Introduction to PCL Bony Avulsions
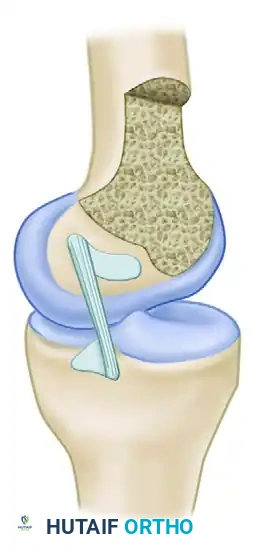
The posterior cruciate ligament (PCL) is the primary restraint to posterior tibial translation. While midsubstance tears are common in high-energy trauma, bony avulsions of the PCL—typically occurring at its tibial insertion—present a unique clinical entity. Unlike midsubstance ruptures, which often require complex ligamentous reconstruction, isolated bony avulsions are highly amenable to primary anatomical repair.
Surgical intervention is indicated to restore the native kinematics of the knee, prevent chronic posterior instability, and mitigate the long-term risk of secondary medial compartment and patellofemoral osteoarthritis. The surgical management of these injuries demands a profound understanding of posterior knee anatomy, meticulous surgical approaches, and rigorous protection of the popliteal neurovascular bundle.
Surgical Anatomy and Biomechanics of the PCL
A thorough comprehension of PCL anatomy is non-negotiable for the operating surgeon. The PCL is not a simple, uniform band; it is a complex continuum of fibers that dynamically stabilize the knee across its entire arc of motion.
Fiber Regions and Kinematics
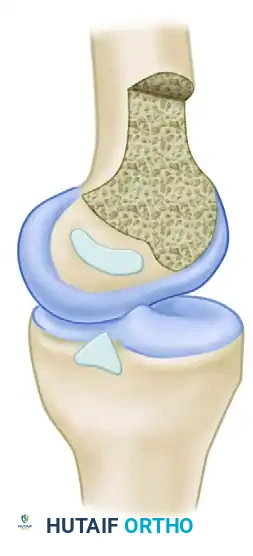
Traditionally, the PCL has been described as consisting of two primary functional bundles: the larger anterolateral (AL) bundle and the smaller posteromedial (PM) bundle. However, advanced macroscopic and functional anatomical studies characterize the ligament as a continuum of fibers without truly separate bands. Based on functional and morphological criteria, the PCL is subdivided into four distinct fiber regions according to their orientation, mechanical behavior during joint motion, and osseous insertion sites:
- Anterior Region: Constitutes the largest cross-sectional area. These fibers tighten progressively with knee flexion and relax during extension.
- Central Region: Acts as a transitional zone, providing stability through mid-flexion.
- Posterior Longitudinal Region: Runs vertically and contributes to extension stability.
- Posterior Oblique Region: Comprises approximately 5% to 15% of the ligament's mass. These fibers are lax in flexion but become taut in full extension.
Clinical Pearl: The amount of force generated in the PCL during a posterior drawer test depends heavily on the angle of flexion. Near 90 degrees of flexion, virtually all posterior force applied to the tibia is transmitted directly to the PCL, making this the optimal angle for clinical evaluation and intraoperative graft tensioning.
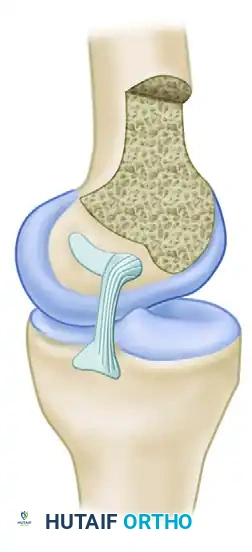
Femoral and Tibial Footprints
The PCL attachment site on the medial femoral condyle forms a broad semicircle with an average width of 32 mm. The tibial insertion site is located in a distinct depression (the fovea) approximately 1 cm below the posterior medial tibial articular surface.
The ligament is oriented vertically in the frontal plane and angles forward 30 to 45 degrees in the sagittal plane, depending on the degree of knee flexion. Biomechanical studies by Galloway et al. demonstrated that restoring knee stability in flexion depends heavily on the precise anatomical location of the femoral attachment. While true isometry is impossible to achieve due to the broad footprint, placing the graft within the native anatomical footprint most closely reproduces the intact knee's posterior limits.
