Complex Revision THA Case Title: Impaction Grafting Success
Patient Presentation & History
A 68-year-old male presented with a 12-month history of worsening right hip pain, progressive limp, and functional decline. He reported mechanical pain, particularly with weight-bearing and initiation of movement, which was not significantly relieved by NSAIDs or activity modification. He had undergone a primary right total hip arthroplasty (THA) 15 years prior for degenerative osteoarthritis. His medical history included controlled hypertension, Type 2 Diabetes Mellitus managed with oral agents, and a remote history of smoking cessation 10 years prior. There was no history of acute trauma, fever, chills, or systemic illness. His BMI was 31. He reported increasing difficulty with activities of daily living, including ambulation beyond short distances, stair climbing, and shoe tying. He denied any symptoms suggestive of neurovascular compromise.
Review of previous operative records indicated an uncemented primary THA with a ceramic-on-polyethylene bearing surface. The patient had an uneventful recovery from his primary surgery and reported excellent function for approximately 10 years, followed by gradual onset of groin and buttock pain that progressively worsened.
Clinical Examination
On initial inspection, the patient walked with a Trendelenburg gait, favoring the right lower extremity, and exhibited a mild fixed external rotation deformity of the right hip. There was no significant limb length discrepancy observed clinically. Surgical scars were well-healed, non-erythematous, and non-tender. There was no local swelling, warmth, or fluctuance.
Palpation revealed diffuse tenderness around the greater trochanter and anterior groin, but no specific point tenderness indicative of bursitis or a specific musculotendinous origin.
Active range of motion (ROM) of the right hip was significantly restricted and painful:
* Flexion: 0-70 degrees (painful at end range)
* Extension: 0 degrees
* Abduction: 0-10 degrees
* Adduction: 0-5 degrees
* Internal Rotation: 0-5 degrees
* External Rotation: 0-15 degrees
Passive ROM mirrored active ROM, with significant discomfort noted at the extremes of motion. There was no mechanical apprehension or obvious instability on provocative testing, though pain limited full assessment.
Neurological examination of the right lower extremity revealed intact motor strength (5/5 in all major muscle groups) and sensation to light touch in L2-S1 dermatomes. Deep tendon reflexes (patellar and Achilles) were 2+ bilaterally. Peripheral pulses (femoral, popliteal, dorsalis pedis, posterior tibial) were palpable and symmetrical. There was no evidence of acute neurovascular compromise. Given the history and radiographic findings, a full workup for potential infection was initiated, including inflammatory markers.
Imaging & Diagnostics
Initial radiographic evaluation included anteroposterior (AP) and lateral views of the right hip and a full-length AP pelvis view. These demonstrated significant findings:
-
AP Pelvis (Right Hip):
- Evidence of severe acetabular osteolysis, particularly in zones 1 and 2, with superior migration of the acetabular component and apparent protrusion into the pelvic cavity. A large lucency around the superior and medial aspects of the cup was clearly visible, consistent with significant bone loss. The uncemented cup appeared loose and significantly displaced.
- The femoral component also showed signs of loosening, with extensive lucency evident at the bone-prosthesis interface along the medial proximal and distal aspects, and evidence of cortical hypertrophy distally, suggesting stress shielding and proximal bone resorption. Minor subsidence was also noted.
- There was no obvious periprosthetic fracture.

Figure 1: Pre-operative AP radiograph demonstrating severe acetabular osteolysis with superior migration of the acetabular component and extensive lucency, consistent with aseptic loosening and significant bone loss.

