DEFINITION
Replantation is the reattachment of a completely amputated body part. Revascularization is the restoration of circulation and repair of all injured structures in an incompletely amputated, dysvascular body part. Revascularization always includes repair of blood vessels to reestablish blood flow to the part.Revision amputation is the procedure performed at the site of amputation to gain soft tissue coverage and to address concomitant injuries to the digit.The decision of whether to perform replantation or revascularization and revision amputation of a digit is multifactorial. The relative indications and contraindications for each are discussed later in the chapter.
ANATOMY
An understanding of the anatomy over the complete length of the digit is essential for successful replantation. The anatomy of the thumb is different from that of the four fingers.Palmar and dorsal cutaneous ligaments maintain the position of the neurovascular bundle during range of motion of the digit.Grayson ligament is palmar to the neurovascular bundle, originates from the flexor tendon sheath, and inserts on the skin.Cleland ligament travels dorsal to the neurovascular bundle from the phalanx to the overlying skin.A radial and ulnar proper digital artery supplies each digit. Each vessel travels with a respective radial and ulnar proper digital nerve. At the level of the digit, the artery lies dorsal to the nerve.The ulnar digital artery is typically larger in the thumb and index fingers. The radial digital artery usually is larger in the small finger.Three major palmar arches arise from the digital arteries. The proximal, middle, and distal arches are consistently located at the level of the C1 pulley, C3 pulley, and just distal to the flexor digitorum profundus (FDP) insertion, respectively.Four palmar and four dorsal branches usually extend from each digital artery.Injection studies have demonstrated that the venous system of the digit consists of a series of arcades on thedorsal and palmar surfaces, with connecting oblique and transverse anastomotic veins.10 The dorsal veins have a larger caliber than the palmar veins, which do not consistently travel with the digital artery and nerve.A radial and ulnar proper digital nerve travels with each proper digital artery. The digital nerve is sensory only and typically contains one to three fascicles. It trifurcates at the level of the distal interphalangeal (DIP) joint.Each finger has two flexor tendons within the flexor tendon sheath. The FDP tendon inserts at the proximal base of the distal phalanx.The flexor digitorum superficialis (FDS) tendon inserts as two slips into the midportion of the middle phalanx.The FDS tendon splits into two slips, and its relative position to the FDP tendon switches from palmar to dorsal at Camper chiasm. This allows the deeper FDP tendon to continue to its more distal insertion.There are a series of five annular and three cruciform pulleys, which are discrete thickenings of the fibro-osseous sheath. The annular pulleys prevent bowstringing of the flexor tendons during flexion, whereas the cruciate pulleys are collapsible, accommodating flexion.The odd-numbered annular pulleys are located over the joints of the finger, and the even-numbered annular pulleys are over the proximal and middle phalanx, respectively.The A2 and A4 pulleys are most important in preventing bowstringing and should be preserved if possible.Each lesser digit receives a tendon from the extensor digitorum communis (EDC). The index and small fingers each have a second extensor tendon, the extensor indicis proprius (EIP) and extensor digiti minimi (EDM), respectively. Both of these tendons are ulnar to the EDC tendons.
PATHOGENESIS
The mechanism of injury has a considerable effect on the potential for replantation. Sharp amputations are ideal for replantation because of the narrow zone of injury.The degree of tissue injury increases substantially with crush and avulsion mechanisms and may prohibit successful replantation (FIG 1).Most digit amputations occur as an isolated injury. When amputations occur in the multiply injured patient, consideration of other systemic injuries and adherence to advanced trauma life support (ATLS) protocols may prevent replantation.
NATURAL HISTORY



FIG 1 • A. This hand sustained sharp amputation of the digits from a table saw. The narrow zone of injury made the digits ideal for replantation. B. This hand sustained a crush injury. The resultant wide zone of injury prohibited successful replantation. Expected survival rates of replanted digits are 80% or higher, with even higher survival rates in revascularized digits.
PATIENT HISTORY AND PHYSICAL FINDINGS


FIG 2 • The amputated part should be wrapped in a sterile gauze moistened with Ringer lactate or normal saline. The gauze is then placed in a leakproof plastic bag, which is placed on ice. The part should never be placed directly on ice.
