revision ORIF with bone grafting, more stable fixation |
| Stiffness / ROM Loss | Common | Aggressive PT, manipulation under anesthesia, arthrolysis |
| Post-Traumatic Arthritis | Variable (glenoid) | Conservative management, glenohumeral arthropllasty for severe cases |
| Chronic Pain | Variable | PT, pain management, address underlying mechanical issues (e.g., hardware removal) |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a critical component of successful scapula fracture management, aiming to restore range of motion, strength, and function while protecting the surgical repair. Protocols must be individualized based on fracture type, stability of fixation, patient factors, and surgeon preference.
General Principles
- Protection: The initial phase prioritizes protection of the healing fracture and soft tissue repair.
- Gradual Progression: Rehabilitation advances incrementally, guided by pain and tissue healing.
- Pain Management: Adequate pain control is essential for patient compliance with therapy.
- Scapular Stabilization: Emphasis on restoring scapular control and kinematics.
- Communication: Close communication between the surgeon, physical therapist, and patient is vital.
Phases of Rehabilitation
Phase 1: Immobilization and Early Passive Motion (Weeks 0-6)
- Goals: Protect the repair, reduce pain and swelling, prevent stiffness, initiate early passive range of motion.
-
Immobilization:
- Arm placed in a sling for 4-6 weeks (duration depends on fracture stability and surgeon preference).
- No active shoulder motion is allowed.
- Elbow, wrist, and hand active range of motion (ROM) exercises are encouraged to prevent stiffness in these joints.
-
Passive Range of Motion (PROM):
- Pendulum (Codman's) exercises: Gentle, gravity-assisted swings of the arm.
- Assisted PROM: Therapist or contralateral arm assists with glenohumeral flexion (up to 90-120 degrees depending on fixation stability), external rotation (neutral to 30 degrees), and internal rotation.
- Avoid stressing the repair: No forced end-range motion. Avoid abduction beyond 90 degrees if superior plate fixation is used.
- Scapular Mobility: Gentle scapular glides and rhythmic stabilization exercises with passive arm motion.
- Weight-Bearing Restrictions: No weight-bearing on the affected arm.
- Pain and Swelling Management: Ice, elevation, NSAIDs as indicated.
Phase 2: Controlled Active Motion (Weeks 6-12)
- Goals: Gradually restore full active range of motion, begin isometric strengthening, improve scapular control.
-
Progression:
- Discontinue sling (as tolerated, usually by week 6).
- Active-Assisted Range of Motion (AAROM): Progress from PROM to AAROM, then to full active range of motion (AROM) as pain allows. Focus on achieving full flexion, abduction, and rotation.
- Isometric Strengthening: Initiate gentle isometric exercises for rotator cuff (internal/external rotation), deltoid, and scapular stabilizers (rhomboids, serratus anterior, trapezius). These are performed without joint movement.
- Scapular Stabilization: Emphasize exercises to promote proper scapulohumeral rhythm, such as prone scapular protraction/retraction, rowing, and "T" and "Y" exercises.
- Light Functional Activities: Begin light daily activities, avoiding heavy lifting or sudden movements.
Phase 3: Progressive Strengthening (Weeks 12-24)
- Goals: Restore full strength, endurance, and advanced scapular stability.
-
Progression:
- Resisted Strengthening: Progress to isotonic strengthening exercises using resistance bands, light weights, or machine weights. Focus on all major shoulder muscle groups: deltoid, rotator cuff (internal/external rotators, abductors), scapular stabilizers.
- Proprioception and Neuromuscular Control: Incorporate exercises with unstable surfaces (e.g., wobble board) or dynamic balance activities to improve neuromuscular control.
- Endurance Training: Low-resistance, high-repetition exercises.
- Functional Training: Replicate movements specific to the patient's occupation or hobbies.
- Return to Activity: Gradual return to activities requiring more strength and coordination. Avoid overhead lifting, pushing, or pulling heavy objects until sufficient strength is regained and radiographic healing is confirmed.
Phase 4: Return to Sport / High-Demand Activities (Months 6+)
- Goals: Achieve full return to pre-injury activity level, including sports.
-
Progression:
- Sport-Specific Training: Incorporate plyometric exercises, throwing programs, and agility drills tailored to the patient's sport.
