Scapula Fractures: How a Fall on Outstretched Hand Leads to Injury
Introduction & Epidemiology
Scapula fractures represent a rare subset of shoulder girdle injuries, typically indicative of high-energy trauma. Their uncommon nature, accounting for less than 1% of all fractures and approximately 3-5% of shoulder girdle fractures, often leads to an underestimation of their associated injury burden. A high index of suspicion is paramount, as these fractures are frequently accompanied by severe concurrent injuries, including pulmonary compromise, head trauma, and other orthopedic disruptions, contributing to elevated Injury Severity Scores (ISS).
Diagnosis relies initially on plain radiographs, specifically a trauma series comprising anteroposterior (AP), scapular Y, and axillary views. However, a computed tomography (CT) scan with multiplanar reconstructions (MPR) and three-dimensional (3D) volumetric rendering is indispensable for comprehensive fracture characterization, evaluation of articular involvement, assessment of displacement, and meticulous pre-operative surgical planning. The intricate anatomy of the scapula and its surrounding soft tissues necessitates detailed imaging to fully appreciate the extent of injury.
Treatment paradigms range from nonoperative management with sling immobilization for stable, minimally displaced fractures to operative intervention for specific patterns. Surgical indications primarily include intra-articular fractures with significant displacement or step-off, markedly displaced scapular body or neck fractures, open fractures, and those associated with glenohumeral instability, particularly fracture-dislocations.
Epidemiology
- Incidence: Scapula fractures are uncommon, representing <1% of all fractures and 3-5% of shoulder girdle fractures.
- Demographics: These injuries commonly occur in individuals between 25 and 50 years of age, with a notable male predominance. This demographic profile aligns with the higher incidence of high-energy trauma in young to middle-aged males.
Etiology and Mechanisms of Injury
Scapula fractures predominantly result from high-energy trauma, accounting for 80-90% of cases. Motor vehicle collisions (MVCs) are the most common mechanism, comprising over 70% of scapula fractures, often involving direct impact to the posterior shoulder.
Indirect trauma, particularly a fall on an outstretched hand (FOOSH) , is a significant mechanism. In a FOOSH injury, axial loading through the humerus transmits compressive and shear forces to the glenoid, often resulting in glenoid rim or fossa fractures. This mechanism can also lead to avulsion fractures of the coracoid or acromion via ligamentous pull or impact from the humeral head. Glenohumeral dislocations, both anterior and posterior, frequently result in associated glenoid rim fractures (Bankart or reverse Bankart lesions) due to impaction or avulsion. Rare mechanisms include seizure activity and electric shock, causing violent muscle contractions that can lead to avulsion fractures.
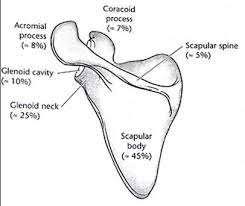
Location and Associated Injuries
Fracture patterns vary significantly depending on the mechanism and vector of force.
*
Scapular body/spine:
45-50%
*
Glenoid:
35%
* Glenoid neck: 25%
* Glenoid fossa/rim: 10% (often associated with impaction of the humeral head into the glenoid)
*
Acromion:
8%
*
Coracoid:
7%

Associated injuries are present in 80-95% of patients with scapula fractures, underscoring the need for a comprehensive trauma workup.
*
Thoracic Injury (80%):
* Hemothorax/pneumothorax (>30%)
* Pulmonary contusion (>40%)
* Rib fractures (up to 50%), including flail chest
* Diaphragmatic rupture
*
Head Injury (35-50%)
*
Abdominal Injury (up to 25%)
*
Vascular Injury:
Subclavian artery/vein, axillary artery (rare but limb-threatening)
*
Neurological Injury:
Brachial plexus (5-10%), suprascapular nerve palsy
*
Ipsilateral Clavicle Fracture (15-40%):
Combined with a scapular neck fracture, this constitutes a "floating shoulder" injury, potentially disrupting the Superior Shoulder Suspensory Complex (SSSC).
*
Ipsilateral Upper Extremity Fractures:
Humerus, forearm, hand fractures.
Surgical Anatomy & Biomechanics
The scapula is a flat, triangular bone crucial for shoulder girdle function and stability. Its unique position, suspended by muscular attachments rather than direct axial skeletal articulation, allows for extensive motion and acts as a stable platform for the glenohumeral joint.
