DEFINITION
Posttraumatic metacarpophalangeal (MCP) joint and proximal interphalangeal (PIP) contractures may develop directly as a result of injury to the joints and adjacent tissues or indirectly as a result of excessive immobilization or poor splinting of the hand. The circumstances precipitating the contracture determine the structures most involved: Joint capsule and collateral ligament contractureFlexor tendon adhesionsIntrinsic musculature contracture Extensor tendon adhesionsSkin and subcutaneous tissue scarringThe MCP joint generally becomes stiff in the extended position. Flexion contractures are uncommon and, when present, generally do not cause significant disability.The PIP joint often becomes contracted in the flexed position, although extension and combined contractures are not uncommon.The key to successfully mobilizing a stiff MCP or PIP joint is anticipating the pathologic causes before surgery.
ANATOMY
MCP joint osteology allows biaxial motion, including circumduction. The articular surface of the metacarpal head is asymmetric, with a relatively flat mediolateral convex arc (abduction-adduction) and a large anteroposterior convex arc (flexion-extension) that extends more volarly (FIG 1A).The MCP joint is enveloped by a relatively loose capsule inserting onto ridges surrounding the articular cartilage.Proper collateral ligaments originate from a dorsolateral tubercle on the metacarpal head and insert on the lateropalmar edge of the phalangeal base (FIG 1B).The volar plate of the MCP joint is an extension of the phalangeal articular surface. Unlike the volar plate of the PIP joint, the volar plate of the MCP joint is collapsible and there is little tendency to produce checkreins.This is one reason why MCP joint flexion contractures are much less common than those in the PIP joint.The flexor and extensor mechanisms surround the MCP joint.Volarly, the flexor sheath lies directly on the palmar plate and is thick, forming the first annular pulley. Dorsally, the extensor tendon gives rise to fibroaponeurotic sagittal bands that wrap around to insert on thepalmar plate. The tendons of the lumbricals and interossei join the dorsal expansion of the extensor. A slip of the dorsal interossei inserts on the dorsolateral aspect of the phalangeal base.The PIP joint is a simple ginglymus hinge joint stabilized by a boxlike arrangement of structures consisting of the proper and accessory collateral ligaments, the volar plate, and the dorsal capsule (FIG 1C,D).The joint is most stable in extension, and stability in flexion is provided by the volar plate, proper and accessory collateral ligaments, and flexor tendons, and less so by the dorsal structures.The collaterals provide radial and ulnar stability. They remain taut throughout the PIP joint range of motion.The accessory collaterals arise from the proximal phalanx and insert into the volar plate. Because there is no insertion of the accessory collateral into the middle phalanx, they will contract when the PIP joint is immobilized in flexion.The volar plate resists PIP hyperextension, and the dorsal capsule is relatively weak. Transverse retinacular ligaments connect the extensor and flexor tendon sheath.
PATHOGENESIS




FIG 1 • A. The articular surface of the metacarpal head protrudes volarly, making the capsule (and proper collateral ligaments) taut with flexion. B. MCP joint anatomy can be considered in two layers: the capsule and collateral ligaments, which lie immediately adjacent to the articular surfaces, and the flexor and extensor mechanisms, which envelop the joint. C. Normal anatomy of the PIP joint showing the arrangement of the collateral ligaments and the volar plate. D. Normal PIP anatomy showing the arrangement of the proper and accessory collateral ligaments. Curtis3,4 has reported that a contracture of the PIP joint can be due to the following:Contracture of the volar plate or the capsular structures Collateral ligament contractureScar contracture over the joint Volar skin contractureFlexor sheath contractureExtensor tendon contracture or adhesions Interosseous contracture or adhesionsA bony block or exostosisAdditional causes not pertinent to this chapter include fascia contracture, as in Dupuytren disease.Watson et al11 reported that a flexion contracture of the PIP joint is due to contracture of the checkreins on the proximal surface of the volar plate.
NATURAL HISTORY
Long-standing scarring and contracture of the MCP or PIP joint capsule almost invariably lead to adhesions to the adjacent flexor sheath and extensor mechanism.Residual joint kinetics are often altered with joint motion occurring through incongruous articular motions such as pivoting.Cartilage gradually atrophies and softens with disuse. Surface irregularities may develop.
