Introduction to Rigid Pes Planus
While flexible pes planus is a common, often asymptomatic condition that rarely necessitates surgical intervention, rigid pes planus frequently produces significant biomechanical dysfunction and pain, justifying operative management. The etiology of a rigid flatfoot deformity is diverse. Congenital vertical talus represents the most severe manifestation of rigid pes planus; however, because it is typically diagnosed and treated in infancy, the focus of this masterclass is on the pathologies encountered in older children, adolescents, and adults: the symptomatic accessory navicular, idiopathic rigid pes planus, and tarsal coalition.
Understanding the pathoanatomy and kinematics of the hindfoot is paramount. A rigid deformity alters the normal force distribution across the midfoot and forefoot, leading to adaptive shortening of musculotendinous units, capsular contractures, and eventual degenerative joint disease if left untreated.
Idiopathic Rigid Pes Planus
Idiopathic rigid pes planus is a distinct clinical entity characterized by a stiff, painful flatfoot in the absence of radiographic evidence of tarsal coalition or other structural anomalies.
Luhmann, Rich, and Schoenecker described a cohort of patients presenting with this condition. Demographically, the majority of these patients were in the 95th percentile for weight relative to their age. Clinically, they exhibited an externally rotated gait with an elevated foot-progression angle.
Clinical Pearl: Examination Under Anesthesia (EUA)
In patients with suspected idiopathic rigid pes planus, an examination under anesthesia is a critical diagnostic and prognostic tool. Luhmann et al. demonstrated that out of 13 patients, 9 experienced significant improvement in hindfoot motion under anesthesia, while 4 showed partial improvement. This differentiates structural rigidity from severe musculotendinous guarding.
Management Protocol for Idiopathic Variants
Treatment must be tailored based on the findings of the EUA:
* Mobile Hindfoot under EUA: Indicates that the rigidity is primarily driven by pain and muscle spasm. These patients often respond well to serial casting combined with subtalar corticosteroid injections.
* Persistent Rigidity under EUA: Indicates fixed contractures. These patients may require peroneal fractional lengthening.
* Refractory Cases: If conservative and soft-tissue procedures fail, structural realignment is necessary. This may involve a medializing calcaneal osteotomy or, in severe cases, subtalar arthrodesis. Even with aggressive intervention, long-term outcomes can be guarded; Luhmann noted that only half of the patients achieved complete pain relief and unlimited activity at final follow-up.
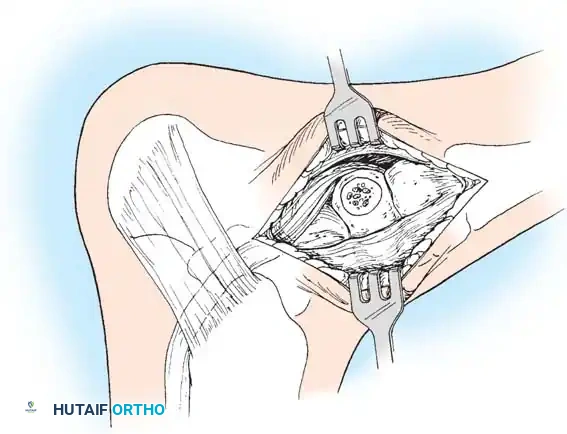
In a parallel study, El Rassi, Riddle, and Kumar evaluated patients presenting with anterolateral hindfoot pain, reduced subtalar mobility, and negative plain radiographs, CT, and MRI. The defining diagnostic feature in their cohort of 19 patients (23 feet) was a positive technetium-99m bone scan, which consistently demonstrated increased radiotracer uptake at the middle facet of the subtalar joint. Surgical exploration revealed a hypervascular, thickened capsule and synovium in this region. Excision of this pathological tissue yielded satisfactory final results in 17 of the 19 patients.