Anatomy
- Body: The broad, flat portion, providing attachment for multiple muscles (subscapularis anteriorly, infraspinatus/teres major/minor posteriorly).
- Spine: A prominent ridge extending posteromedially to laterally, terminating in the acromion. Separates the supra- and infraspinous fossae.
- Acromion: The lateral extension of the spine, articulating with the clavicle to form the acromioclavicular (AC) joint. Provides attachment for the deltoid and trapezius muscles.
- Coracoid Process: A hook-like anterior projection, serving as an origin for the coracobrachialis and short head of the biceps, and attachment for the pectoralis minor, coracoclavicular (conoid and trapezoid), and coracoacromial ligaments.
- Glenoid Fossa: The shallow, pear-shaped articular surface that articulates with the humeral head. It is typically retroverted (0-7 degrees) and superiorly inclined (5-10 degrees). The labrum enhances stability and deepens the fossa.
- Glenoid Neck: The constricted region connecting the glenoid to the scapular body.
Neurovascular Structures
Understanding the regional neurovascular anatomy is critical for surgical planning and avoiding iatrogenic injury.
*
Suprascapular Nerve:
Originates from the upper trunk of the brachial plexus (C5, C6). Courses laterally across the posterior triangle of the neck, passes through the suprascapular notch (inferior to the superior transverse scapular ligament) to innervate the supraspinatus. It then curves around the spinoglenoid notch (inferior to the inferior transverse scapular ligament) to innervate the infraspinatus. This nerve is particularly vulnerable to injury during approaches to the scapular neck and glenoid, especially with superior plating or excessive retraction.
*
Axillary Nerve:
Arises from the posterior cord of the brachial plexus (C5, C6). Passes through the quadrangular space (bounded by teres minor, teres major, long head of triceps, and surgical neck of humerus) to supply the deltoid and teres minor. It is at risk during posterior approaches to the inferior glenoid, especially during plate application.
*
Dorsal Scapular Nerve:
Originates from the C5 nerve root. Runs inferiorly to innervate the rhomboids and levator scapulae.
*
Long Thoracic Nerve:
Originates from C5, C6, C7. Innervates the serratus anterior. At risk with medial retraction of the scapula.
*
Circumflex Scapular Artery:
A branch of the subscapular artery (from the axillary artery). Passes through the triangular space and supplies the infraspinatus and teres minor.
*
Suprascapular Artery:
Often accompanies the suprascapular nerve, typically passing
over
the superior transverse scapular ligament.
Biomechanics
The scapula's mobility and muscular suspension allow for coordinated motion of the entire upper extremity. During a FOOSH injury, the axial load transmitted from the hand through the forearm and humerus impacts the glenoid. This direct impaction can cause:
1.
Glenoid Fossa Fractures:
Chondral or osteochondral lesions, or more substantial articular fractures (Ideberg types).
2.
Glenoid Rim Fractures:
Avulsion or impaction fractures of the anterior or posterior rim, often leading to glenohumeral instability (fracture-dislocation).
3.
Glenoid Neck Fractures:
Resulting from the transmitted forces causing shear or bending moments at the relatively narrow neck.
Indirect forces, such as violent muscle contractions or forces transmitted through ligaments (e.g., coracoclavicular ligaments during clavicle fracture), can lead to avulsion fractures of the coracoid or acromion. Direct posterior impact to the body or spine often causes comminuted fractures. The integrity of the SSSC, formed by the glenoid, scapular body, coracoid, coracoclavicular ligaments, and clavicle, is paramount for shoulder stability. Disruption of two or more components of the SSSC (e.g., ipsilateral clavicle fracture and displaced scapular neck fracture, or superior acromial fracture with coracoclavicular ligament disruption) defines a "floating shoulder" injury, which significantly compromises shoulder stability and may necessitate operative stabilization.
Indications & Contraindications
The decision for operative versus non-operative management of scapula fractures is complex, weighing fracture characteristics, patient factors, and the presence of associated injuries. Most scapula fractures can be managed non-operatively.
Non-Operative Indications
- Scapular body and spine fractures: Undisplaced or minimally displaced (<1 cm displacement, <20 degrees angulation) without significant soft tissue disruption or involvement of the glenoid.