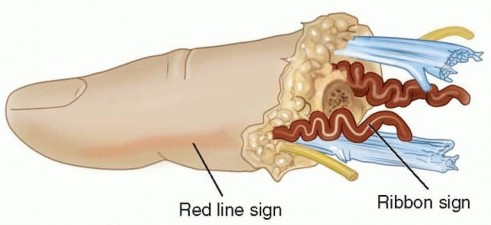
FIG 3 • The red line sign, which represents an avulsion injury, is seen clinically as a red streak of ecchymosis along the lateral border of the digit. This ecchymosis is the result of hemorrhage from avulsed branches of the digital artery after a traction injury. The ribbon sign, which also represents an avulsion injury, refers to the corkscrew appearance of the digital artery resulting from disruption of the vessel wall layers. When these clinical signs are present, the zone of injury must be bypassed with vein grafts if replantation is attempted.Theribbon signalso represents an avulsion injury (see FIG 3). Coiling of the artery at the amputation siteresults from disruption of the vessel wall layers from traction.17 If replantation is attempted, vein grafting is often required.
IMAGING AND OTHER DIAGNOSTIC STUDIES
When the patient arrives in the emergency department, standard radiographs of the amputated parts and the injured limb are obtained (FIG 4).Laboratory evaluations should include a complete blood count, basic metabolic panel, coagulation panel, drug screen, and blood type and crossmatch. Other preoperative tests are ordered as indicated by the patient's age and comorbidities.
NONOPERATIVE MANAGEMENT


FIG 4 • A. Standard posteroanterior (PA) radiograph of the injured hand. B. A radiograph of the amputated parts is also obtained by placing the bag containing the parts directly on the x-ray cassette.
SURGICAL MANAGEMENT
The decision to replant a digit is predicated on the determination that the anticipated function after replantation will be better than that of a revision amputation. This determination is made after careful consideration of the factorsinfluencing the predicted survival of the replanted digit, morbidity to the patient, and functional outcome. Specific factors related to the status of the amputated part and the status of the patient include the following:Mechanism of injury (eg, sharp, crush, avulsion) Level of amputationIschemia time (warm or cold) Health of patientAge of patientPresence of segmental injury Predicted rehabilitation Vocation and hobbiesInformed consent for replantation versus revision amputation must reference the postoperative care differences.Patients undergoing revision amputation typically are discharged from the hospital much quicker and have much shorter, less intensive rehabilitation protocols.Patients treated by replantation typically require a 5- to 7-day hospital course, avoidance of smoking and caffeine, possible blood transfusions, and prolonged rehabilitation. Furthermore, these patients must be advised about the likelihood of cold intolerance.The techniques we use for replantation of amputated digits are described in detail in the following sections. The same techniques and sequence of repair are followed for the revascularization of partially amputated parts.In partial amputations, not all structures will be injured, so it may be that only some structures require repair. For example, if the dorsal skin and its veins remain intact, the procedure does not require venous anastomosis for outflow.Each case should be examined individually, and all structures should be carefully evaluated for injury.
PREOPERATIVE PLANNING
Broad-spectrum antibiotics and tetanus prophylaxis are administered on presentation in the emergency department.The patient, hand, and amputated parts are examined to confirm suitability for possible replantation. A urethral catheter should be placed for long procedures.Regional anesthesia is preferred to facilitate autonomic blockade, which results in increased peripheral vasodilation. Ideally, an indwelling catheter is placed to allow for continuous postoperative pain relief and sympathetic block. General anesthesia is required for children.If an attempt at replantation is determined to be appropriate and desired, the parts are brought to the operating room as soon as possible. Initial preparation of the parts can begin while the anesthesia team evaluates the patient.The operating room and patient must be kept warm to prevent peripheral vasoconstriction. The sequence of repair is as follows:Débridement and identification of structures Bone shortening and fixationExtensor tendon repairFlexor tendon repairArterial repair Nerve repair Vein repairSkin closure/coverageP.1139
POSITIONING
The patient is positioned supine on a standard operating room table with a hand table attachment. The table is rotated 90 degrees to allow access for the operating microscope and fluoroscopy.
APPROACH
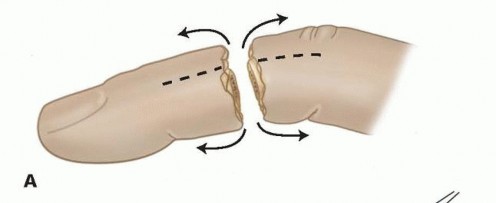
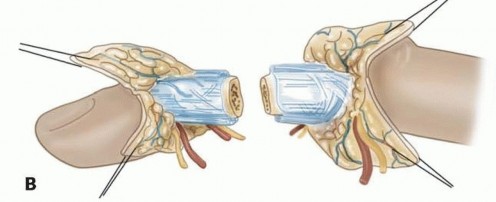
FIG 5 • A,B. Bilateral longitudinal midaxial incisions allow for easy exposure of the neurovascular bundles and dorsal veins.
