INTRODUCTION TO POSTERIOR HIP DISLOCATIONS
The hip is a highly constrained, intrinsically stable ball-and-socket joint. Dislocation requires significant high-energy trauma, most commonly seen in motor vehicle collisions (the classic "dashboard injury") or falls from a significant height. Posterior hip dislocations account for approximately 90% of all hip dislocations.
Because the medial circumflex femoral artery provides the primary blood supply to the femoral head, a posterior dislocation places these critical vessels under extreme tension or causes direct tearing. Consequently, posterior hip dislocation is an absolute orthopedic emergency.
Clinical Pearl: The risk of avascular necrosis (AVN) of the femoral head increases exponentially if the hip remains dislocated for more than 6 hours. Immediate closed reduction is the standard of care and must be prioritized during the initial trauma resuscitation.
CLINICAL PRESENTATION AND PRE-REDUCTION IMAGING
Characteristic Extremity Posture
Patients with a pure posterior hip dislocation present with a highly characteristic lower extremity posture. Because the femoral head is displaced posterior and superior to the acetabulum, the limb is typically shortened, adducted, and internally rotated. The hip is usually held in a flexed position.

FIGURE 55-52 A: Characteristic extremity posture of a posterior hip dislocation demonstrating flexion, adduction, and internal rotation.

FIGURE 55-52 B: Anterior view of the characteristic extremity posture.
Neurological Evaluation
Before any reduction attempt, a meticulous neurological examination is mandatory. The sciatic nerve lies directly posterior to the hip joint and is at high risk of compression or traction injury. Approximately 10% to 20% of posterior dislocations are associated with a sciatic nerve palsy, most commonly affecting the common peroneal division (resulting in foot drop and decreased sensation in the first web space).
Pre-Reduction Radiographic Assessment
Standard Advanced Trauma Life Support (ATLS) protocols dictate an anteroposterior (AP) radiograph of the pelvis. This single view is usually sufficient to diagnose a posterior dislocation and identify gross concomitant fractures of the femoral head, neck, or acetabulum.
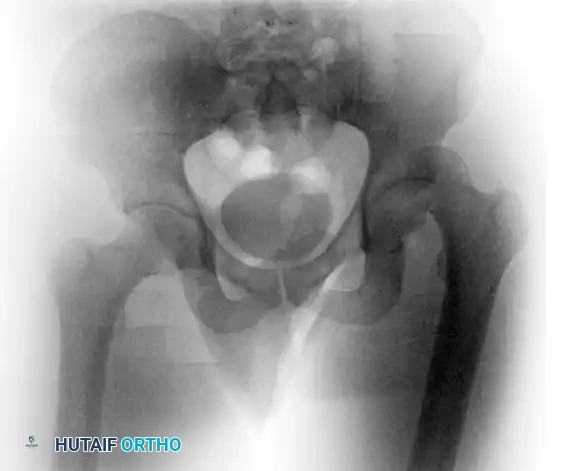
FIGURE 55-52 C: Preoperative AP radiograph demonstrating a posterior hip dislocation with a concomitant femoral head fracture.
If the patient is hemodynamically stable and already in the CT scanner for a trauma pan-scan, pre-reduction axial and coronal CT images can provide invaluable information regarding intra-articular fragments and acetabular wall integrity.

FIGURE 55-52 D: Preoperative axial CT scan detailing the posterior displacement.
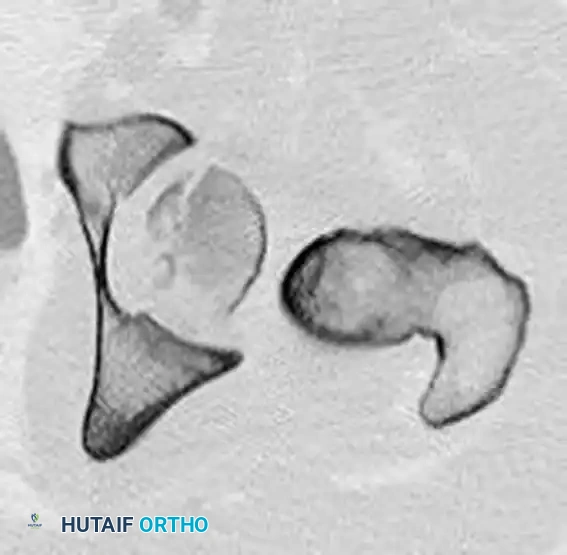
FIGURE 55-52 E: Additional preoperative axial CT scan highlighting the femoral head fracture.