Figure 2: Magnified view of the acetabulum from the pre-operative radiograph, highlighting the substantial bone defect and component migration.
To further characterize the extent of bone loss and assess for potential intra-pelvic migration or occult fracture, a computed tomography (CT) scan of the pelvis and proximal femur was obtained.
*
CT Scan Findings:
* Confirmed extensive acetabular bone loss, classified as a Paprosky Type IIIb defect, characterized by discontinuity of the acetabular rim, pelvic discontinuity, and significant bone loss extending into the obturator foramen and ischium. The anterior and posterior columns were severely compromised.
* The femoral bone loss was less severe but significant, consistent with a Paprosky Type IIIB defect, showing significant cortical thinning and proximal osteolysis around the stem.
* No acute fracture was identified. The precise extent of the defect was critical for surgical planning.
Inflammatory markers were obtained to rule out periprosthetic joint infection (PJI), given the chronic pain and progressive loosening.
* Erythrocyte Sedimentation Rate (ESR): 45 mm/hr (reference: <20 mm/hr)
* C-Reactive Protein (CRP): 15 mg/L (reference: <5 mg/L)
* White Blood Cell (WBC) count: 7.2 x 10^9/L (normal)
* Differential: Normal
* Joint aspiration was considered but deferred initially due to the high suspicion of aseptic loosening and the planned comprehensive surgical debridement and culture collection. The elevated but not markedly high inflammatory markers were considered equivocal, necessitating intraoperative assessment.
Pre-operative templating was performed meticulously using calibrated radiographs and CT data. This involved:
*
Acetabular Templating:
Assessing optimal cup size, position, and potential need for augmented components or structural allografts to contain the impaction grafting. Consideration of cages or custom triflange components for Paprosky IIIb defects, but the plan leaned towards impaction grafting with reinforcement due to the potential for biological integration.
*
Femoral Templating:
Determining appropriate stem length, diameter, and taper for a cemented revision stem after impaction grafting, aiming for distal fixation and proximal bone support.
Differential Diagnosis
A comprehensive differential diagnosis for a painful, loose revision THA with significant bone loss includes aseptic loosening with osteolysis, periprosthetic joint infection (PJI), and periprosthetic fracture.
| Feature | Aseptic Loosening & Osteolysis | Periprosthetic Joint Infection (PJI) | Periprosthetic Fracture |
|---|---|---|---|
| History | Gradual onset of pain, mechanical in nature, usually years post-op. No systemic symptoms. | Variable onset, acute or chronic pain. May have systemic symptoms (fever, chills, malaise), sinus tract. | Acute onset of pain, often after fall or specific event. Loss of function. |
| Physical Exam | Mechanical pain, limp, restricted ROM. No overt signs of infection. | Pain, warmth, erythema, swelling, tenderness. May have sinus tract. Limited ROM. | Acute pain, deformity, inability to bear weight. Swelling, tenderness. |
| Radiographs | Component migration/subsidence, significant lucency (>2mm), osteolysis, endosteal scalloping. No acute fracture line. | Component loosening (similar to aseptic), but often more rapid progression. May show periosteal reaction. | Fracture line adjacent to or through implant. Possible component migration/dislocation. |
| Inflammatory Markers (ESR/CRP) | Mildly elevated or normal. | Typically significantly elevated. (e.g., CRP >10 mg/L, ESR >30 mm/hr). | Mildly elevated or normal, unless severe soft tissue injury. |
| Synovial Fluid Analysis | WBC <2,500 cells/µL, PMN <65%. | WBC >2,500 cells/µL (or >10,000 for chronic PJI), PMN >65%. Positive culture. | Not indicated unless PJI is also suspected. Usually traumatic effusion. |
| Intraoperative Findings | Avascular, grayish fibrous membrane. Extensive bone loss. | Purulent fluid, inflamed synovium, granulomatous tissue. Pus. | Fracture hematoma, cortical disruption, often implant integrity compromised. |
| Treatment | Revision arthroplasty with bone grafting. | Two-stage revision (debridement, antibiotic spacer, then reimplantation) or one-stage revision in selected cases. | ORIF or revision arthroplasty depending on fracture pattern and implant stability. |
Surgical Decision Making & Classification
Given the patient's severe, chronic pain, significant functional impairment, and radiographic evidence of extensive acetabular and femoral osteolysis with component loosening, operative intervention was deemed necessary. Non-operative management, such as activity modification and analgesics, had failed to provide sufficient relief and would not address the underlying structural integrity issues. The risk of further bone destruction, intra-pelvic migration, or catastrophic failure necessitated surgical revision.
The extent of bone loss dictated the complexity of the revision. We utilized the Paprosky classification system for both acetabular and femoral bone defects:
-
Acetabular Classification: The CT scan confirmed a Paprosky Type IIIb defect . This severe classification implies:
- Loss of the superior acetabular dome.
- Disruption of both anterior and posterior columns.
- Significant pelvic discontinuity, often extending to the ischium or pubis.
- Lack of host bone to support a conventional uncemented cup.
- This classification strongly indicated the need for advanced reconstructive techniques, such as impaction grafting with a cemented cup, a cage, or a custom triflange component. Impaction grafting was chosen as it offers the potential for biological integration and long-term reconstitution of host bone stock.
-
Femoral Classification: The CT scan and radiographs indicated a Paprosky Type IIIB defect . This signifies:
- Extensive proximal femoral bone loss, often circumferential.
- Compromise of cortical bone and medullary canal integrity.
- Inability to achieve stable primary fixation with a standard uncemented stem.
- Impaction grafting with a cemented stem was considered the most viable option to restore the proximal femoral metaphysis and achieve stable stem fixation, aiming for distal diaphyseal engagement.
The decision for impaction grafting was based on its established success in managing significant bone defects in revision THA. This technique offers several advantages:
1.
Biological Reconstruction:
Uses morselized allograft to recreate bone stock, allowing for biological incorporation and potentially long-term stability.
2.
Versatility:
Adaptable to various defect types, both acetabular and femoral.
3.
Restoration of Biomechanics:
Allows for restoration of hip center of rotation and leg length, which can be challenging with other reconstruction methods.
4.
Long-term Durability:
Successful impaction grafting can lead to durable constructs with graft incorporation and remodeling.
Surgical Technique / Intervention
The patient was positioned in the left lateral decubitus position on a standard operating table, allowing for ample access to the right hip. A standard posterior approach was utilized.
1. Component Removal and Debridement:
- The original posterior incision was re-opened. The fascia lata was incised, and the gluteus maximus fibers were split.
- The short external rotators were carefully detached from the greater trochanter, and the posterior capsule was excised.
- The femoral head was dislocated. Significant inflammatory fibrous tissue and pseudomembrane were noted around the loose acetabular and femoral components.
- Intraoperative tissue samples (at least 5-6) were sent for aerobic and anaerobic cultures, histopathology, and alpha-defensin testing to definitively rule out PJI.
-
The uncemented acetabular cup was carefully extracted using osteotomes and specialized cup removal tools. This revealed the extent of the Paprosky IIIb defect, with the superior and medial walls completely deficient, and exposure of intra-pelvic structures.