The Accessory Navicular and the Kidner Procedure
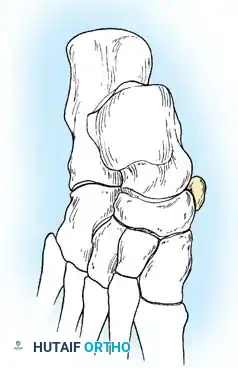
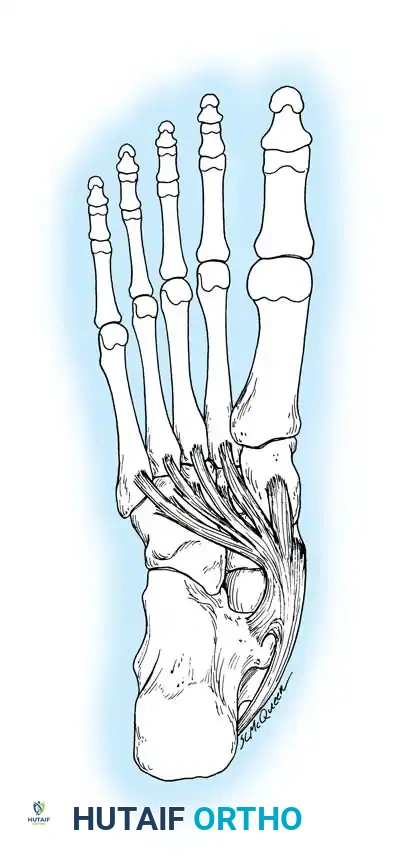
The accessory navicular (os naviculare) is a common accessory ossicle located adjacent to the medial tuberosity of the navicular. When symptomatic, it disrupts the normal insertion and mechanical advantage of the posterior tibial tendon (PTT), contributing to medial arch collapse and rigid pes planus.
The Kidner Procedure involves the excision of the accessory navicular and the transposition/advancement of the PTT to restore its function as a dynamic elevator of the medial longitudinal arch.
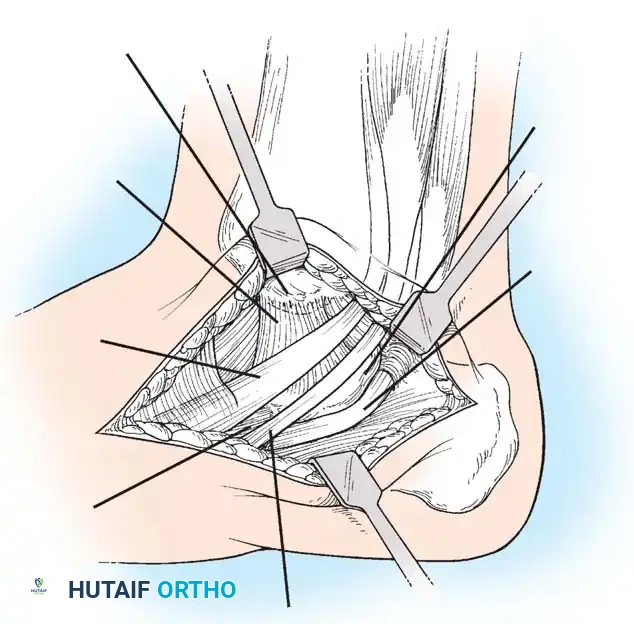
🔪 Surgical Technique 79-6: The Kidner Procedure
1. Incision and Exposure
-
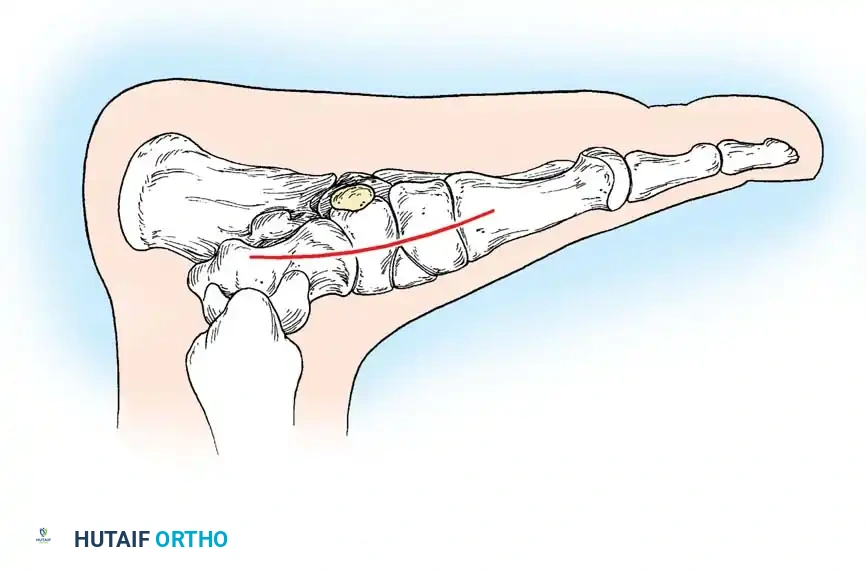
Incision: Begin the skin incision 1 to 1.5 cm inferior and distal to the tip of the medial malleolus. Arch the incision slightly dorsalward, peaking directly over the medial prominence of the accessory navicular, and slope it distally to the base of the first metatarsal.