Indications for Surgery
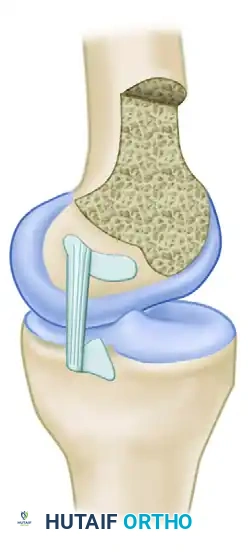
Acute Bony Avulsions
Primary repair is the gold standard for acute, displaced bony avulsions of the PCL from the tibia. Nonoperative management of displaced fragments inevitably leads to nonunion or malunion, resulting in chronic grade II or III posterior laxity.
Chronic Insufficiency and Reconstruction Criteria
For chronic PCL injuries, or those associated with multiligamentous trauma (e.g., knee dislocations), reconstruction is indicated.
* Grade III Posterior Drawer: More than 10 mm of posterior laxity is a strong relative indication for surgical reconstruction.
* Associated Instability: Torg et al. established a direct correlation between combined multidirectional instability and the rapid onset of patellar chondromalacia, meniscal derangement, and degenerative joint disease.
* Posterolateral Corner (PLC) Involvement: Harner et al. demonstrated biomechanically that PCL reconstruction is rendered ineffective and will likely fail due to overloading if associated posterolateral structures are not concurrently repaired or reconstructed.
Surgical Approaches for PCL Avulsion Repair
The choice of surgical approach depends on the size of the avulsed fragment, the presence of concomitant intra-articular pathology, and the surgeon's familiarity with posterior knee anatomy.
The Medial and Posteromedial Approach
If repair of an isolated PCL bony avulsion is the only anticipated procedure, a medial approach provides excellent utility.
- Incision: Begin a medial incision at a level 5 cm proximal to the superior pole of the patella. Proceed distally across the medial epicondylar area, paralleling the medial border of the patella and patellar tendon, and end at the level of the upper border of the pes anserinus.
- Superficial Dissection: Reflect the skin and subcutaneous tissue anteriorly to the medial border of the patella and posteriorly to the posteromedial corner.
- Joint Exploration: Make an anteromedial capsular incision to explore the joint and address any concurrent intra-articular pathology.
The Direct Posterior Approach
If the isolated PCL disruption is characterized by the avulsion of a large piece of bone from the posterior aspect of the tibia, a direct posterior approach is highly effective.
Surgical Warning: The direct posterior approach does not permit exploration of the anterior knee or correction of other intra-articular disorders. Therefore, the knee must be examined arthroscopically prior to positioning the patient prone to rule out and treat concurrent meniscal or chondral pathology.
With the direct posterior approach, detachment of the medial head of the gastrocnemius from the femoral condyle allows full, unhindered exposure of the posterior capsule and the posterior intercondylar notch.
Surgical Technique: Repair of Tibial Bony Avulsion (Technique 45-22)
Suture Pull-Through Fixation
If the PCL is avulsed from the tibia and the repair is to be performed through a medial approach, the following steps are executed:
- Exposure: Dissect the posterior skin and subcutaneous tissue as a single layer to the posteromedial corner. With the knee flexed to 90 degrees, retract the medial head of the gastrocnemius and the popliteal structures posteriorly to adequately expose the tibial attachment of the ligament.
- Capsulotomy: In the absence of major medial compartment disruption, a posteromedial capsular incision allows adequate exposure of the tibial attachment.
- Note: The most medial portion of an intact posterior horn of the medial meniscus may make exposure and suture placement difficult. However, excision of an intact medial meniscus is strictly contraindicated and unnecessary.
- Suture Placement: Place heavy, nonabsorbable sutures (e.g., #2 or #5 FiberWire) through the avulsed tibial attachment of the ligament using a locking Krackow or whipstitch configuration.