- Glenoid neck fractures: Undisplaced or minimally displaced (<1 cm displacement, <20-30 degrees angulation) without concomitant ipsilateral clavicle fracture or disruption of the SSSC.
- Acromial fractures: Undisplaced or minimally displaced, without impingement on the rotator cuff space.
- Coracoid fractures: Undisplaced or minimally displaced, not involving the base and without significant disruption of the coracoclavicular ligaments.
- Minimally displaced intra-articular glenoid fractures (Ideberg Type I/II): Generally <2mm step-off and <5mm gap.
- Patients with significant medical comorbidities precluding surgery.
Operative Indications
Operative intervention aims to restore anatomical alignment, provide a stable platform for glenohumeral function, and facilitate early rehabilitation.
*
Glenoid Fractures:
*
Articular step-off >2mm or articular gap >5mm:
Especially in young, active patients.
*
Glenoid rim fractures associated with persistent glenohumeral instability
(fracture-dislocation, often Ideberg Type I-IV).
*
Large articular fragments
comprising >25% of the glenoid surface, leading to instability.
*
Ideberg Type V
(combined glenoid fossa and neck fracture).
*
Glenoid Neck Fractures:
*
Angulation >40 degrees or displacement >1 cm.
*
Floating Shoulder Injury:
Scapular neck fracture with an ipsilateral displaced clavicle fracture, particularly if there is significant displacement or angulation of the scapular component, or complete disruption of the SSSC.
*
Scapular Body Fractures:
* Significant displacement (>2-3 cm) with severe angulation, especially if impinging on the chest wall or interfering with rotator cuff function.
* Gross displacement in the setting of a floating shoulder injury or polytrauma where anatomical restoration is deemed beneficial for overall recovery.
*
Acromial Fractures:
*
Displaced fractures leading to subacromial impingement
(e.g., fracture fragment compromising the rotator cuff space).
*
Significant displacement
leading to superior humeral head migration.
*
Coracoid Fractures:
*
Displaced fractures involving the base
with significant disruption of the coracoclavicular ligaments, especially in conjunction with an AC joint separation or clavicle fracture.
*
Large avulsion fractures
significantly affecting biceps/coracobrachialis function.
*
Open Fractures.
*
Neurovascular Compromise:
Fracture fragments directly impinging on neurovascular structures.
Contraindications
- Severe comminution where stable fixation is not achievable or unlikely to improve functional outcome significantly.
- Significant active infection.
- Severe medical comorbidities or physiological instability (e.g., polytrauma patients in extremis) where the risks of surgery outweigh the benefits.
- Extensive soft tissue injury or poor skin quality precluding safe surgical access and wound closure.
Operative vs. Non-Operative Indications Summary Table
| Feature | Non-Operative Management | Operative Management |
|---|---|---|
| Glenoid Fractures | <2mm articular step-off, <5mm gap, stable | >2mm articular step-off, >5mm gap, glenohumeral instability (fracture-dislocation), >25% glenoid involvement, Ideberg Type V |
| Glenoid Neck Fractures | <1cm displacement, <40° angulation, no SSSC disruption | >1cm displacement, >40° angulation, Floating Shoulder (scapular neck + ipsilateral clavicle fracture), significant SSSC disruption |
| Scapular Body Fractures | <2cm displacement, stable | Gross displacement (>2-3cm), severe angulation, significant impact on rotator cuff or SSSC stability (rare as isolated injury) |
| Acromial Fractures | Undisplaced, no impingement | Displaced causing subacromial impingement, superior humeral head migration |
| Coracoid Fractures | Undisplaced base, no ligament disruption | Displaced base with coracoclavicular ligament disruption, large avulsion affecting biceps/coracobrachialis function |
| Other Considerations | Significant medical comorbidities, elderly with low demand | Open fractures, neurovascular compromise, pathological fractures |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is crucial for successful scapula fracture fixation, particularly given the complex anatomy and high association with other injuries.
Workup and Imaging
- Primary and Secondary Survey: Thorough evaluation for life-threatening injuries, especially in polytrauma patients. Scapula fractures are a marker for severe trauma.
- Radiographs: AP, scapular Y, and axillary views are standard. Stryker notch view may be useful for anterior glenoid rim fractures.