-
Dissection: Carefully dissect through the subcutaneous tissues. Identify and ligate the plantar communicating branches of the saphenous venous system. Protect the terminal branches of the saphenous nerve.
-
Tendon Identification: Identify the posterior tibial tendon as it approaches the accessory navicular.
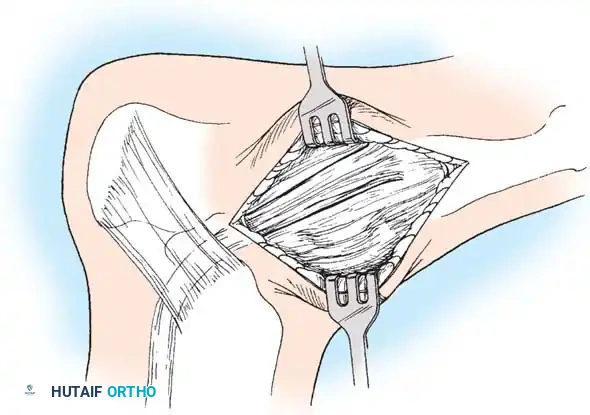

-
Tendon Exposure: Identify the dorsal and plantar margins of the PTT approximately 2 cm proximal to the accessory navicular. Expose the tendon distally, ending at the bone.
Surgical Warning: It is imperative to expose the entire tendon without disturbing the portion extending plantarward toward its multiple insertions on the cuneiforms and metatarsal bases. Preserving these plantar slips maintains the structural integrity of the midfoot.
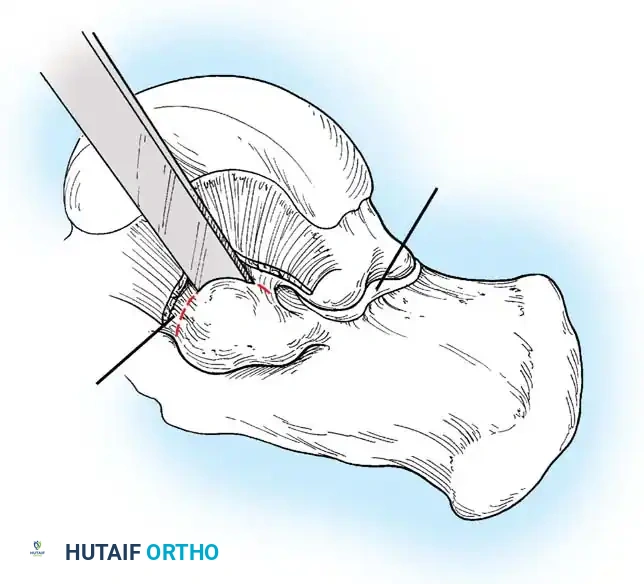
2. Transposition and Advancement of the PTT
-
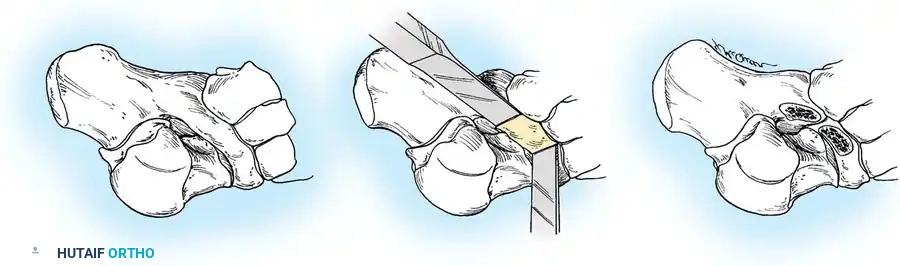
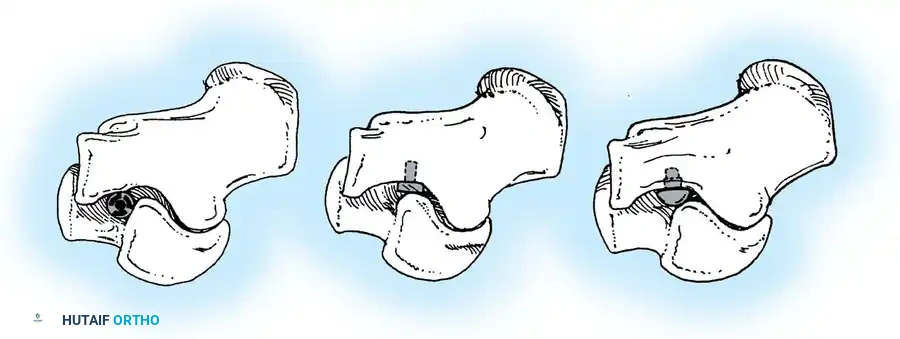
Ossicle Excision: Using sharp dissection, meticulously shell the accessory navicular out from the substance of the posterior tibial tendon. If transposition of the tendon is planned, attempt to leave a microscopic sliver of bone within the tendon to enhance subsequent bone-to-tendon healing.