TECHNIQUES
PREPARATION OF THE AMPUTATED PART
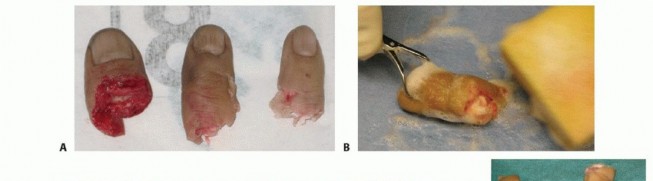

TECH FIG 1 • A,B. The amputated parts are removed from the bag, and a sterile prep is performed on a separate table. C. A sterile metal irrigation basin is filled with ice and covered with a sterile adhesive drape. Use as much ice as can be placed without disruption of the sterile environment to maximize contact with the amputated parts. D. A sterile surgical towel is then placed over the drape and used as a working surface. E. Nylon sutures placed through the amputated parts are secured to the surgical towel. The amputated parts are now ready for débridement and preparation.


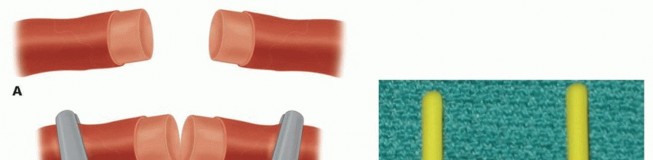
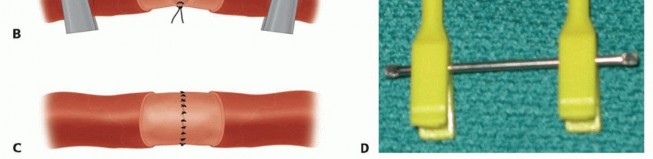
TECH FIG 2 • A. A Tajima-type suture repair is used so that the flexor tendons can be opposed and secured at the ideal time. B,C. The suture is placed in the proximal and distal ends of the tendon. D. The sutures are then tied in the repair site at the appropriate time.


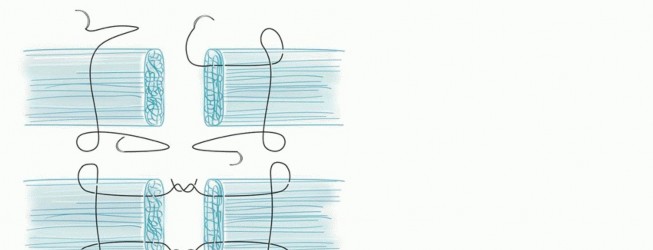
TECH FIG 3 • A-D. Parallel longitudinal K-wires allow for easy and rapid fixation with low complication rates.(continued)
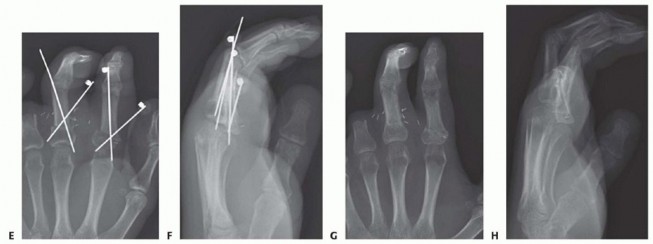
TECH FIG 3 •(continued)E-H. In more proximal amputations, longitudinal K-wires may not be possible. Crossed K-wires can be used successfully in these injuries.