FIGURE 55-52 F: Preoperative coronal CT scan showing the superior migration of the femoral head.

FIGURE 55-52 G: Anteroposterior pelvic radiograph showing eventual union after appropriate management.
PREREQUISITES FOR CLOSED REDUCTION
Attempting to reduce a dislocated hip against spastic, powerful pelvic and thigh musculature is a recipe for iatrogenic femoral neck fracture or chondral damage.
- Adequate Sedation/Anesthesia: Deep conscious sedation (e.g., Propofol and Ketamine) or general anesthesia with complete muscle relaxation is required.
- Pelvic Stabilization: A dedicated assistant must firmly stabilize the pelvis to the stretcher. Without counter-traction, the entire patient will simply be pulled off the bed.
- Floor Clearance: Ensure the stretcher is locked and the floor is clear of slipping hazards, as the surgeon will need to apply significant force.
REDUCTION MANEUVERS FOR POSTERIOR HIP DISLOCATION
Many closed reduction maneuvers have been described in the orthopedic literature. The choice of maneuver depends on the surgeon's preference, the number of available assistants, and the patient's concomitant injuries.
1. The East Baltimore Lift
The East Baltimore lift is highly convenient for the surgeon, ergonomically superior, and extremely effective. It utilizes the strength of the surgeon's legs rather than the upper body, minimizing fatigue during difficult reductions.
Step-by-Step Technique:
* Positioning: The patient remains supine. The surgeon stands on the side of the affected extremity, facing an assistant who stands on the opposite side of the limb.
* Limb Position: The patient’s hip and knee are flexed to 90 degrees.
* Arm Placement: The surgeon’s more cephalad arm is passed beneath the patient’s proximal calf and placed firmly on the assistant’s shoulder. The assistant reciprocates by placing his or her hand on the surgeon’s shoulder for stability.
* Ankle Control: The surgeon’s more caudad arm is used to control the patient’s ankle, allowing for subtle internal or external rotation of the extremity as necessary.
* Pelvic Stabilization: A second assistant places their hands firmly on the patient's anterior superior iliac spines (ASIS) to stabilize the pelvis.
* The Reduction: The surgeon and the first assistant simultaneously stand up (extending at their own hips and knees). This generates a powerful, controlled, anterior-directed force to lift the femoral head over the posterior acetabular rim and reduce the dislocation.
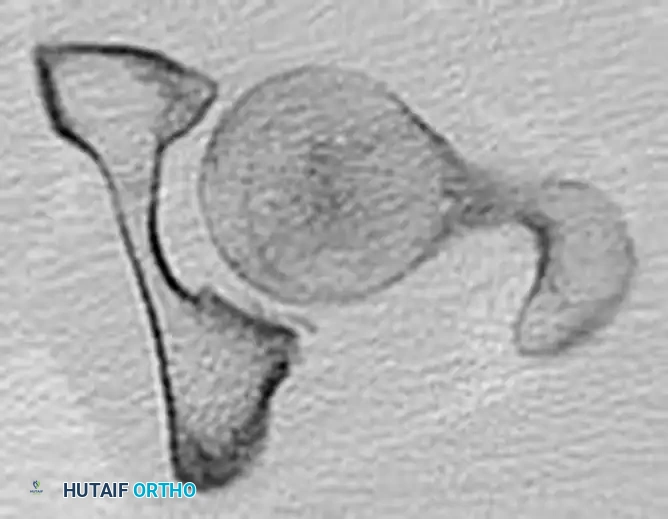
FIGURE 55-56 A: East Baltimore lift setup. Surgeon and assistant link arms beneath the patient's calf.