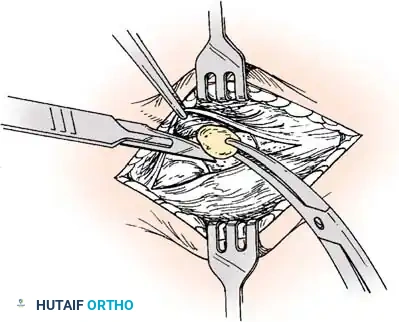

-
Navicular Resection: Resect the medial prominence of the main navicular so that it is flush with the medial border of the first cuneiform. This is typically achieved using an osteotome, followed by a rongeur and rasp to smooth the cortical edges.

-
Tendon Advancement: Suture the PTT to the apex of the medial longitudinal arch. This can be achieved by utilizing local periosteum and ligamentous tissue to secure the transposed tendon slip, or by passing heavy non-absorbable sutures through drill holes placed in the center of the navicular and tying them dorsally.
- Biomechanical Reduction: Try to advance this slip of tendon while the talonavicular joint is anatomically reduced. Reestablish the medial longitudinal arch by holding the midfoot and forefoot in a cavovarus position during knot tying.

3. Skin Closure and Casting
- Closure: Close the subcutaneous tissue and skin with absorbable sutures or adhesive skin strips. A meticulous closure is required as the postoperative cast will remain in place for an extended period.
- Immobilization: Apply a long leg, bent-knee cast in two parts. Ensure the cast is well-padded and gently molded into the longitudinal arch with the talonavicular joint reduced and the foot inverted. The knee should be flexed to 45 degrees to relax the gastrocnemius.
- Alternative Protocol: If the patient is highly reliable and the parents are thoroughly informed, a short leg non-weight-bearing cast with the foot in equinovarus is a reasonable alternative. The cast must remain in place for 4 weeks.
Tarsal Coalition: Pathoanatomy and Genetics
Tarsal coalition is frequently, though somewhat inaccurately, grouped strictly under congenital rigid pes planus. While the anatomical defect is present at birth, symptoms rarely manifest until the cartilaginous bar begins to ossify in late childhood or early adolescence.
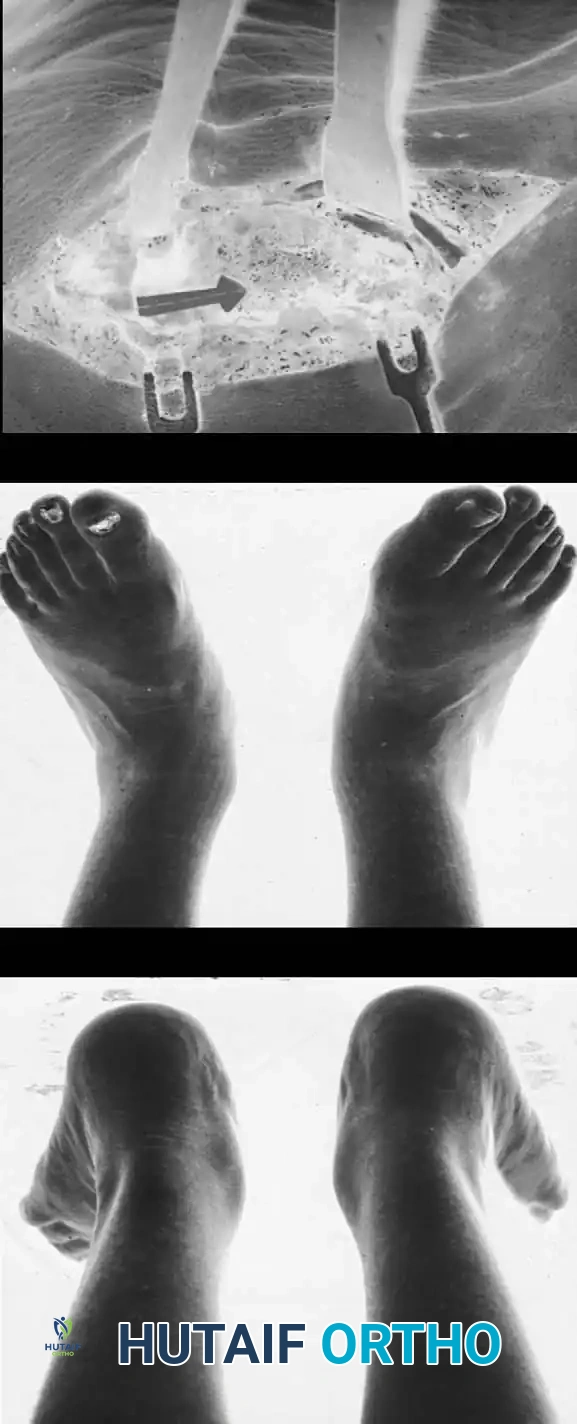
The Myth of "Peroneal Spastic Flatfoot"
Historically, tarsal coalition, rigid pes planus, and peroneal muscle spasm were collectively termed "peroneal spastic pes planus." However, true spasticity (an upper motor neuron sign) is absent. The "spasm" is actually an acquired, adaptive shortening of the musculotendinous units of the peroneal muscles.