TECH FIG 4 • A-C. Arterial repair is performed using the operating microscope. A tension-free anastomosis of normal intima to normal intima is essential for survival of the replanted part. D. The vascular approximating clamp should have less than 30 g of closing pressure. Two clamps on a sliding bar allow for tension-free positioning of the vessel ends. If adequate blood flow is not obtained, evaluate for all reversible causes of vasospasm, including hypotension, hypovolemia, acidosis, pain, or cold. Double check that the tourniquet was deflated.Evaluate the proximal vessel for mechanical constriction.Thoroughly irrigate the lumen with warm heparinized Ringer lactate through a 30-gauge blunt-tipped needle on a 10-mL syringe.If vasospasm persists, irrigate the proximal vessel with papaverine solution (diluted 1:20 with sterile normal saline).After appropriate blood flow is established, the proximal and distal stumps are placed within the vascular approximators. Several types of approximating devices are available. We favor two clamps on a sliding bar. The clamps should have less than 30 g of closing pressure and should be limited to no more than 30 minutes of application time due to the potential for vessel damage (TECH FIG 4D).Place a microsurgical background deep to the repair site.A bolus of 3000 to 5000 U of intravenous heparin is given just before the anastomosis. After the bolus, we typically initiate a heparin drip at 1000 U per hour.Repeat inspection of the intima is performed proximally and distally to confirm its integrity. Verify that the anastomosis is tension-free and that no adventitia overhangs the lumen.Appropriately sized monofilament nylon sutures (Table 1) are used and initial sutures are placed 180 degrees apart.The size of each “bite” should be about one to two times the thickness of the arterial wall. Care must be taken to avoid damaging the intima of the vessel.One limb each of the initial sutures should be cut long for use in manipulating the vessel without directly handling it.Suture the front wall of the artery sequentially between stay sutures.Irrigate the lumen after each suture is tied, and inspect the repair site to confirm that the back wall was not captured.Flip the approximating clamp to expose the back wall and complete the anastomosis.Remove the vessel from the approximating clips and repeat the procedure on the other digital artery.Site of Repair|Suture Size|Needle Size (μm)------Palm|9-0|100Proximal digit|10-0|75Distal digit|11-0|50 Table 1 Needle and Suture Sizes
NERVE REPAIR
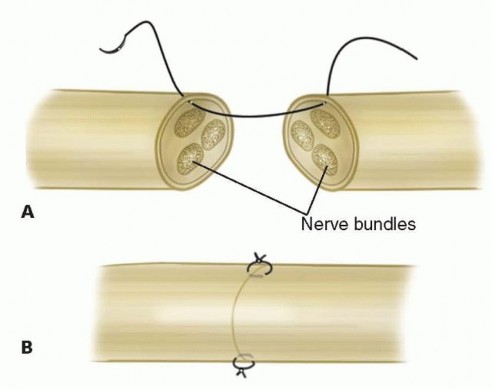
TECH FIG 5 • A,B. The digital nerve is approximated using an epineurial repair consisting of two or three sutures.
VEIN REPAIR
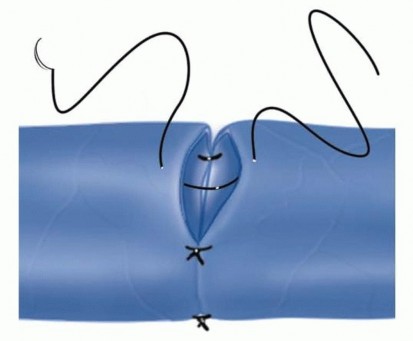
TECH FIG 6 • The venous anastomosis is performed with fewer sutures than the arterial repair due to the low-pressure flow. Familiarity with alternatives to venous anastomosis is necessary in the event suitable veins cannot be located.Continuous venous oozing can be encouraged by removal of the nail with subsequent scraping of the matrix. This scraping is performed every 2 hours with a cotton-tipped applicator and is followed by the application of heparinsoaked pledgets.If proximal veins are present but distal veins are not, creation of either an arteriovenous or venocutaneous fistula may facilitate outflow to reduce congestion. This scenario is most common in very distal amputations just proximal to the nail. An arteriovenous fistula may be created possibly if one artery has been successfully repaired and back bleeding is present from the other distal artery. This artery can be anastomosed to the proximal vein. Alternatively, a vein graft can be used to create a temporary shunt from the skin of the pulp to the proximal vein.Medicinal leeches (Hirudo medicinalis) can be placed on the engorged part if postoperative venous congestion occurs. They should be changed every few hours and should be used for a minimum of 7 days to allow for the establishment of collateral circulation. Although the leeches may fall off after engorgement, they secrete hirudin, a local anticoagulant that keeps the digit bleeding for 8 to 12 hours. While using leech therapy, the patient should be treated with a third-generation cephalosporin as prophylaxis againstAeromonas hydrophila infection, a symbiotic gram-negative rod in the leech gut.1. Skin Coverage and Wound ClosureBefore the wound is closed, meticulous hemostasis must be achieved. Even small postoperative hematomas can compress the vascular repairs and result in failure of the replant.Interrupted nylon sutures are used to close the wounds, avoiding constriction of underlying structures. The midlateral incisions can be left open without concern for healing difficulties. If the repaired dorsal veins lack local coverage, a split- or full-thickness graft should be applied.No part of the postoperative dressing should be circumferential. Small strips of petroleum-impregnated gauze are applied to the incisions. A bulky dressing is constructed with a plaster splint extending above the elbow. The tips of all digits must remain exposed, and a temperature probe is taped to the pulp of the replanted digit for monitoring.The limb is elevated in a foam pillow.
