INTRODUCTION TO HIP JOINT INSTABILITY AND DISLOCATION
Hip dislocations represent true orthopedic emergencies that demand immediate recognition, precise radiographic evaluation, and urgent reduction. The native hip joint is inherently stable due to its deep acetabular socket, robust labral complex, and formidable ligamentous restraints (iliofemoral, ischiofemoral, and pubofemoral ligaments). Consequently, a dislocation requires high-energy trauma, frequently resulting in concomitant injuries to the acetabulum, femoral head, or adjacent neurovascular structures.
The overarching goal of immediate reduction is the preservation of the femoral head's tenuous blood supply—primarily derived from the medial circumflex femoral artery (MCFA)—to mitigate the devastating complication of avascular necrosis (AVN) or osteonecrosis. This comprehensive guide delineates the biomechanics, closed reduction maneuvers, and advanced surgical interventions required for both pure hip dislocations and complex fracture-dislocations, including those classified under the Pipkin system.
REDUCTION MANEUVERS FOR ANTERIOR HIP DISLOCATION
Anterior hip dislocations account for approximately 10% to 15% of all traumatic hip dislocations. They are typically classified into superior (pubic or iliac) and inferior (obturator) subtypes, dictated by the degree of hip flexion at the exact moment of impact.
Biomechanics and Clinical Presentation
Anterior dislocations generally occur when the hip is subjected to a forceful abduction and external rotation moment.
* Inferior (Obturator) Dislocation: Occurs with simultaneous hip flexion, abduction, and external rotation. The patient presents with the affected limb fixed in flexion, abduction, and external rotation.
* Superior (Pubic) Dislocation: Occurs with the hip extended, abducted, and externally rotated. The limb presents in extension, slight abduction, and external rotation.
Closed Reduction Technique
The primary objective of closed reduction is to unlock the femoral head from the anterior acetabular rim or obturator foramen without causing iatrogenic fracture to the femoral neck or further damaging the articular cartilage.
Anterior hip dislocations typically can be reduced utilizing a combination of:
1. Longitudinal Traction: Applied in the line of the deformity to distract the femoral head from the pelvis.
2. Laterally Directed Force: An assistant applies a lateral force to the proximal thigh to help clear the femoral head past the anterior acetabular rim.
3. Internal Rotation: Often required to complete the reduction, guiding the head back into the acetabular fossa.
⚠️ Surgical Warning: Failed Closed Reduction
Repeated, forceful attempts at closed reduction are contraindicated. If closed reduction fails after two well-executed attempts under adequate sedation or general anesthesia, the surgeon must proceed to open reduction. The Smith-Petersen (anterior) approach is the gold standard for irreducible anterior hip dislocations, allowing direct visualization and extraction of interposed soft tissues (e.g., rectus femoris, capsule, or labrum) blocking the reduction.
POSTERIOR HIP DISLOCATION: CLOSED REDUCTION MANEUVERS
Posterior dislocations are far more common, comprising 85% to 90% of cases. They typically result from a direct blow to the flexed knee (the classic "dashboard injury") with the hip in varying degrees of adduction and internal rotation.
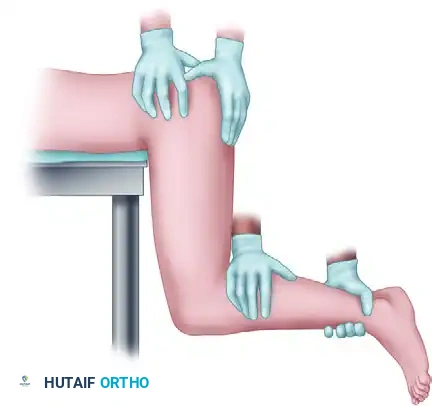
The Stimson Maneuver
The Stimson maneuver is a highly effective, gravity-assisted technique for the reduction of posterior hip dislocations. It is particularly advantageous as it minimizes iatrogenic trauma to the articular surface and requires less physical exertion from the surgeon compared to the Allis or Bigelow maneuvers.
Step-by-Step Execution:
1. Place the patient prone on the stretcher with the affected lower extremity hanging freely off the edge, flexing the hip and knee to 90 degrees.
2. The surgeon applies steady, downward longitudinal traction in line with the femur.
3. Simultaneously, an assistant stabilizes the pelvis by applying firm pressure to the sacrum and bilateral iliac crests.
4. Gentle internal and external rotation of the hip is applied to navigate the femoral head past the posterior acetabular wall.
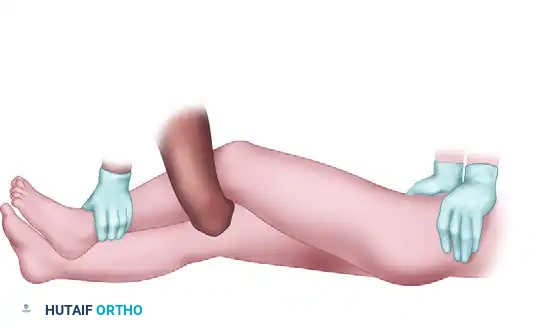
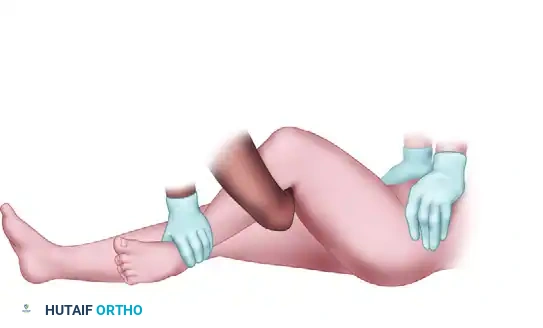
The following sequence illustrates the progressive steps of the Stimson and modified reduction maneuvers:



OPEN REDUCTION OF POSTERIOR HIP DISLOCATION
When closed reduction of a posterior dislocation is unsuccessful, or if there is a non-concentric reduction secondary to incarcerated intra-articular fragments (e.g., osteochondral loose bodies, inverted labrum, or piriformis tendon), emergent open reduction is mandated.