When an examiner applies inversion stress to the foot, it elicits an unsustained three- or four-beat clonus—this is simply the stretch reflex of a chronically shortened muscle. According to Lapidus, the relaxed position of the subtalar joint is valgus, which places the least strain on the talocalcaneal interosseous ligament. Through an ill-defined reflex mechanism, the peroneal muscles are stimulated to evert the hindfoot, effectively "decompressing" the subtalar joint. Over time, this everted position becomes fixed.
Diagnostic Pitfall: Peroneal muscle tightness is not pathognomonic for tarsal coalition. It is also seen in rheumatoid arthritis, osteochondral fractures, subtalar infections (tuberculous, mycotic, pyogenic), and adjacent neoplasms (osteoid osteoma, osteochondroma, Trevor disease).
Embryology and Genetics
The etiology of tarsal coalition is almost irrefutably a failure of primitive mesenchyme to segment by cleavage in the 27- to 72-mm fetus, preventing the formation of the normal peritalar joint complex. This hypothesis was definitively demonstrated by Harris in 1955 through the dissection of fetal hindfeet.
Genetically, tarsal coalition behaves as an autosomal dominant trait with reduced penetrance. Wray and Herndon documented a calcaneonavicular bar across three successive generations of men. Leonard's radiographic survey of 31 index patients and 98 first-degree relatives revealed that 39% of the relatives had tarsal coalitions. Strikingly, not a single one of the affected relatives had any history of foot complaints or peroneal spasticity, suggesting that the true incidence of tarsal coalition in the general population is significantly higher than the traditionally quoted 1%.
Clinical Presentation and Radiographic Evaluation
Ossification Timelines
Because the coalition is initially cartilaginous, the malleability of the peritalar complex prevents significant symptoms in early childhood. As the cartilage ossifies, hindfoot stiffness ensues, and the patient's ability to withstand the microtrauma of vigorous activity declines.
* Calcaneonavicular coalitions typically ossify and become symptomatic between 8 to 12 years of age.
* Talocalcaneal coalitions ossify later, typically between 12 to 16 years of age.
The coalition interface may be bony (synostosis), cartilaginous (synchondrosis), or fibrous (syndesmosis). Paradoxically, incomplete coalitions (cartilaginous or fibrous) are often more symptomatic due to micro-motion at the rigid interface.