PEARLS AND PITFALLS
Amputatedparts1. Take the amputated parts to the operating room to begin débridement andidentification of structures as soon as the room is ready.Heterotopicreplantation1. Prioritize the functional goals for replantation. If multiple digits are amputated, but notall parts are suitable for replantation, put the salvageable digits in the most functional position (eg, replant a finger in the thumb position if the thumb cannot be saved).Vein grafts1. If there is concern for intimal damage, resection and the liberal use of vein graftssaves time and frustration. Always reverse the vein graft in case valves are present in the segment. The volar aspect of the wrist contains numerous veins 1-2 mm in diameter.Spare partssurgery1. Never discard any amputated parts until the conclusion of the case. Amputated partsthat are not suitable for replantation are an ideal source of autologous grafts.Vascularanastomosis1. Never perform an anastomosis under tension. Either additional bone shortening orvein grafting should be performed.Multiple digit ▪ The overall duration of surgery is decreased by performing a structure-by-structurereplantations repair instead of a digit-by-digit repair (ie, repair the same anatomic structure in alldigits before repairing the next structure).3P.1145
POSTOPERATIVE CARE
Usually, the hand is elevated, with the level of elevation adjusted for changes in vascular status. If arterial inflow becomes problematic, the hand is lowered. If venous congestion is present, the hand is raised.Color, warmth, turgor, and capillary refill are monitored by the surgeon.The patient's room should be kept warm, preferably above 22° C (72° F). The temperature probe is monitored by the nursing staff, and the surgeon is notified if the digital temperature is less than 30° C or if the temperature drops 2° C over 1 hour.The patient is maintained on bed rest for the first 2 or 3 days, and the room is kept dark with minimal stimulation. Visitors are limited to two at a time.The patient is restricted from nicotine and caffeine products.The intravenous heparin drip is continued at 1000 U per hour. The rate is adjusted for a goal activated partial thromboplastin time (aPTT) of 1.5 times normal. It is maintained for 5 days, then weaned by 100 U per hour until off.Dextran 40 is given as a 50-mL bolus and then maintained at a rate of 20 mL per hour while the patient is in the hospital.Enteric-coated aspirin (325 mg daily) and dipyridamole (50 mg three times a day) are initiated and maintained for 6 weeks postoperatively.Chlorpromazine (25 mg orally every 8 hours) is useful as both an anxiolytic and a peripheral vasodilator. We generally use it for the duration of the patient's hospital stay.Appropriate antibiotics are maintained for 7 days.We prefer to leave the operative dressing in place for 7 days to avoid causing vasospasm. Excessive bleeding with formation of a blood cast that would restrict venous outflow should prompt an earlier dressing change.Gentle active motion is started on postoperative day 3 within the confines of the splint. Formal hand therapy is initiated after the splint is removed.
OUTCOMES
A survival rate greater than 80% is expected for replantation surgery.Functional outcomes are greatest for replantation of the thumb, proximal hand, and single digit distal to the FDS insertion (FIG 6A-D).5,6,13,16Recovery of sensation is correlated with function. As in other peripheral nerve injuries, age is the most important factor for recovery, with better results in younger patients. The average two-point discrimination inreplanted thumbs is 11 mm and in fingers is 8 mm.4 These values represent the average recovery for sharp amputation. Crush and avulsion mechanisms result in poorer two-point discrimination.Range of motion is related to level of amputation. Active PIP joint motion in replantations proximal to the FDS insertion average 35 degrees, whereas replantations distal to the FDS insertion result in 82 degrees of PIPjoint motion (FIG 6E-G).7
COMPLICATIONS
IMMEDIATE COMPLICATIONS




FIG 6 • A-D. This patient sustained an amputated thumb, which was successfully replanted with good cosmetic and functional results. E-G. Successful replantation of the ring and small fingers resulted in a functional hand capable of holding common objects. Vigilant reexamination of color, warmth, turgor, and capillary refill is necessary to decide whether exploration in the operating room is indicated. Revisions after 4 to 6 hours of reduced perfusionseldom result in digit salvage.7If venous engorgement occurs postoperatively, elevate the hand and remove constrictive dressings (including sutures that are too tight).Consideration for return to the operating room is based on intraoperative findings affecting the possibility of revising the venous anastomosis.If this is not possible, leeches or nail removal are used to alleviate venous congestion. These methods typically are used to bridge the first 4 to 6 days until adequate outflow is established.