- Heavy Lifting and Impact: Gradually introduce heavy lifting and activities involving high impact or repetitive overhead movements.
- Maintenance Program: Advise on a long-term home exercise program to maintain strength and flexibility and prevent recurrence.
Important Considerations:
*
Radiographic Healing:
Clinical progress should be correlated with radiographic evidence of fracture healing before advancing to higher-load activities.
*
Patient Compliance:
Adherence to the rehabilitation protocol is crucial.
*
Pain as a Guide:
Pain should be a primary guide for progression; exercises should not cause significant or prolonged pain.
Summary of Key Literature / Guidelines
Current management strategies for scapula fractures are guided by a growing body of evidence, primarily comprising retrospective case series, comparative studies, and expert consensus. While Level I evidence (randomized controlled trials) is scarce due to the rarity and heterogeneity of these injuries, several key themes and guidelines have emerged.
-
Non-Operative vs. Operative Decision-Making:
- A significant portion of scapular body fractures heal well with non-operative management due to the surrounding muscle envelope. Early functional rehabilitation is key.
- Operative fixation is increasingly favored for displaced intra-articular glenoid fractures, significantly displaced scapular neck fractures (angulation >40°, translation >1 cm), and "floating shoulder" injuries (ipsilateral clavicle and scapular neck/body fracture). The rationale for surgery in these cases is to restore articular congruity, glenoid version, and overall shoulder girdle stability, aiming to improve long-term functional outcomes and reduce the risk of post-traumatic arthritis or impingement.
- Studies by Ada and Miller (1991) and Thompson et al. (1995) highlighted the importance of early motion in non-operatively treated fractures and the poor outcomes associated with significant displacement of glenoid or neck fractures, respectively.
- More recently, Kontakis et al. (2014) systematic review underscored the consensus that displaced glenoid and neck fractures benefit from ORIF, while isolated body fractures often do not.
-
Surgical Approaches and Techniques:
- The Judet posterior approach remains the gold standard for most displaced scapular fractures involving the glenoid, neck, and body. Its ability to provide comprehensive exposure and accommodate various plating configurations makes it versatile.
- Advancements in plating technology, particularly the use of pre-contoured locking plates , have improved fixation stability and reduced hardware prominence. The concept of creating a "construct" with plates along the lateral border and spine for neck fractures is well-established.
- CT with 3D reconstruction is universally acknowledged as indispensable for pre-operative planning, providing detailed anatomical information critical for surgical decision-making and preventing iatrogenic injury.
-
Floating Shoulder Injuries:
- The management of floating shoulder (ipsilateral clavicle and scapula fracture) is debated. Historically, many were treated non-operatively. However, a growing body of literature suggests that operative fixation of at least one component (typically the clavicle, or more robustly, the scapular neck) , particularly in significantly displaced patterns, improves outcomes by restoring the integrity of the superior shoulder suspensory complex (SSSC) and preventing medial translation of the glenoid.
- Oh et al. (2012) and Egol et al. (2010) demonstrated superior functional outcomes and reduced rates of malunion with operative fixation of displaced floating shoulder injuries.
-
Complications and Outcomes:
- While operative treatment improves reduction and stability, it carries risks, notably neurovascular injury (suprascapular and axillary nerves) . Meticulous technique, careful soft tissue handling, and awareness of nerve courses are crucial.
- Long-term outcomes, particularly for articular glenoid fractures, are influenced by the quality of reduction. Post-traumatic arthritis remains a significant concern if anatomical congruity is not restored.
- Early, controlled rehabilitation is paramount to prevent stiffness and optimize functional recovery, regardless of operative or non-operative management.
-
Areas of Ongoing Research:
- The optimal number and configuration of plates for complex scapular fractures.
- The role of arthroscopic assistance in glenoid fracture fixation.
- Further clarification on specific indications for "floating shoulder" operative intervention.
- Long-term functional outcomes comparing different fixation techniques and rehabilitation protocols.
In conclusion, the current consensus emphasizes careful patient selection for operative intervention, guided by detailed imaging and a thorough understanding of fracture biomechanics. Anatomic reduction and stable fixation, primarily via posterior approaches, followed by a structured rehabilitation program, are the cornerstones of successful management for complex and displaced scapula fractures, aiming to restore pre-injury shoulder function and minimize long-term sequelae.