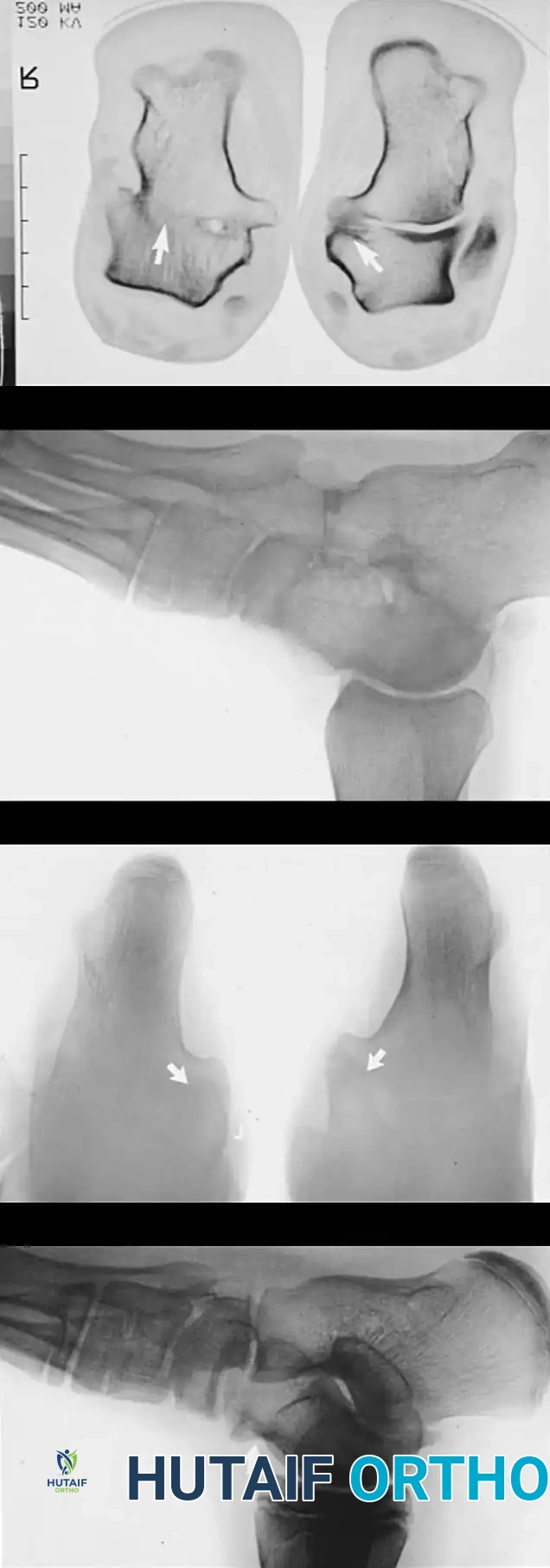
Radiographic Imaging
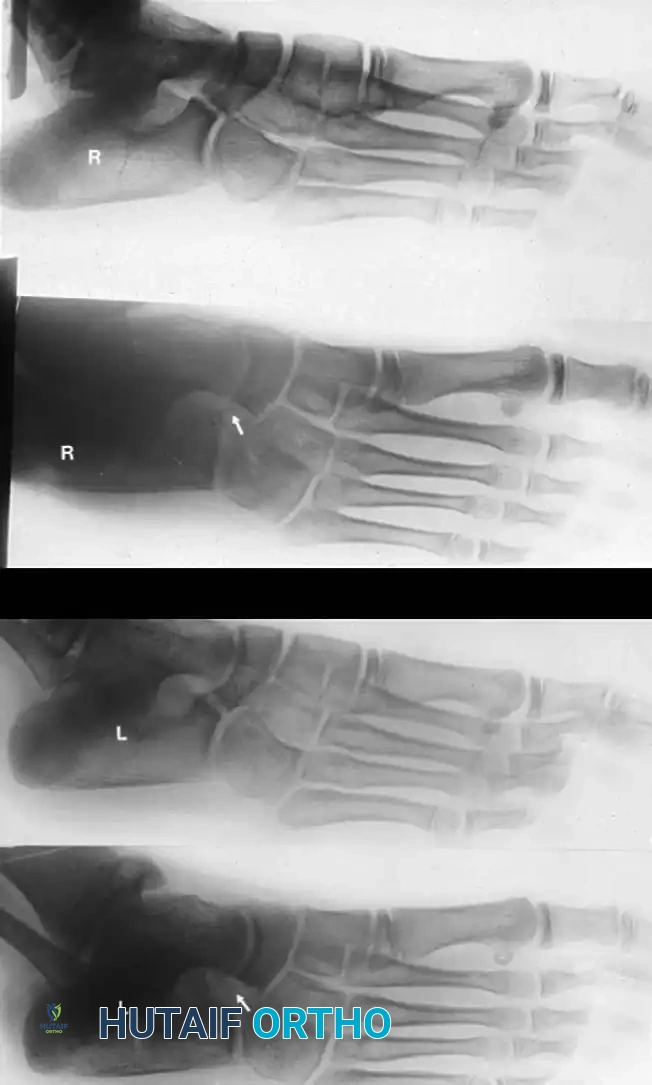
The 45-degree lateral oblique radiograph is the gold standard for diagnosing a calcaneonavicular coalition. The abnormal bar extends from the anterior process of the calcaneus (just lateral to the anterior facet) dorsally and medially to the lateral/dorsolateral extra-articular surface of the navicular. It typically measures 1 to 2 cm in length and 1 to 1.2 cm in width.