PATIENT HISTORY AND PHYSICAL FINDINGS
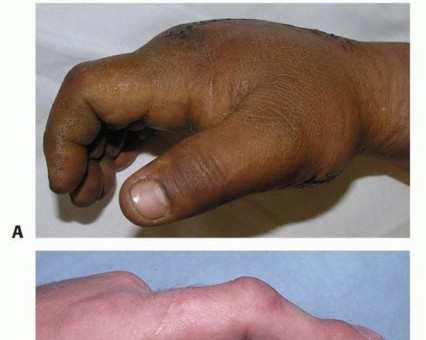
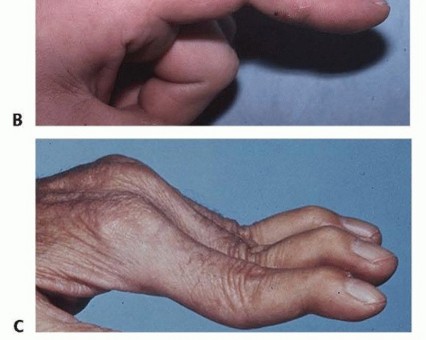
FIG 2 • A. Swollen hand. B. Boutonnière deformity. C. Swan-neck deformity. Concomitant PIP flexion and distal interphalangeal hyperextension mark a boutonnière deformity (FIG 2B), whereas hyperextension at the PIP joint is a sign of a swan-neck deformity (FIG 2C).
IMAGING AND OTHER DIAGNOSTIC STUDIES
Plain radiographs of the hand are made to evaluate for extrinsic and intrinsic causes of joint stiffness.ExtrinsicMetacarpal neck or shaft fracture: Extensor tendon adhesions at the fracture site may restrict MCP joint flexion (passive and active).Metacarpal fracture malunion: Shortening of the metacarpal results in extensor lag (average of 7 degreesfor every 2 mm of shortening according to Strauch and colleagues12). Apex dorsal metacarpal malunions create a corresponding extensor lag at the adjacent MCP joint.Proximal phalangeal fracture: Flexor and extensor tendon adhesions at the fracture site may limit active PIP (and sometime MCP) joint motion; passive motion may be maintained.Proximal phalangeal fracture malunion: Common apex volar proximal phalanx malunions can cause an apparent limitation of MCP joint flexion.IntrinsicIntra-articular fracture: Articular incongruity may serve as a bony restraint to joint motion.Arthritic changes: Cartilage softening and erosion often result in some degree of radiographically apparent arthritis.A “true” lateral radiograph of the involved joint must be closely examined for significant arthritic changes or any subluxation.There is little role for computed tomography (CT) scanning or magnetic resonance imaging (MRI) of the digits.
DIFFERENTIAL DIAGNOSIS
MCP extension contracture from extrinsic extensor muscle spasticity or intrinsic muscle paralysis or denervationMCP loss of flexion from proximal phalanx apex volar malunionPIP contracture from tendon imbalances, including boutonnière deformity and swan-neck deformity Skin contractureDupuytren disease
NONOPERATIVE MANAGEMENT
Nonoperative efforts to improve joint motion must be tried until motion has plateaued and the soft tissues are absolutely quiescent.As a general rule, inflammation and edema will subside and range of motion will improve for a minimum of 3 to 4 months after a traumatic or surgical insult to the hand.During this time, a supervised hand therapy program is essential.Most MCP contractures occur in extension. In addition to regular exercises, dynamic flexion splints (daytime) and static extension splints (nighttime) are useful.Most PIP contractures occur in flexion. Treatment begins with application of a nonelastic extension force across the PIP joint for an extended time. This can be done with serial finger casts or commercially available splints such as the Joint Jack (Joint Jack Co., Wethersfield, CT) or wire-foam splints. Once the contracture is corrected, elastic splints such as the Joint Spring or clock-spring splints can be used.Prosser10 presented one of the few studies to follow patients treated conservatively. Using a Capener splint to be worn for 8 to 12 hours per day over an 8-week period, there was an average improvement in the flexioncontracture from 39 to 21 degrees.10 There was no association between time in the splint with final extension or with final stiffness.PIP extension contractures are treated conservatively with serial static splints such as a joint-strap system.Curtis3,4 has reported that these joints do not require surgery if the joint can be passively flexed more than 75 degrees.The only study in the literature on the results of conservative treatment comes from Weeks et al.15 In a review of 212 patients with 415 stiff PIP joints, 87% responded favorably to nonoperative treatment. The average improvement in total active motion was 36 degrees.