FIGURE 55-56 B: Execution of the East Baltimore lift, applying anterior-directed force by standing.
2. The Allis Maneuver
The Allis maneuver is the most universally taught technique and can be performed with one less assistant than the East Baltimore lift. It relies on direct, in-line traction.
Step-by-Step Technique:
* Positioning: The patient is positioned supine.
* Pelvic Stabilization: An assistant firmly stabilizes the pelvis by pressing down on the ASIS.
* Initial Traction: The surgeon applies traction in the direction opposite the deformity (in-line with the femur).
* Flexion: While continuous traction is being applied, the hip is slowly flexed to 90 degrees. This relaxes the Y-ligament of Bigelow.
* Reduction: The surgeon applies a strong anterior lifting force. The extremity is gently internally and externally rotated as necessary to clear the posterior acetabular wall and achieve reduction. A palpable and audible "clunk" typically signifies successful reduction.
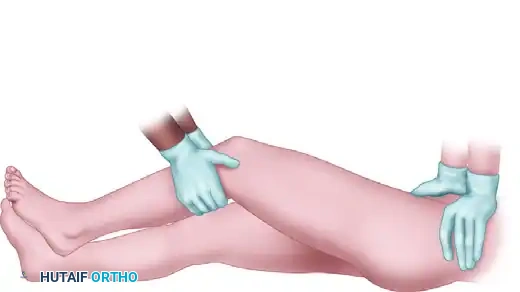
FIGURE 55-57 A: Allis maneuver setup with the assistant stabilizing the pelvis.

FIGURE 55-57 B: Application of in-line traction while flexing the hip.
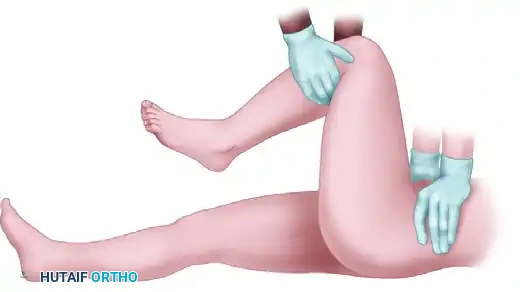
FIGURE 55-57 C: Anterior lifting force applied at 90 degrees of hip flexion.
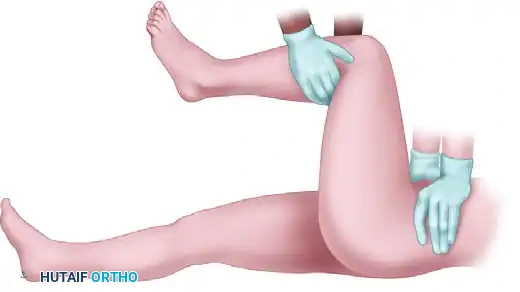
FIGURE 55-57 D: Gentle rotation to guide the femoral head into the acetabulum.
3. The Bigelow Maneuver
The Bigelow maneuver requires the same number of individuals as the Allis maneuver but utilizes a levering technique rather than pure traction.
Surgical Warning: The Bigelow maneuver carries a higher risk of iatrogenic femoral neck fracture if performed forcefully against resistance. It must be executed with finesse, not brute strength.
Step-by-Step Technique:
* Positioning: The patient is positioned supine, and an assistant stabilizes the pelvis.
* Grip: The surgeon places one arm beneath the patient’s proximal calf and grasps the ankle with his or her other arm.
* Traction and Flexion: The surgeon applies traction in the direction opposite the deformity and then flexes the hip to 90 degrees.
* Positioning the Head: Traction is maintained at 90 degrees of flexion, keeping the extremity adducted and internally rotated.
* The Levering Motion: The femoral head is then levered into the acetabulum with a smooth, continuous combination of abduction, external rotation, and extension of the hip (a circumduction motion).
4. The Stimson Maneuver
The Stimson maneuver utilizes gravity to assist with the reduction. However, it is often impractical in the acute trauma setting.
Step-by-Step Technique:
* Positioning: The patient must be placed prone with the affected extremity hanging off the end of the stretcher.
* Execution: The surgeon applies downward pressure on the proximal calf (anterior force relative to the femur) while the hip is flexed at 90 degrees over the edge of the bed.
* Drawbacks: Turning a polytrauma patient prone is frequently contraindicated due to spine, chest, or abdominal injuries, making this maneuver less practical.
POST-REDUCTION EVALUATION AND IMAGING
Following a palpable reduction, the limb should rest comfortably in a neutral position. The neurological exam must be immediately repeated and documented.
Radiographic Confirmation
An AP pelvis radiograph is obtained immediately to confirm concentric reduction. However, plain radiographs are notoriously insensitive for detecting small intra-articular osteochondral fragments or subtle joint incongruity.