In incomplete coalitions, the adjacent bony margins appear irregular, sclerotic, and indistinct. The talar head may also appear small and underdeveloped.
Radiographic Pearl: The "Pseudocoalition"
In older adolescents and adults, a prominent anterior tuberosity of the calcaneus may overlap the navicular on standard views, creating the illusion of a coalition (pseudocoalition). This must be correlated with clinical subtalar motion and dynamic fluoroscopy or varied-angle oblique radiographs.
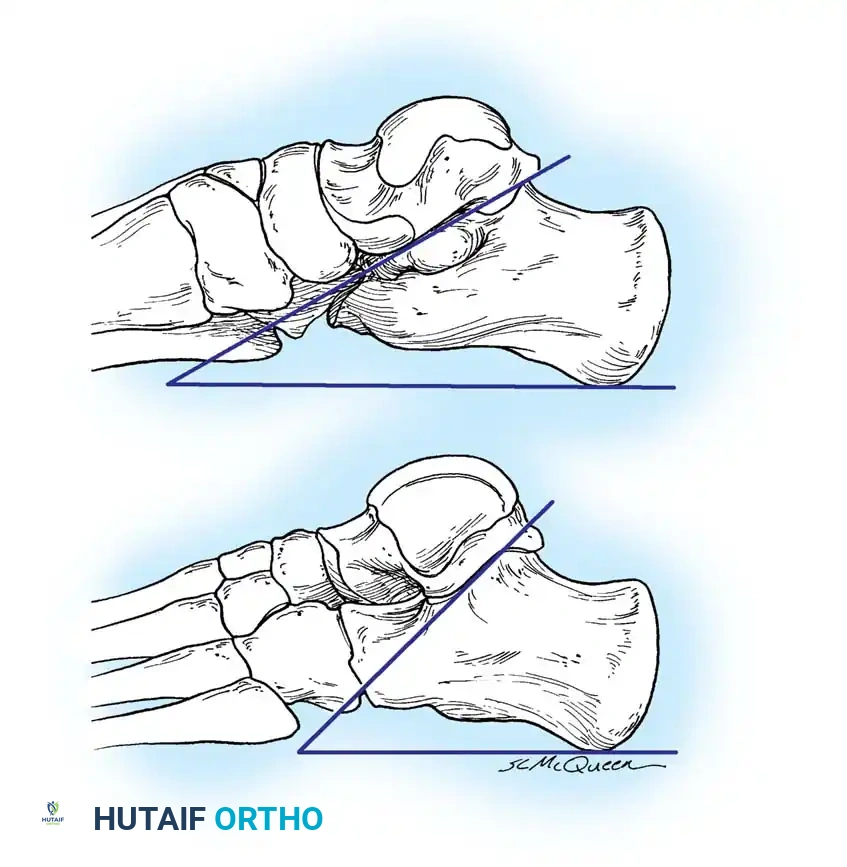
While standard anteroposterior and lateral radiographs may show secondary signs (such as the "anteater nose" sign for calcaneonavicular coalitions or the "C-sign" and talar beaking for talocalcaneal coalitions), advanced imaging is often utilized in modern practice.