-
Computed Tomography (CT):
Essential for all displaced or articular scapula fractures.
- Axial, sagittal, and coronal reconstructions: To assess fracture lines, comminution, and articular involvement.
- 3D reconstructions: Invaluable for visualizing the complex 3D anatomy, fracture patterns, displacement, and relationships between fragments. This aids in surgical approach selection and implant templating.
- CT angiogram may be necessary if vascular injury is suspected.
- Magnetic Resonance Imaging (MRI): Not routine for acute fracture management, but may be considered for suspected rotator cuff tears, labral injuries, or brachial plexus lesions that influence treatment.
Classification Systems
- AO/OTA Classification: A comprehensive system for all fractures, but can be cumbersome for scapula.
-
Ideberg Classification (for Glenoid Fractures):
Widely used and highly relevant.
- Type I: Anterior (IA) or posterior (IB) rim fracture.
- Type II: Transverse fracture through the glenoid fossa exiting inferiorly.
- Type III: Transverse fracture through the glenoid fossa exiting superiorly (often with suprascapular nerve involvement).
- Type IV: Horizontal fracture through the glenoid fossa into the body/neck.
- Type V: Combination of Ideberg Type II and IV.
- Type VI: Severe comminution of the glenoid articular surface.
- Euler Classification (for Scapular Body and Neck Fractures): Less commonly used in practice but provides anatomical descriptors.
Timing of Surgery
While open fractures or fracture-dislocations with irreducible humeral head dislocation require urgent intervention, most scapula fractures can be safely delayed for 3-7 days, or even longer, until the patient is medically stable and swelling has subsided. This allows for thorough planning and optimization of surgical conditions.
Templating and Implant Selection
- Pre-contoured Locking Plates: Scapula-specific plates are available, designed to fit the complex contours of the lateral border, glenoid neck, and spine.
- Small Fragment Locking Plates: 2.7mm or 3.5mm systems are common.
- Screws: Variable-angle locking screws provide pull-out strength in thin bone. Bi-cortical fixation is preferred where possible, especially in the glenoid neck.
Patient Positioning
Proper positioning is critical for optimal exposure and management of neurovascular structures.
*
Prone Position:
*
Advantages:
Excellent exposure for posterior approaches to the scapular body, spine, glenoid neck, and posterior glenoid. Allows for easier intraoperative fluoroscopy.
*
Disadvantages:
Potential for airway compromise, pressure sores, difficult anterior glenoid access.
*
Setup:
Chest rolls to free the chest and abdomen. Arm draped free on an arm board or suspended in traction to allow manipulation.

*
Lateral Decubitus Position:
*
Advantages:
Good exposure for posterior approaches. Allows for slight anterior translation of the scapula away from the chest wall.
*
Setup:
Axillary roll, beanbag. Arm draped free, often suspended in traction.
*
Beach Chair Position:
*
Advantages:
Optimal for anterior approaches (e.g., anterior glenoid rim), good for glenohumeral arthroscopy if combined.
*
Disadvantages:
Limited posterior access.
*
Setup:
Standard beach chair setup, head secured.
Pre-operative Considerations
- Antibiotics: Prophylactic intravenous antibiotics.
- DVT Prophylaxis: As per institutional protocols, especially given the trauma context.
- Anesthesia: General anesthesia is typical. Regional blocks (e.g., interscalene) may be used for post-operative pain control.
- Fluoroscopy: C-arm must be readily available and draped sterilely for intraoperative verification of reduction and hardware placement.
Detailed Surgical Approach / Technique
The goal of surgical fixation is anatomical reduction, especially of the articular surface, and stable internal fixation to allow early rehabilitation. Indirect reduction techniques are often employed to minimize soft tissue stripping.
General Principles
- Articular surface reduction: Critical for glenoid fractures to prevent post-traumatic arthritis.
- Stable fixation: Achieved with plates and screws that provide adequate biomechanical strength in the thin scapular bone.
- Soft tissue preservation: Minimizing dissection to maintain vascularity and reduce complications.
- Neurovascular protection: Vigilant identification and protection of the suprascapular nerve, axillary nerve, and associated vessels.
Surgical Approaches
1. Posterior (Judet) Approach
This is the most common and versatile approach for fractures of the glenoid, glenoid neck, scapular body, and spine.