FIGURE 55-54 A: Pre-reduction radiograph of a posterior dislocation.
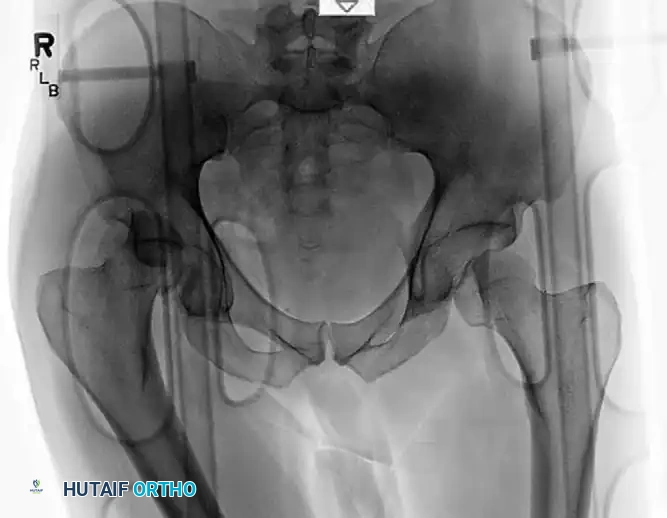
FIGURE 55-54 B: Radiograph after closed reduction. The joint space appears slightly widened.
The Mandatory Post-Reduction CT Scan
If reduction is achieved, a post-reduction CT scan with fine cuts (1-2 mm) is absolutely mandatory. The CT scan evaluates for:
1. Concentric Reduction: Ensuring the femoral head is perfectly seated.
2. Incarcerated Fragments: Identifying bone or cartilage fragments trapped in the joint space, which will rapidly destroy the articular cartilage if left in situ.
3. Acetabular Wall Fractures: Assessing the size and displacement of posterior wall fractures to determine if surgical fixation is required for stability.

FIGURE 55-54 C: Axial CT scan after reduction clearly showing an incarcerated intra-articular fragment preventing concentric reduction.

FIGURE 55-54 D: Coronal CT scan confirming the incongruous joint space.
Even when plain radiographs appear acceptable, subtle incongruity can only be ruled out via CT.

FIGURE 55-55 A: Subtle incongruity on a plain radiograph that is easily missed.