Figure 3: Intraoperative view of the acetabular defect after removal of the primary component, demonstrating severe superior and medial bone loss, consistent with Paprosky Type IIIb. -
The femoral stem was then extracted. Due to severe osteolysis around the proximal stem, this was achieved with relative ease. The femoral canal was meticulously cleaned of any remaining cement or fibrous tissue.
2. Acetabular Impaction Grafting:
-
Containment: The significant pelvic discontinuity and medial wall defect necessitated robust containment. A titanium mesh was contoured to bridge the medial wall defect and secure it to existing host bone around the periphery of the defect, providing a stable floor for impaction. An obturator plate was fixed anteriorly and inferiorly for further containment.

Figure 4: Intraoperative view of the acetabular defect with a titanium mesh applied to contain the medial wall defect and a plate used for anterior/inferior support. -
Graft Preparation: Fresh-frozen, morselized cancellous allograft bone chips (typically 4-10 mm in size) were prepared. These chips were mixed with autologous bone marrow aspirate from the greater trochanter to enhance osteoinductive and osteoconductive properties.
-
Impaction: The grafting process commenced with careful, sequential impaction of the morselized allograft into the defect. Layers were built up incrementally, starting peripherally and working towards the center. Specialized impactors and mallets were used to achieve high-density compaction of the graft, ensuring a stable, structurally sound bed. The goal was to recreate a spherical acetabular cavity.

Figure 5: Sequential impaction of morselized allograft bone chips into the acetabular defect using a spherical impactor. -
Reaming and Final Impaction: Sequential reaming was performed through the compacted graft, gradually increasing in size until appropriate tension and stability were achieved with a trial liner. This ensured a perfectly spherical, densely packed acetabular cavity, ready for the definitive cup.

Figure 6: Reaming through the compacted allograft to create a perfectly spherical acetabular cavity, preparing for cementation. -
Cemented Cup Insertion: A conventional polyethylene acetabular cup (cemented type) was then cemented into the densely impacted allograft. The cement mantle was meticulously applied under pressure, ensuring interdigitation with the compacted graft particles.

Figure 7: The cemented polyethylene acetabular cup inserted into the reconstructed acetabulum, demonstrating good position and cement mantle.
3. Femoral Impaction Grafting:
-
Canal Preparation: The femoral canal was thoroughly curetted and debrided. The extent of bone loss necessitated significant reconstruction of the proximal femur.