*
Patient Position:
Prone or lateral decubitus.
*
Incision:
A curvilinear incision starting from the posterolateral corner of the acromion, extending inferiorly and medially along the scapular spine, and then curving inferiorly along the medial border of the scapula. Alternatively, a more direct incision along the lateral border of the scapula.
*
Dissection:
1.
Skin and subcutaneous tissues
are incised. Subcutaneous flaps are developed.
2.
Internervous plane:
The interval between the deltoid and teres minor allows access to the lateral border of the scapula. More medially, the interval between infraspinatus and teres minor or between deltoid and trapezius can be utilized.
3.
Exposure of the Scapular Spine:
The deltoid origin is detached from the scapular spine, typically subperiosteally, to expose the spine and acromion.
4.
Exposure of the Infraspinous Fossa:
The infraspinatus muscle is detached from its fossa and retracted superiorly, or split longitudinally in line with its fibers if a more direct approach to the posterior glenoid is needed. Careful identification and protection of the suprascapular nerve within the spinoglenoid notch is critical.
5.
Exposure of the Lateral Border/Inferior Glenoid:
The interval between the infraspinatus and teres minor is developed. The teres minor is typically retracted inferiorly.
6.
Exposure of the Glenoid Neck and Lateral Scapular Body:
The interval between the deltoid and teres minor is utilized. The axillary nerve and posterior humeral circumflex artery run approximately 5-7 cm inferior to the inferior glenoid rim, exiting the quadrangular space. Protection of these structures is paramount, especially when placing plates on the inferior aspect of the glenoid neck.

Judet (posterior) approach to scapula body, glenoid neck, and glenoid.

The internervous plane between the deltoid and teres minor is utilized for the Judet approach. The axillary nerve and posterior humeral circumflex artery are visualized in the quadrangular space, inferior to the teres minor.
-
Reduction Techniques:
- Indirect Reduction: Often preferred. Distal traction on the arm, manipulation with ball-spiked pushers, joysticks (K-wires inserted into fragments).
- Direct Reduction: Articular fragments of the glenoid are reduced under direct visualization. Pointed reduction clamps are invaluable for holding fragments.
-
Temporary Fixation:
K-wires are used to provisionally secure reduced fragments. Intraoperative fluoroscopy (AP, lateral, axillary views) confirms reduction.

Reduction of a glenoid neck fracture with K-wires.
-
Definitive Fixation:
- Glenoid Fossa: Articular fragments are typically reduced first. Small cancellous screws (e.g., 2.7mm or 3.5mm) can be placed from posterior to anterior to lag articular fragments, ensuring screw heads are flush or countersunk below the articular surface.
-
Glenoid Neck:
Plate fixation is the mainstay.
- Lateral Border Plate: A pre-contoured plate (e.g., reconstruction plate, scapula-specific plate) is applied to the lateral border of the scapula, extending onto the glenoid neck. Screws are placed bicortically where possible, carefully avoiding the glenoid articular surface and neurovascular structures.
- Posterior Glenoid Plate: For Ideberg Type II or V fractures, a plate may be applied more posteriorly on the glenoid neck, often extending superiorly or inferiorly.
-
Dual plating:
Sometimes necessary for highly unstable fractures, with plates on the lateral border and superior aspect, or lateral border and posterior aspect. Careful attention to the suprascapular nerve when placing superior hardware.

Lateral border plate fixation for a glenoid neck fracture.

Post-operative radiograph of a scapula fracture with plate and screw fixation.
- Scapular Body and Spine: For significantly displaced body or spine fractures, especially in the context of a floating shoulder, plate fixation along the lateral border and/or spine may be used. Direct exposure through muscle splitting or detaching (e.g., infraspinatus from its fossa) is required. Low-profile plates are preferred to avoid soft tissue irritation.
2. Anterior (Deltopectoral) Approach
Less commonly used for primary scapula fractures, but useful for anterior glenoid rim fractures, coracoid fractures, or anterior dislocations with large bony Bankart lesions.
*
Patient Position:
Beach chair or supine.
*
Incision:
Deltopectoral groove incision.
*
Dissection:
Interval between deltoid and pectoralis major is developed. Cephalic vein is identified and preserved or ligated. Coracoid process is identified. Subscapularis can be detached or split to access the anterior glenoid. The musculocutaneous nerve (innervating coracobrachialis and biceps) should be protected, as it enters the coracobrachialis muscle.