- Drilling Bone Tunnels: Drill parallel holes from the anteromedial aspect of the proximal tibia, aiming posteriorly to exit near the normal tibial attachment of the PCL. These holes should exit the posterior aspect of the tibia approximately 5 mm below the posterior articular margin. Commercial PCL drill guides are highly recommended to ensure precise trajectory.
- Protecting the Neurovascular Bundle: As the drill penetrates the posterior tibial cortex, it is imperative to protect the popliteal vessels. Place a wide metallic retractor (such as a malleable or Chandler retractor) between the posterior capsule and the neurovascular bundle.
- Fixation: Pass the sutures previously placed in the avulsed fragment through the parallel drill holes using suture passers. Tie them over a robust bridge of bone on the anteromedial tibia to reattach the ligament to its anatomical insertion and restore native tension.
- Closure: Use interrupted sutures to close both the anteromedial and posteromedial capsular incisions.
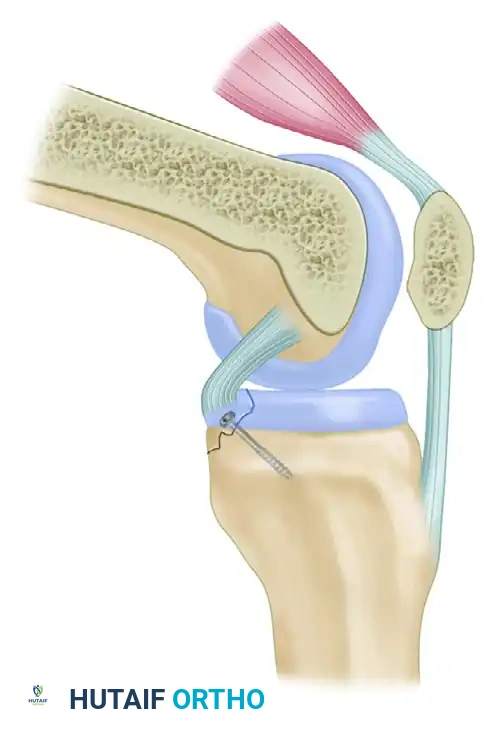
Screw Fixation for Large Fragments
When the avulsed bone fragment is large and structurally sound, rigid internal fixation with a screw provides superior biomechanical compression compared to sutures.
- Fit the fragment of bone carefully into its anatomical crater on the posterior tibia.
- Secure it with a partially threaded cancellous screw and washer. Ensure the screw trajectory is perpendicular to the fracture plane to maximize interfragmentary compression.
- Alternatively, suture anchors or a combination of pull-through sutures and screws can be utilized depending on bone quality.
- Repair the frequently associated tear of the posterior capsule with interrupted sutures.
Historical Perspectives on Postoperative Fixation
Historically, surgeons were highly concerned about the gravitational posterior sag of the tibia during the healing phase, which could stretch out the repaired PCL or graft. This led to the development of invasive transarticular fixation methods, which are now largely abandoned in modern practice.
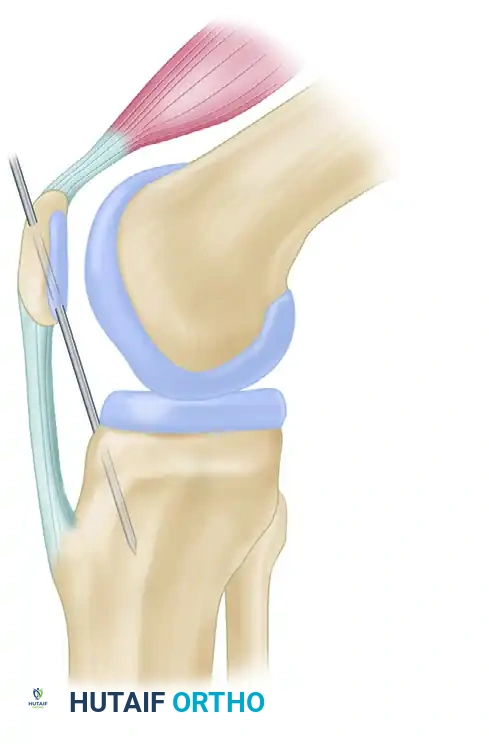
Transarticular Pinning
Before closure of the capsular incision, some historical texts advocated the insertion of a large Steinmann pin diagonally through the proximal tibia. The pin entered the joint in the intercondylar area and was driven into the femoral condyle while the tibia was held in an anteriorly reduced position. Advocates believed this prevented posterior sagging and protected the repair, even within a long-leg cast.