SURGICAL MANAGEMENT
A capsulectomy is indicated only for a contracture not associated with articular incongruity or persistent subluxation of the joint.A stiff MCP or PIP joint in the face of articular incongruity or subluxation is best treated as an arthritic joint with a salvage type of surgery such as arthroplasty or arthrodesis.Mild to moderate joint wear is not a contraindication to capsulectomy, particularly in younger patients. Focal areas of articular cartilage irregularity and dorsal osteophytes may be débrided at the time of surgery.P.1200The literature does not give any specifics as to when to recommend surgery. We usually make this decision when a “functional arc of motion” has not been achieved after a minimum of 3 months of therapy.There is no absolute functional arc of motion for the MCP joint. In the absence of interphalangeal contractures, we have found that index, middle, ring, and small finger MCP flexion of 30, 35, 40, and 45 degrees, respectively, is generally satisfactory. When the interphalangeal joints have limited flexion, greater degrees of MCP flexion may be useful.Similarly, 45 degrees or more of total PIP motion is usually satisfactory. Flexion contractures greater than 45 degrees are poorly tolerated and may benefit from surgical release.Extreme flexion contractures (>60 or 70 degrees) may be best managed with arthrodesis. The results of a capsulectomy are often disappointing.Extension contractures are better tolerated, especially if there is flexion to at least 75 degrees.When a patient has exhausted nonoperative management options and joint stiffness exceeds the preceding guidelines, surgery for contracture release is considered.
PREOPERATIVE PLANNING


FIG 3 • A. A combined MCP extension contracture and PIP flexion contracture of the index finger is approached by extending the dorsal incision distally in the midaxial line. B. Excellent exposure of the finger extensor mechanism is coupled with visualization of the volar aspect of the PIP joint.
POSITIONING
Patients are positioned supine with the affected extremity on a hand table. A brachial tourniquet is applied that allows access to the forearm should a full-thickness skin graft be necessary.
APPROACH
The approach for MCP contracture depends on three factors:The number of involved MCP joints The need to operate on the PIP joint The quality of the dorsal soft tissuesA single MCP joint is approached with a dorsal longitudinal incision. If the PIP joint has an extension contracture, the incision is carried over the PIP in the midline. If the PIP has a flexion contracture, the incision may be extended distally in the midaxial line (FIG 3A).Multiple MCP joint extension contractures are approached using separate dorsal longitudinal incisions.This is the most extensile method and facilitates management of associated extensor tendon adhesions and PIP contractures (FIG 3B).Two adjacent MCP joints may also be approached by making a dorsal longitudinal incision centered in the web between affected rays.If necessary, it is safe to extend this incision as a Y onto each digit to complete a tenolysis or operate on the PIP joints.Multiple MCP joints may be also approached by making a single transverse incision lying just proximal to the metacarpal heads.This approach is preferred only when the dorsal soft tissues are fibrotic and noncompliant. In this situation, the surgeon should plan for skin graft or flap coverage of the anticipated defect.The surgical approach forisolatedPIP joint contractures varies with the procedure used.A capsulectomy for a flexion contracture is performed through a lateral approach, a checkrein releasethrough a volar approach, and percutaneous release laterally.A dorsal skin incision could be used with a capsulectomy for an extension contracture or when there is a previous dorsal incision or specific hardware to remove.External fixation requires no incision.P.1201
TECHNIQUE
Metacarpophalangeal Joint Contractures
METACARPOPHALANGEAL JOINT CONTRACTURES
DORSAL CAPSULECTOMY OF THE JOINT
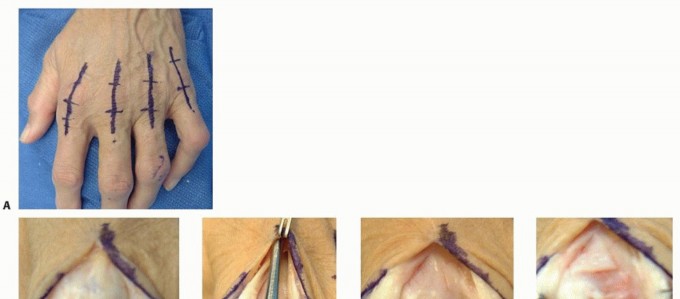
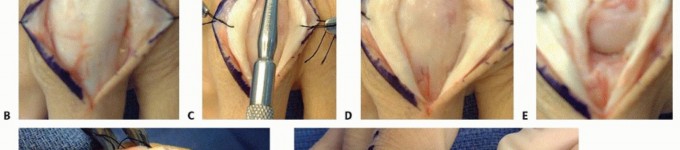
TECH FIG 1 • A. Separate dorsal longitudinal incisions are planned for multiple MCP joint extension contractures. B. Full-thickness soft tissue flaps are raised at the level of the extensor mechanism. C. The extensor mechanism is split longitudinally. D. Each side of the extensor tendon is freed of adhesions to the adjacent tissues. E. The dorsal capsule is excised. F. The proper collateral ligaments are released from the metacarpal head. G. MCP flexion is reassessed.