3. Superior (Sabre-Cut) Approach
For acromial fractures or superior glenoid fractures.
*
Patient Position:
Beach chair or prone.
*
Incision:
A longitudinal incision over the superior aspect of the shoulder, often along the acromion.
*
Dissection:
Deltoid splitting approach. Care to identify the neurovascular structures around the acromion and coracoid.
Wound Closure
After achieving stable fixation and confirming reduction with fluoroscopy, the wound is copiously irrigated. A drain may be placed if significant dead space or bleeding is anticipated. Muscles are reapproximated (e.g., deltoid reattached to scapular spine), followed by layered closure of subcutaneous tissues and skin.
Complications & Management
Scapula fracture surgery, while effective for select indications, carries a risk of various complications, both intraoperative and postoperative.
Intraoperative Complications
-
Neurovascular Injury (5-15%):
- Suprascapular Nerve: Most vulnerable during superior or posterior plating, especially at the spinoglenoid notch. Prevention involves careful dissection, identification, and avoiding excessive traction or direct plate/screw impingement. Management: Acute neuropraxia often recovers; persistent palsy may require neurolysis or transfer.
- Axillary Nerve: At risk during approaches to the inferior glenoid or lateral border due to its proximity (5-7 cm inferior to glenoid rim). Prevention: Careful dissection, use of blunt retractors, avoiding deep screw placement inferiorly. Management: As above.
- Subclavian/Axillary Vessels: Rare, but potentially catastrophic. Prevention: Meticulous dissection, particularly with medial body fractures. Management: Vascular repair.
- Iatrogenic Fracture: During reduction or screw placement. Management: Extended fixation.
- Excessive Blood Loss: Scapula is highly vascularized. Careful hemostasis.
- Infection: Standard surgical prophylaxis.
Early Postoperative Complications
- Wound Infection (1-5%): Superficial or deep. Management: Debridement, antibiotics.
- Wound Dehiscence: Especially with extensive swelling or poor skin quality. Management: Local wound care, potentially surgical closure.
- Hematoma: May require drainage.
- Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE): Standard prophylaxis.
- Pneumonia: Especially in polytrauma patients. Aggressive pulmonary hygiene.
Late Postoperative Complications
-
Nonunion / Malunion (5-10%):
- Incidence: Higher in comminuted fractures, poor fixation, or early return to activity. Glenoid neck fractures are particularly prone to malunion.
- Management: Symptomatic nonunion may require revision surgery with bone grafting. Malunion causing pain or impingement may necessitate corrective osteotomy.
-
Hardware Failure / Prominence (10-20%):
- Incidence: Plates and screws can become prominent, especially in thin patients or with suboptimally contoured plates, leading to pain or soft tissue irritation.
- Management: Symptomatic hardware typically requires removal after fracture union (6-12 months).
-
Post-Traumatic Arthritis (PTA) (10-30% for articular fractures):
- Incidence: Directly correlated with the quality of articular reduction, size of initial defect, and severity of comminution.
- Management: Initial non-operative measures (NSAIDs, physical therapy, injections). For end-stage arthritis, surgical options include glenohumeral arthroplasty (total shoulder arthroplasty, reverse shoulder arthroplasty for rotator cuff deficient cases, or hemiarthroplasty), fusion, or débridement.
-
Stiffness / Loss of Motion (20-40%):
- Incidence: A common sequela due to prolonged immobilization, capsular contracture, or muscle scarring.
- Management: Aggressive, supervised physical therapy is paramount. Manipulation under anesthesia or capsular release may be required in refractory cases.
- Pain: Chronic pain can result from malunion, arthritis, or hardware.
- Heterotopic Ossification: Can occur with extensive soft tissue dissection. Prophylaxis with NSAIDs or low-dose radiation may be considered in high-risk patients.