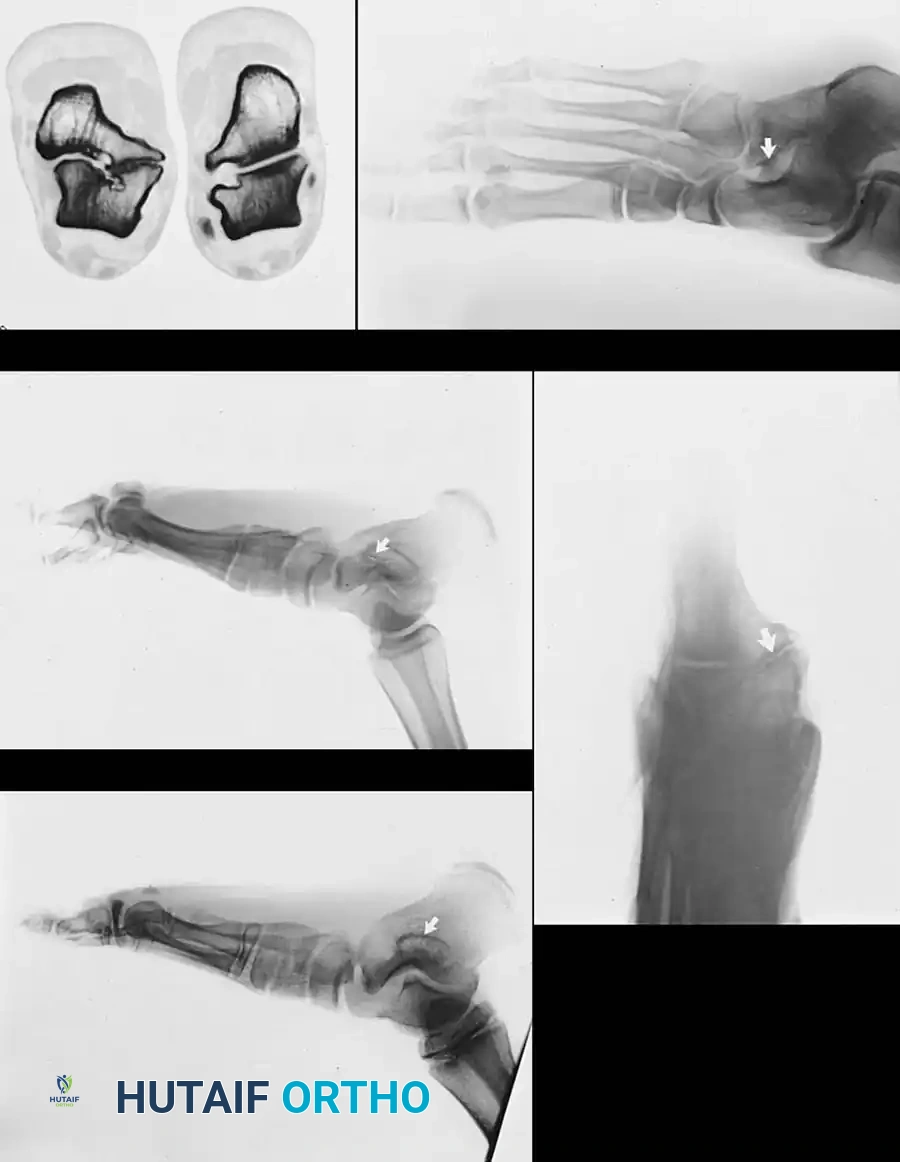
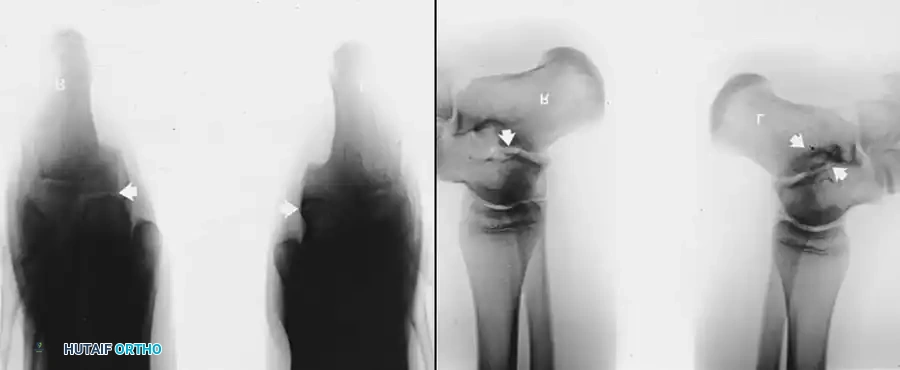
Advanced Imaging and Anatomical Reference Gallery
The following images illustrate various presentations, surgical exposures, and advanced imaging modalities (including CT and MRI correlates) utilized in the comprehensive evaluation and treatment of rigid pes planus and tarsal coalitions: