Scapulothoracic Dissociation
- This injury is a traumatic disruption of the scapula from the posterior chest wall.
- This rare, life-threatening injury is essentially a subcutaneous fore-quarter amputation.
- The mechanism is a violent traction and rotation force, usually as a result of a motor vehicle or motorcycle accident.
- Neurovascular injury is common: 1. Complete brachial plexopathy: 80%
- Partial plexopathy: 15%
- Subclavian or axillary artery: 88%
- It can be associated with fracture or dislocation about the shoulder or without obvious bone injury.
- Diagnosis includes: 1. Massive swelling of shoulder region
- A pulseless arm
- A complete or partial neurologic deficit
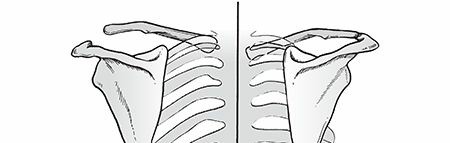
-
Lateral displacement of the scapula on a nonrotated chest radiograph, which is diagnostic (
Fig. 13.7
)


- Classification ## Type I: Musculoskeletal injury alone
Type IIA: Musculoskeletal injury with vascular disruption
Type IIB: Musculoskeletal injury with neurologic impairment
Type III: Musculoskeletal injury with both neurologic and vascular injury
- Initial treatment 1. Patients are often polytraumatized.
- Advanced trauma life support protocols should be followed.
-
Angiography of the limb with vascular repair and exploration of brachial plexus are performed
as indicated. - Stabilization of associated bone or joint injuries is indicated.
- Later treatment 1. Neurologic
- At 3 weeks, electromyography is indicated.
- At 6 weeks, cervical myelography or magnetic resonance imaging (MRI) is performed.
- Shoulder arthrodesis and/or above elbow amputation may be necessary if the limb is flail.
- Nerve root avulsions and complete deficits have a poor prognosis.
- Partial plexus injuries have good prognosis, and functional use of the extremity is often regained.
- MRI—“empty sleeve sign”
- Osseous
- If initial exploration of the brachial plexus reveals a severe injury, primary above elbow amputation should be considered.
-
If cervical myelography reveals three or more pseudomeningoceles, the prognosis is similarly
poor. - This injury is associated with a poor outcome including flail extremity in 52%, early amputation in 21%, and death in 10%.
Intrathoracic Dislocation of the Scapula
- This is extremely rare.
- The inferior angle of the scapula is locked in the intercostal space.
- Chest computed tomography may be needed to confirm the diagnosis.
- Treatment consists of closed reduction and immobilization with a sling and swathe for 2 weeks, followed by progressive functional use of the shoulder and arm.