Complications and Management Table
| Complication | Incidence | Salvage Strategy |
|---|---|---|
| Neurovascular Injury | 5-15% | Neurolysis, nerve repair/graft, vascular repair |
| Wound Infection | 1-5% | Debridement, antibiotics, wound vac, delayed closure |
| Nonunion / Malunion | 5-10% | Revision surgery, bone grafting, corrective osteotomy |
| Hardware Failure/Prominence | 10-20% | Hardware removal after union, revision fixation if nonunion |
| Post-Traumatic Arthritis | 10-30% (articular) | Non-operative management, eventually arthroplasty (TSA, RSA, Hemi), fusion |
| Stiffness / Loss of Motion | 20-40% | Aggressive physical therapy, manipulation under anesthesia, capsular release |
| Chronic Pain | Variable | Pain management, hardware removal, revision surgery |
Post-Operative Rehabilitation Protocols
Rehabilitation following scapula fracture fixation is critical for restoring function and preventing long-term complications such as stiffness and weakness. Protocols are individualized based on fracture stability, fixation achieved, and the patient's overall health and commitment to therapy. A balance between protecting the repair and initiating early motion is essential.
Phase I: Protection Phase (0-6 Weeks Post-Op)
- Goals: Protect fracture healing, control pain and swelling, maintain mobility of uninvolved joints.
- Immobilization: Arm in a sling for comfort and protection. Sling can be removed for hygiene and prescribed exercises.
-
Motion:
- Passive Range of Motion (PROM): Gentle pendulum exercises (Codman's) initiated early (within the first week), focusing on gravity-assisted motion without active muscle contraction.
- Elbow, Wrist, Hand: Active range of motion (AROM) exercises for the distal joints are encouraged from day one to prevent stiffness and promote circulation.
- Scapular Setting: Gentle isometric contractions of periscapular muscles to encourage stability without stressing the fracture site.
- Weight-Bearing: No weight-bearing or active lifting with the affected arm.
- Patient Education: Strict instructions on avoiding active shoulder movement, lifting, or sudden movements.
Phase II: Early Mobility Phase (6-12 Weeks Post-Op)
- Goals: Gradually increase shoulder range of motion, initiate light strengthening.
-
Motion:
- Active-Assisted Range of Motion (AAROM): Progress from PROM to AAROM, using the unaffected arm or a pulley system to assist motion. Focus on forward flexion, abduction, and gentle external/internal rotation within pain-free limits.
- Active Range of Motion (AROM): Gradually introduce unassisted AROM as tolerated and as bony healing progresses (typically around 8-10 weeks).
-
Strengthening:
- Isometrics: Begin gentle isometric strengthening of the rotator cuff and periscapular muscles (e.g., against a wall), ensuring no pain at the fracture site.
- Light resistance: Introduce very light resistance exercises with elastic bands for rotator cuff strengthening (internal/external rotation) and scapular stabilization.
- Weight-Bearing: Still no heavy lifting. Avoid pushing or pulling heavy objects.
Phase III: Strengthening Phase (12+ Weeks Post-Op)
- Goals: Restore full range of motion, maximize strength, power, and endurance, return to functional activities.
- Motion: Continue to work on achieving full, pain-free AROM.
-
Strengthening:
- Progressive Resistive Exercises (PREs): Systematically increase resistance and load. Focus on all major muscle groups of the shoulder girdle and upper extremity.
- Rotator Cuff and Scapular Stabilizers: Emphasize strengthening of the rotator cuff (supraspinatus, infraspinatus, teres minor, subscapularis) and scapular stabilizers (serratus anterior, rhomboids, trapezius).
- Proprioceptive Exercises: Incorporate exercises to improve joint position sense and neuromuscular control.
-
Functional Training:
- Gradual return to activity-specific or sport-specific training.
- Introduction of overhead activities and weight-bearing as appropriate for the individual's demands and fracture healing status.
- Return to Sport/Work: Varies widely, but typically 4-6 months for light activities and 6-12 months for contact sports or heavy labor, pending radiographic union and full strength recovery.
Key Considerations:
*
Pain Control:
Adequate pain management is essential to facilitate participation in physical therapy.
*
Radiographic Healing:
Progress of rehabilitation should be guided by radiographic evidence of fracture healing.
*
Individualization:
Each protocol must be tailored to the specific fracture pattern, surgical stability, and patient's response to therapy. Close communication between the surgeon and physical therapist is crucial.
*
Avoidance of Overuse:
Prevent early aggressive mobilization or strengthening that could disrupt fixation or delay healing.