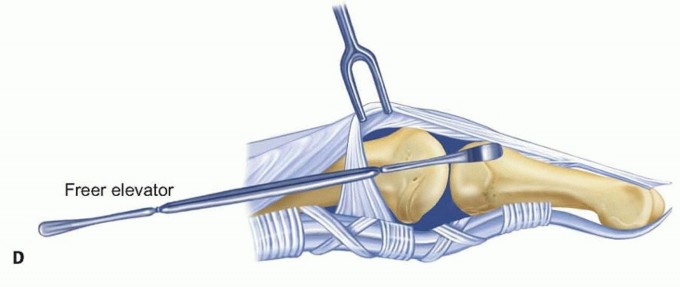
TECH FIG 3 • A. Release of MCP extension contractures in the severely burned hand is accomplished through a transverse skin incision and extensor tenotomy.(continued) If bleeding from scar is excessive, then use a small rubber vascular loop or a quarter-inch Penrose drain to stent open the wound to allow drainage for the first 24 hours.A dorsal splint is applied to maintain the MCP joints in 70 degrees of flexion. Limited Dorsal Capsulotomy of the Metacarpophalangeal Joint In mild contractures, a dorsal capsulectomy may not be necessary. Bode and Gottlieb1 have described a limited capsulotomy.Expose the extensor mechanism as described earlier (see TECH FIG 1).Use a Freer elevator to release the extensor mechanism and sagittal bands from the dorsal capsule (TECH FIG 2A).Retract the dorsal capsule distally.Incise the capsule transversely at the distal dorsal aspect of the metacarpal head (TECH FIG 2B).The incision extends from one collateral recess to the other.Using a Beaver blade or Freer elevator directed to the periphery of the capsulotomy, perform a stepwise release of the collateral ligaments off the metacarpal head (TECH FIG 2C). Extensor Tenotomy of the Metacarpophalangeal Joint


TECH FIG 3 •(continued)B. The MCP joints are maintained in flexion with Kirschner wires. C. The dorsal soft tissue defect is covered with a pedicled tensor fascia lata flap. Make a tenotomy at the distal margin of the sagittal bands. Capsulectomy and collateral ligament release follow as described earlier.At closure, sew the proximal tendon to the sagittal bands; close the extensor hood on itself in the midline dorsally.Given the chronicity of these contractures, consider temporary Kirschner wire fixation of the MCP joints in flexion (TECH FIG 3B).Kirschner wire fixation is especially useful for protection of skin grafts or flaps when the dorsal soft tissues are deficient (TECH FIG 3C).1. Proximal Interphalangeal Joint Contracture Capsulectomy for Proximal Interphalangeal Joint Flexion Contracture



TECH FIG 4 • A. Skin incision. B. The transverse retinacular ligament is protected and the collateral ligament is exposed for excision. C. The collateral ligaments are excised.(continued)
TECH FIG 4 •(continued)D. Extensor tenolysis is done if required.