Figure 8: Intraoperative view of the femoral canal after stem removal, showing proximal femoral bone loss and cortical thinning. -
Containment: Distal plugging of the femoral canal was performed to create a contained cavity for the graft. In some cases of extensive proximal defect, a mesh or cerclage wires may be used to provide external containment for the proximal bone bed, though not explicitly shown in this sequence.
- Graft Impaction: Similar to the acetabulum, morselized allograft bone chips were sequentially impacted into the femoral canal. Specialized femoral impactors were used to create a solid, stable column of compacted graft, rebuilding the proximal metaphysis and providing a stable bed for the cemented stem.
-
Stem Trialing and Cementation:
Revision femoral stems with various lengths and diameters were trialed to ensure appropriate fit, fill, and restoration of leg length and offset. Once the ideal stem size and version were determined, the stem was cemented into the impacted allograft. A standard technique for cementing revision stems was employed, ensuring a good cement mantle and pressurization.
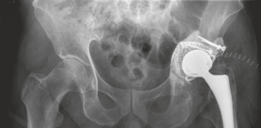
Figure 9: Intraoperative view of femoral impaction grafting with morselized allograft, with a trial femoral stem in place to assess fit and stability.

Figure 10: The definitive cemented femoral stem inserted into the reconstructed femoral canal after impaction grafting.
4. Reduction and Closure:
- The trial femoral head and liner were used to reduce the hip. Stability was meticulously assessed through a full range of motion, with particular attention to flexion, adduction, and internal rotation, as well as extension, abduction, and external rotation. No impingement or instability was noted.
- The final ceramic femoral head and polyethylene liner were inserted.
- The short external rotators were repaired if possible, or the posterior capsule was reconstructed. The gluteus maximus was reapproximated, and the fascia lata, subcutaneous tissues, and skin were closed in layers.
- A suction drain was placed.
Post-Operative Protocol & Rehabilitation
1. Immediate Post-Operative Period (Day 0-3):
- Weight-Bearing: Touch-down weight-bearing (TDWB) or toe-touch weight-bearing (TTWB) on the operative extremity for the first 6-12 weeks, as bone graft incorporation is critical.
- DVT Prophylaxis: Low molecular weight heparin (LMWH) or oral anticoagulants initiated immediately and continued for 4-6 weeks post-operatively.
- Pain Management: Multimodal analgesia including epidural/nerve blocks, oral opioids, NSAIDs (if not contraindicated), and acetaminophen.
- Wound Care: Drain typically removed within 24-48 hours. Daily dressing changes, monitoring for signs of infection.
-
Physical Therapy (PT):
- Day 1: Initiate gentle active-assisted range of motion (AAROM) exercises within protected arcs. Ankle pumps, quad sets, gluteal sets.
- Hip Precautions: Strict adherence to posterior hip precautions (avoiding flexion >90 degrees, adduction past midline, internal rotation).
- Mobilization: Transfers to chair, commode with assistance. Progressive ambulation with assistive devices (walker) maintaining TDWB/TTWB.
2. Early Rehabilitation (Weeks 1-6):
- PT Focus: Progressive strengthening of hip abductors, extensors, and quadriceps. Continuation of ROM exercises within precautions.
- Gait Training: Progression from walker to crutches, maintaining protected weight-bearing.
- Activities of Daily Living (ADLs): Training for independence in dressing, bathing, and transfers.
- Imaging: Follow-up AP pelvis and lateral hip X-rays at 6 weeks to assess component position and early signs of graft incorporation.
3. Intermediate Rehabilitation (Weeks 6-12):
- Weight-Bearing Progression: Gradually advance weight-bearing to partial weight-bearing (PWB) as radiographic signs of graft consolidation become evident and pain allows. Full weight-bearing typically allowed after 12 weeks, upon clear radiographic evidence of graft healing and stability.
- PT Focus: Continued strengthening, balance, and proprioceptive exercises. Gradual increase in ambulation distance.
- Imaging: X-rays at 3 months post-op to monitor graft integration and component stability.
4. Long-Term Rehabilitation (Months 3-12+):
- PT Focus: Advanced strengthening, functional exercises, return to recreational activities as tolerated. Gradual weaning from assistive devices.
- Hip Precautions: May be relaxed somewhat for posterior approach patients once tissues are well-healed and strength is optimized, but patient education on safe movement patterns remains crucial.
- Follow-up: Clinical and radiographic follow-up at 6 months, 1 year, and annually thereafter for the first 5 years, then biannually. Look for signs of graft resorption, new lucencies, or component migration.
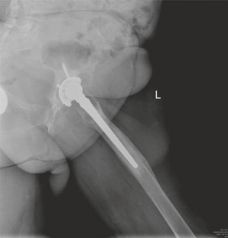
Figure 11: Immediate post-operative AP radiograph showing the well-positioned cemented acetabular cup and cemented femoral stem after impaction grafting, with restoration of the hip center of rotation and leg length.