LONG-TERM COMPLICATIONS
Long-term complications include pin tract infections, cold intolerance, stiffness, malunion, and nonunion.Pin tract infections usually occur more than 4 weeks after surgery. They are easily treated by pin removal and a course of oral antibiotics.Cold intolerance is almost universal. (This also is a problem in revision amputations.) Cold intolerance is expected to improve over the first 2 years, but it remains debatable whether it completely resolves.2,14 Digital stiffness is common because both the flexor and extensor tendons are repaired. Tenolysis should be delayed for at least 3 months postreplantation but has demonstrated good results.9Malunion usually results from malalignment at the time of bone fixation. Intraoperatively, rotational alignment is the most difficult to assess. Malunion is more common in proximal amputations because even slight malalignment at the amputation level is greatly accentuated at the fingertip.Nonunion is not common after replantation of the digit. It has been reported in fewer than 10% of digit replantations and rarely requires reoperation.15,16
REFERENCES
- Allen DM, Levin LS. Digital replantation including postoperative care. Tech Hand Up Extrem Surg 2002;6:171-177.
- Backman C, Nyström A, Backman C, et al. Arterial spasticity and cold intolerance in relation to time after digital replantation. J Hand Surg Br 1993;18:551-555.
- Camacho FJ, Wood MB. Polydigit replantation. Hand Clin 1992;8:409-412.P.1147
- Glickman LT, MacKinnon SE. Sensory recovery following digital replantation. Microsurgery 1990;11:236-242.
- Goldner RD, Howson MP, Nunley JA, et al. One hundred eleven thumb amputations: replantation versus revision. Microsurgery 1990;11:243-250.
- Goldner RD, Stevanovic MV, Nunley JA, et al. Digital replantation at the level of the distal interphalangeal joint and the distal phalanx. J Hand Surg Am 1989;14:214-220.
- Goldner RD, Urbaniak JR. Replantation. In: Green D, Hotchkiss RN, Pederson WC, et al, eds. Green's Operative Hand Surgery, ed 5. Philadelphia: Elsevier Churchill Livingstone, 2005:1569.
- Hattori Y, Doi K, Ikeda K, et al. A retrospective study of functional outcomes after successful replantation versus amputation closure for single fingertip amputations. J Hand Surg Am 2006;31:811-818.
- Jupiter JB, Pess GM, Bour CJ. Results of flexor tendon tenolysis after replantation in the hand. J Hand Surg Am 1989;14:35-44.
- Lucas GL. The pattern of venous drainage of the digits. J Hand Surg Am 1984;9:448-450.
- Matsuzaki H, Yoshizu T, Maki Y, et al. Functional and cosmetic results of fingertip replantation: anastomosing only the digital artery. Ann Plast Surg 2004;53:353-359.
- Ozkan O, Ozgentas HE, Safak T, et al. Unique superiority of microsurgical repair technique with its functional and aesthetic outcomes in ring avulsion injuries. J Plast Reconstr Aesthet Surg 2006;59:451-459.
- Patradul A, Ngarmukos C, Parkpian V. Major limb replantation: a Thai experience. Ann Acad Med Singapore 1995;24(4 suppl):82-88.
- Povlsen B, Nylander G, Nylander E. Cold-induced vasospasm after digital replantation does not improve with time: a 12-year prospective study. J Hand Surg Br 1995;20:237-239.
- Urbaniak JR, Hayes MG, Bright DS. Management of bone in digital replantation: free vascularized and composite bone grafts. Clin Orthop Relat Res 1978;(133):184-194.
- Urbaniak JR, Roth JH, Nunley JA, et al. The results of replantation after amputation of a single finger. J Bone Joint Surg Am 1985;67(4):611-619.
- Van Beek AL, Kutz JE, Zook EG. Importance of the ribbon sign, indicating unsuitability of the vessel, in replanting a finger. Plast Reconstr Surg 1978;61:32-35.
- Waikakul S, Sakkarnkosol S, Vanadurongwan V, et al. Results of 1018 digital replantations in 552 patients. Injury 2000;31:33-40.
- Wei FC, Chang YL, Chen HC, et al. Three successful digital replantations in a patient after 84, 86 and 94 hours of cold ischemia. Plast Reconstr Surg 1988;82:346-350.