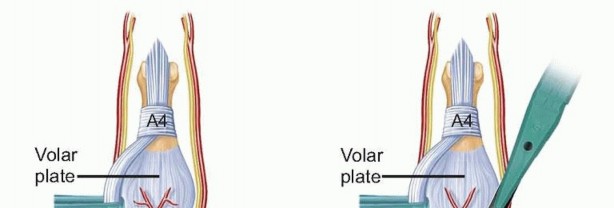


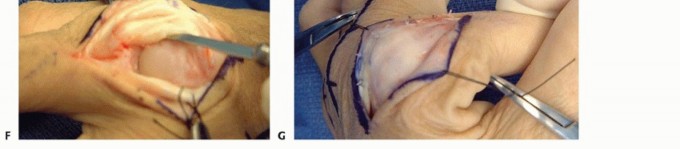
TECH FIG 5 • A. The flexor sheath is exposed and the checkrein ligament on the proximal edge of the volar plate is exposed. B. Watson's technique for release of the checkrein ligaments to correct a PIP flexion contracture. Checkrein Ligament Release for Proximal Interphalangeal Flexion Contracture According to Watson et al,14 the volar plate does not flex but rather slides proximally and distally with flexion and extension. PIP joint adhesions causing contracture occur proximal to the volar plate and involve the checkrein ligaments.Excision of the volar plate or division of the collateral ligaments is rarely required to achieve full extension.The joint is approached volarly, often with a V-Y incision to address palmar skin contracture. Open the theca between the A2 and A4 pulleys and retract the flexor tendons (TECH FIG 5A). Release the checkrein ligaments, preserving the nutrient vessel (TECH FIG 5B).If there is still a contracture after release of the checkreins, release the dorsal portion of the collaterals or the oblique retinacular ligament of Landsmeer.This technique is helpful if a palmar exposure is required for excision of Dupuytren disease or during flexor tendon reconstruction. Percutaneous Collateral Ligament Release for Proximal Interphalangeal Flexion Contracture


TECH FIG 6 • A. Cross-section shows placement of the no. 69 Beaver blade parallel to the proximal phalanx and adjacent to the PIP collateral ligament origin. B. Sagittal view demonstrates the technique of “sweeping” the Beaver blade and detaching the collateral ligament from its origin. Place a no. 69 Beaver blade percutaneously adjacent to the proximal phalangeal head (TECH FIG 6A). Disinsert the proper collateral ligaments with a sweeping-type motion (TECH FIG 6B).Gently manipulate the finger into extension. Use of an External Fixator for Proximal Interphalangeal Flexion Contracture


TECH FIG 7 • Application of the Digit Widget for PIP flexion contractures. An external frame is applied without any soft tissue release.Houshian et al8 distracts a one-fourth turn (¼ mm) each day until 5-mm distraction of the joint is achieved.The frame is left in place for 4 to 6 weeks. Houshian leaves the frame in place for one week after distraction is stopped. Capsulectomy for Proximal Interphalangeal Joint Extension Contracture
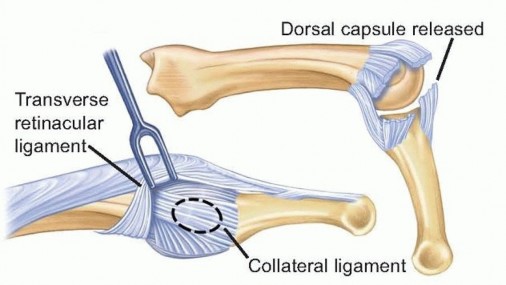
TECH FIG 8 • Through a dorsal incision, the transverse retinacular ligament is protected and the collateral ligament is excised. The dorsal capsule is also released. P.1206Persistent stiffness1. Failure to recognize intrinsic contracture, inadequate skinenvelope, and flexor sheath contracture2. Unrecognized reflex sympathetic dystrophyPostoperative instability1. Failure to preserve transverse retinacular fibers orexcessive release of the soft tissuesPreoperative flexion contracturemore than 75 degrees1. Consider an arthrodesis rather than soft tissue release.Best patients for a release1. Younger patient, without a crush injury, reflex sympatheticdystrophy, or revascularization2. Preoperative flexion contracture of less than 43 degrees
PEARLS AND PITFALLS
MCP JOINT
Indications ▪ The patient must have participated in a well-supervised rehabilitation protocoland be committed to another 8-12 weeks of therapy.Approach ▪ A transverse skin incision is more likely to restrict flexion and more prone to breakdown in the postoperative period; however, a transverse skin incision facilitates soft tissue coverage of multiple MCP joints when operative release of the severely crushed or burned hand is undertaken.Capsulectomy and collateral release1. Adhesions between the volar plate and condyles may be responsible for limited flexion after release of the proper collateral ligaments.2. Accessory collateral ligament release may be necessary to achieve full extension without catching.Associated pathology1. Intraoperative attempts at active flexion by the patient will identify associated flexor tendon adhesions in a surprisingly large number of patients.2. Flexor tenolysis may be made by extending the dorsal incision in the midaxial line or by making a separate Brunner-type volar approach.
PIP JOINT
POSTOPERATIVE CARE

FIG 4 • Dynamic flexion splinting is instituted after surgery for correction of MCP joint extension contracture. Patients are reassessed 2 to 3 weeks after surgery. If there is a significant extensor lag (as may follow an extensive extensor tenolysis), a dynamic extension splint can be alternated with the dynamic flexion splint during the day.Nighttime static splinting is continued for a minimum of 6 to 8 weeks. Therapy is usually continued for about 3 months.PIP release often benefits from early dynamic splinting during the day and passive splinting at night.