FIGURE 55-55 B: The same patient's CT scan revealing a significant intra-articular fragment requiring surgical excision.
MANAGEMENT OF IRREDUCIBLE DISLOCATIONS
If reduction cannot be obtained by closed methods with adequate sedation in the emergency department, an immediate CT scan is ordered to determine the presence of any bony block to reduction (e.g., a large incarcerated posterior wall fragment or a buttonholed capsule).
One additional closed reduction attempt can be made in the operating room with the patient under general anesthesia and complete chemical paralysis. If this fails, the surgeon must proceed immediately with an open reduction, typically via a Kocher-Langenbeck posterior approach.
COMPLEX SCENARIOS: CONCOMITANT PROXIMAL FEMORAL FRACTURES
High-energy trauma resulting in posterior hip dislocation can occasionally cause concomitant fractures of the proximal femur, including femoral head fractures (Pipkin classifications) or subtrochanteric fractures.
When a subtrochanteric fracture occurs in conjunction with a hip dislocation, closed reduction of the hip is often impossible because the proximal femur cannot be manipulated via the distal shaft. These complex fracture-dislocations require open reduction and rigid internal fixation.
Fixation with a Proximal Femoral Locking Plate
For subtrochanteric fractures associated with complex hip trauma, a proximal femoral locking plate provides excellent biomechanical stability.
Surgical Technique Overview:
1. Approach: The plate is introduced through a proximal lateral wound.
2. Positioning: It is advanced distally to a level that allows the placement of a guide pin just proximal to the calcar and perfectly centered in the femoral head on the lateral fluoroscopic view.
3. Temporary Fixation: The plate is pinned in place proximally and distally once placement has been optimized.
4. Locking Construct: A locking screw is placed just proximal to the calcar to secure the proximal segment, followed by distal shaft fixation.
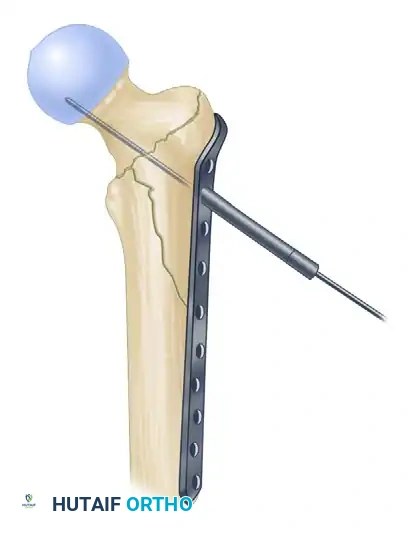
FIGURE 55-51 A: Plate is introduced through the proximal wound and advanced distally.
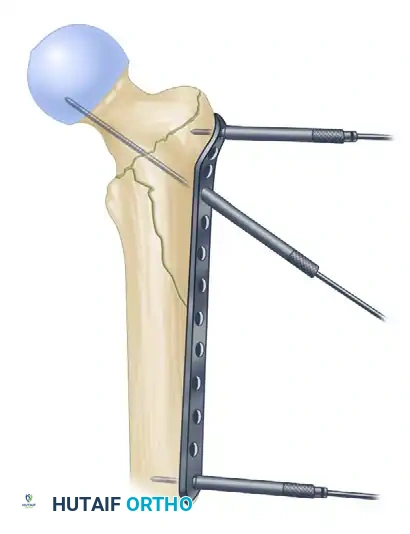
FIGURE 55-51 B: Plate is pinned in place proximally and distally once placement has been optimized.

FIGURE 55-51 C: Locking screw is placed just proximal to the calcar.

📚 Medical References
- posterior hip dislocations in the lateral position using traction-countertraction: safer for the surgeon? J Orthop Trauma 13:373, 1999.
- DeLee JC, Evans JA, Thomas J: Anterior dislocation of the hip and associated femoral-head fractures, J Bone Joint Surg 62A:960, 1980.
- Dreinhöfer KE, Schwarzkopf SR, Haas NP, et al: Isolated traumatic dislocation of the hip: long-term results in 50 patients, J Bone Joint Surg 76B:6, 1994.
- Epstein HC: Traumatic anterior and simple posterior dislocations of the hip in adults and children, Instr Course Lect 22:115, 1973.
- Epstein HC: Traumatic dislocations of the hip, Clin Orthop Relat Res 92:116, 1973.
- Epstein HC: Posterior fracture-dislocations of the hip, J Bone Joint Surg 56A:1103, 1974.
- Goddard NJ: Classifi cation of traumatic hip dislocation, Clin Orthop Relat Res 377:11, 2000.
- Gregory CF: Fractures and dislocations of the hip and fractures of the acetabulum: early complications of dislocation and fracture-dislocations of the hip joint, Instr Course Lect 22:105, 1973.
- Hougaard K, Lindequist S, Nielsen LB: Computerized tomography after posterior dislocation of the hip, J Bone Joint Surg 69B:556, 1987.
- Hougaard K, Thomsen PB: Traumatic posterior dislocation of the hip—prognostic factors infl uencing the incidence of