Figure 12: Follow-up AP radiograph at 6 months, demonstrating early signs of graft incorporation and stable components.

Figure 13: Follow-up AP radiograph at 1 year, showing excellent graft remodeling and complete incorporation, with no signs of lucency or component migration.

Figure 14: Follow-up AP radiograph at 2 years, confirming stable components, complete graft integration, and successful long-term reconstruction of bone stock.
Pearls & Pitfalls
Pearls (Crucial for FRCS/Board Exams):
- Pre-operative Planning is Paramount: Meticulous templating using calibrated radiographs and CT scans is essential for assessing bone defect type (Paprosky classification), determining graft volume, and selecting appropriate components (containment devices, stem length/diameter, cemented vs. uncemented).
- Allograft Selection and Preparation: Use high-quality, fresh-frozen morselized cancellous allograft (typically 4-10mm). Consider mixing with autologous bone marrow aspirate or demineralized bone matrix to enhance osteoinductive properties. Avoid finely ground graft as it compacts poorly and is less osteoconductive.
- Defect Containment: Achieving a contained defect is critical for successful impaction grafting. This may require anti-protrusion cages, acetabular reconstruction cages, customized titanium mesh, or structural allografts (e.g., femoral head). For femoral defects, distal plugging is essential.
- Sequential Impaction: Build up the graft in thin, sequential layers (2-3mm), starting peripherally and working centrally. Use dedicated impactors that match the geometry of the defect. Each layer must be thoroughly impacted to create a dense, stable bone bed. "Every tap counts."
- Achieve Stability & Spherical Cavity: For acetabular defects, the final reaming through the impacted graft must create a perfectly spherical and stable cavity that matches the chosen cup size. For femoral defects, the compacted graft should be stable enough to support the cemented stem.
- Cementation Technique: Utilize modern cementing techniques (e.g., retrograde filling, pressurization, vacuum mixing) to ensure a high-quality cement mantle that interdigitates effectively with the compacted graft particles for robust mechanical interlock.
- Limb Length & Offset Restoration: Use trial components to accurately restore leg length, hip center of rotation, and femoral offset to optimize biomechanics and reduce impingement/dislocation risk.
- Post-operative Protected Weight-bearing: This is non-negotiable, especially for large defects. Early, unprotected weight-bearing can lead to graft migration, subsidence, or collapse, compromising the entire construct.
Pitfalls (Crucial for FRCS/Board Exams):
- Inadequate Containment: Failure to create a contained defect can lead to graft migration, extrusion, or lack of proper impaction, resulting in an unstable construct and early failure.
- Poor Graft Impaction: Insufficient impaction results in a loose, non-structural graft that will subside or resorb, leading to aseptic loosening of the components. Over-impaction can damage host bone.
- Infection: Despite thorough intraoperative sampling, unrecognized low-grade infection can lead to graft failure, delayed healing, and eventual loosening. Aseptic technique throughout the procedure is vital.
- Neurovascular Injury: Complex revision THA carries an increased risk of injury to the sciatic nerve, femoral nerve, or major vascular structures, especially with extensive osteolysis and distorted anatomy. Careful dissection and awareness of anatomical landmarks are paramount.
- Periprosthetic Fracture: During component removal or impaction, there is a risk of iatrogenic fracture, particularly in osteoporotic or osteolytic bone. Meticulous technique and appropriate instrumentation are crucial.
- Dislocation: Impaction grafting can alter the hip's biomechanics. Failure to restore leg length, offset, or maintain proper component orientation can lead to recurrent dislocation.
- Graft Resorption/Non-incorporation: While rare with good technique, the allograft may fail to incorporate or may resorb over time, leading to late aseptic loosening. This is why protected weight-bearing and close follow-up are critical.
- Stem Subsidence/Migration: For femoral impaction grafting, if the distal canal preparation or graft compaction is inadequate, the cemented stem may subside, leading to loss of fixation.