OUTCOMES
Final motion is often much less than that obtained at surgery but often makes a substantial difference in hand function.Motion plateaus 3 to 6 months after surgery.Results are best when the joint can be mobilized with capsulectomy alone. Each additional procedure, such asP.1207tenolysis, increases postoperative swelling and scar formation, limiting long-term gains.4In some cases, an improvement in MCP or PIP joint motion of 30 to 45 degrees is a reasonable expectation.2,16According to Gould and Nicholson,7 improvement in MCP and PIP motion depends on the cause of the contracture. In a study of 105 MCP capsulectomies and 112 PIP capsulectomies, patients with direct joint trauma (fractures or crush injuries) gained an average of about 20 degrees of active motion, slightly more for the MCP and less for the PIP. Patients with indirect causes of capsular contracture (nerve injury,stroke, or skin burns) did better.7Ghidella et al6 reported on the results of 68 PIP capsulectomies. The average overall improvement was adisappointing 7 degrees.6 The best results occurred in young patients without a history of crush injury, pain syndrome, or revascularization. The average improvement measured 17 degrees in this group compared with 0 degree when there was a “complex diagnosis.”Houshian et al8 reported a mean improvement of 67 degrees in 94 patients. Better results were observedin patients younger than 40 years old.8 Only 12 superficial infections were observed without major complications. There are no reported results using the Digit Widget. Unfortunately, the authors have not been able to reproduce Houshian's results.
COMPLICATIONS
Wound dehiscence and infection Persistent or recurrent contracture Extensor ruptureUlnar deviation of the finger at the MCP joint Postoperative subluxation or dislocation Injury to the dorsal branch of the digital nerve
REFERENCES
- Bode L, Gottlieb M. Dorsal capsulectomy of the metacarpophalangeal joint. In: Blair WF, ed. Techniques in Hand Surgery. Baltimore: Williams & Wilkins, 1996:923-929.
- Buch VI. Clinical and functional assessment of the hand after metacarpophalangeal capsulotomy. Plast Reconstr Surg 1974;53:452-457.
- Curtis R. Stiff finger joints. In: Grabb W, Smith J, eds. Plastic Surgery. Boston: Little, Brown, 1979:598-603.
- Curtis RM. Capsulectomy of the interphalangeal joints of the fingers. J Bone Joint Surg Am 1954;36-A(6):1219-1232.
- Favre Y, Kinnen L. Resection of the flexor digitorum superficialis for trigger finger with proximal interphalangeal joint positional contracture. J Hand Surg Am 2012;37:2269-2272.
- Ghidella SD, Segalman KA, Murphey MS. Long-term results of surgical management of proximal interphalangeal joint contracture. J Hand Surg Am 2002;27(5):799-805.
- Gould JS, Nicholson BG. Capsulectomy of the metacarpophalangeal and proximal interphalangeal joints. J Hand Surg Am 1979;4:482-486.
- Houshian S, Jing SS, Kazemian GH, et al. Distraction for proximal interphalangeal joint contractures: longterm results. J Hand Surg Am 2013;38:1951-1956.
- Kasabian A, McCarthy J, Karp N. Use of a multiplanar distracter for the correction of a proximal interphalangeal joint contracture. Ann Plast Surg 1998;40:378-381.
- Prosser R. Splinting in the management of proximal interphalangeal joint flexion contracture. J Hand Ther 1996;9:378-386.
- Stanley JK, Jones WA, Lynch MC. Percutaneous accessory collateral ligament release in the treatment of proximal interphalangeal joint flexion contracture. J Hand Surg Br 1986;11:360-363.
- Strauch RJ, Rosenwasser MP, Lunt JG. Metacarpal shaft fractures: the effect of shortening on the extensor tendon mechanism. J Hand Surg Am 1998;23:519-523.
- Tsuge K. Contractures. In: Tsuge K, ed. Comprehensive Atlas of Hand Surgery. Chicago: Year Book Medical Publishers, 1989:239-241.
- Watson HK, Light TR, Johnson TR. Checkrein resection for flexion contracture of the middle joint. J Hand Surg Am 1979;4:67-71.
- Weeks PM, Wray RC Jr, Kuxhaus M. The results of non-operative management of stiff joints in the hand. Plast Reconstr Surg 1978;61:58-63.
- Young VL, Wray RC Jr, Weeks PM. The surgical management of stiff joints in the hand. Plast Reconstr Surg 1978;62:835-841.