Summary of Key Literature / Guidelines
Scapula fracture literature, while growing, often consists of retrospective series and expert opinions due to the rarity and heterogeneity of these injuries. However, several themes and evidence-based recommendations have emerged.
-
Role of CT and 3D Reconstruction:
- There is universal consensus that CT scanning with 3D reconstructions is essential for comprehensive characterization of scapula fractures, especially those involving the glenoid or neck. This imaging modality allows for accurate assessment of articular involvement, displacement, and comminution, which directly impacts surgical decision-making and planning. Studies consistently demonstrate the superiority of CT over plain radiographs for defining fracture morphology and guiding treatment.
-
Indications for Operative Fixation:
- The primary drivers for operative intervention are glenohumeral instability and significant displacement of the articular surface .
- Glenoid Fractures (Ideberg Classification): Ideberg Type I fractures (rim fractures) causing instability are often fixated. Types II, III, and V with articular step-off >2mm or significant instability are strong indications for surgery to prevent post-traumatic arthritis and chronic instability. Type VI (comminution) remains challenging, with outcomes depending on reconstructibility.
- Glenoid Neck Fractures: Displaced glenoid neck fractures with >1 cm translation or >40 degrees of angulation are generally considered for surgery. The most compelling indication for surgical fixation of a glenoid neck fracture is its association with an ipsilateral clavicle fracture, forming a "floating shoulder." When both components of the SSSC are disrupted, especially with significant displacement of the scapular component, operative stabilization has been shown to improve functional outcomes compared to non-operative management, reducing shoulder girdle collapse and malunion.
- Scapular Body Fractures: Isolated, significantly displaced scapular body fractures rarely require operative fixation. However, in polytrauma patients or in the setting of severe floating shoulder injuries, fixation of severely displaced body fractures may be considered to restore shoulder mechanics and provide a stable platform.
- Acromial/Coracoid Fractures: Fixation is typically reserved for displaced acromial fractures causing impingement or significantly displaced coracoid fractures compromising coracoclavicular ligament integrity or biceps/coracobrachialis function.
-
Surgical Timing:
- While open fractures or fracture-dislocations warrant emergent intervention, elective fixation of most scapula fractures can be safely delayed for several days to weeks. This allows for resolution of soft tissue swelling, improved patient physiological status (especially in polytrauma), and thorough pre-operative planning, without significantly compromising outcomes.
-
Surgical Approaches and Techniques:
- The posterior Judet approach is the workhorse for most scapula fractures, allowing excellent visualization of the glenoid, neck, lateral border, and posterior body. Meticulous identification and protection of the suprascapular and axillary nerves are critical.
- Reduction techniques prioritize anatomical reduction of the articular surface, often utilizing indirect maneuvers initially, followed by direct reduction with clamps and K-wires.
- Fixation typically involves low-profile locking plates and screws, often pre-contoured, to conform to the complex anatomy. Dual plating constructs may be used for highly unstable fractures to provide multiplanar stability.
-
Outcomes and Complications:
- Functional outcomes following operative fixation are generally good to excellent for appropriately selected cases, with improvement in pain, range of motion, and strength. However, the complexity of these injuries and high association with polytrauma often influence overall functional recovery.
- Complications such as post-traumatic arthritis (especially with articular involvement), stiffness, hardware prominence, and neurological injury remain notable concerns. Long-term follow-up is essential to assess for degenerative changes and patient satisfaction.
-
Controversies:
- The optimal management of borderline displaced glenoid neck fractures (e.g., 30-40 degrees angulation) without clavicle involvement remains controversial, with some advocating for non-operative management if stable.
- The precise role of routine fixation for all "floating shoulder" injuries is debated, with some studies suggesting that well-reduced scapular neck fractures may fare well with non-operative management of the scapular component if the clavicle is also managed appropriately.
- The management of severely comminuted glenoid fractures (Ideberg Type VI) is challenging, with outcomes often guarded, and the role of early arthroplasty versus reconstruction debated.
In summary, current guidelines emphasize a tailored approach to scapula fractures, driven by detailed imaging, a thorough understanding of fracture patterns and associated injuries, and a clear appreciation of the patient's functional demands and comorbidities. While most scapula fractures heal non-operatively, surgical intervention for specific unstable patterns, particularly those involving the articular surface or compromising the SSSC, significantly improves outcomes and reduces long-term disability.