"Olecranization" of the Patella (Müller)
Müller and others advocated placing a 4.5-mm Steinmann pin through a predrilled hole in the patella and driving it into the tibia with the joint in appropriate alignment. This technique, termed "olecranization," aimed to rigidly link the extensor mechanism to the tibia to prevent posterior sag.

Evidence-Based Pitfall: Modern biomechanical studies have thoroughly debunked these practices. Weinstabl et al. investigated the influence of olecranization in vitro and demonstrated that it actually resulted in PCL strain five times greater than normal when the knee was in extension below 20 degrees or in flexion above 40 degrees.
Furthermore, an experimental study by Ogata et al. showed that no sagging of the tibia occurred at full extension in knees with an "isolated" sectioning of the PCL, provided the collateral ligaments were intact. Sagging only occurred as the knee was flexed.
Current Standard of Care: We do not use either of these invasive pinning techniques. The modern preference is to place the knee in a controlled motion brace locked in full extension, utilizing dynamic anterior tibial support braces if necessary.
Reconstruction of the Posterior Cruciate Ligament
When primary repair is impossible—such as in chronic insufficiency, midsubstance tears, or highly comminuted avulsions—PCL reconstruction is required.
Graft Selection
Numerous tissues have been advocated for PCL reconstruction. Historically, extra-articular procedures and intra-articular use of the medial gastrocnemius or lateral meniscus were attempted with poor long-term success.
- Autografts: Free bone-patellar tendon-bone (BTB) autografts produce highly predictable and satisfactory results for chronic PCL insufficiency. While semitendinosus and gracilis tendons are popular for ACL reconstruction, there is significant doubt regarding whether they possess adequate length and biomechanical strength to serve as a robust PCL replacement.
- Allografts: If the patient accepts allograft tissue, excellent results are obtained using a deep-frozen BTB graft (15 to 20 mm wide) or an Achilles tendon allograft with a bone block. These allografts provide the superior length and cross-sectional strength required to replicate the massive native PCL.
Tunnel Placement and Tensioning
The controversy regarding PCL reconstruction extends to tunnel placement. While the anatomy should be re-created to provide optimal stability, true isometry is impossible.
Most surgeons choose to place the femoral tunnel in the anterior portion of the femoral footprint. This replaces the bulky anterior fibers of the native PCL. Because these anterior fibers tighten in flexion, the graft must be tensioned and fixed with the knee near 90 degrees of flexion. Conversely, placing the tunnel too posteriorly creates a graft that is vertically oriented and fails to restrain posterior translation in functional flexion angles.
Postoperative Care and Rehabilitation
Postoperative rehabilitation following PCL avulsion repair or reconstruction must carefully balance the need to prevent stiffness with the imperative to protect the healing tissue from posterior tibial translation.
- Immobilization: The knee is immediately placed in a hinged knee brace locked in full extension. As demonstrated by Ogata et al., full extension utilizes the intact collateral ligaments to prevent posterior tibial sag.
- Weight-Bearing: Patients are typically restricted to touch-down weight-bearing (TDWB) with crutches for the first 4 to 6 weeks.
- Range of Motion (ROM): Passive prone ROM is initiated early to prevent arthrofibrosis. Prone positioning allows gravity to assist in anterior tibial translation, thereby offloading the PCL repair. Flexion is gradually advanced, typically limited to 90 degrees for the first 6 weeks.
- Strengthening: Quadriceps rehabilitation is the cornerstone of PCL recovery. The quadriceps act as a dynamic synergist to the PCL by drawing the tibia anteriorly. Isolated hamstring strengthening is strictly avoided for at least 3 to 4 months, as hamstring contraction directly exerts a posterior translation force on the tibia, stressing the repair.
By adhering to strict anatomical principles, ensuring robust fixation, and following a biologically sound rehabilitation protocol, surgeons can achieve excellent functional outcomes in the management of PCL bony avulsions.