Surgical Technique: The Kocher-Langenbeck Approach
The Kocher-Langenbeck (posterior) approach provides excellent exposure to the posterior column, posterior wall, and the posterior aspect of the femoral head.
- Patient Positioning: Place the patient in the lateral decubitus position. Ensure the hip is extended and the knee is flexed to at least 90 degrees. This specific positioning is critical to relieve tension on the sciatic nerve, which is highly vulnerable during posterior approaches. Consider the use of skeletal traction if there is a large intra-articular fragment complicating the joint space.
- Incision and Dissection: Make a standard Kocher-Langenbeck incision. Incise the fascia lata and split the gluteus maximus in line with its fibers.
- Sciatic Nerve Identification: Identify the sciatic nerve. This can be exceptionally difficult due to the altered anatomy and hemorrhage associated with the dislocation. Attempt to locate the nerve safely on the posterior aspect of the quadratus femoris muscle, where its anatomical relationship remains relatively constant.
- Preservation of Blood Supply:
- To avoid further potential insult to the blood supply of the femoral head (specifically the ascending branch of the MCFA), do not release the quadratus femoris from the femur.
- Release the piriformis and obturator internus tendons at least 15 mm from their respective insertions on the greater trochanter.
- Capsulotomy: Make any necessary capsulotomy extension directly off the acetabular rim to preserve the retinacular vessels supplying the femoral neck.
- Joint Debridement: Remove any impediments to reduction within the acetabulum. This includes meticulous extraction of osteochondral fragments, organized hematoma, or an inverted labrum.
- Reduction: Gently guide the femoral head back into the acetabulum while strictly protecting the sciatic nerve with a blunt retractor.
🔪 Clinical Pearl: Sciatic Nerve Protection
The sciatic nerve is stretched over the dislocated femoral head in posterior dislocations. Retractors placed in the greater sciatic notch must be positioned with extreme care. Always maintain the knee in flexion during the procedure to minimize neural tension.
FEMORAL HEAD FRACTURES: THE PIPKIN CLASSIFICATION
Femoral head fractures occur in association with 5% to 15% of all hip dislocations. These injuries represent severe articular trauma and carry a high risk of post-traumatic osteoarthritis and osteonecrosis. The most universally accepted classification system for femoral head fractures is the Pipkin classification.
Pipkin Classification System
- Type I: Femoral head fracture caudad (inferior) to the fovea capitis. This area is generally considered non-weight-bearing.
- Type II: Femoral head fracture cephalad (superior) to the fovea capitis. This involves the primary weight-bearing dome of the femoral head.
- Type III: Femoral head fracture (caudad or cephalad to the fovea, Pipkin I or II) associated with a femoral neck fracture. This is a highly unstable and devascularizing injury pattern.
- Type IV: Femoral head fracture (Pipkin I, II, or III) associated with an acetabular fracture (most commonly a posterior wall fracture).
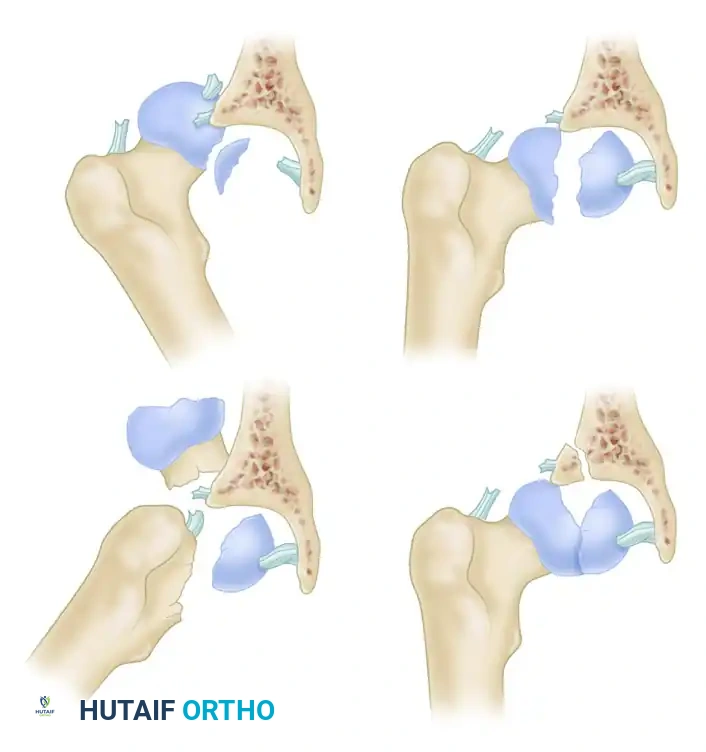
Figure: Pipkin Types I and II. Note the relationship of the fracture line to the fovea capitis.
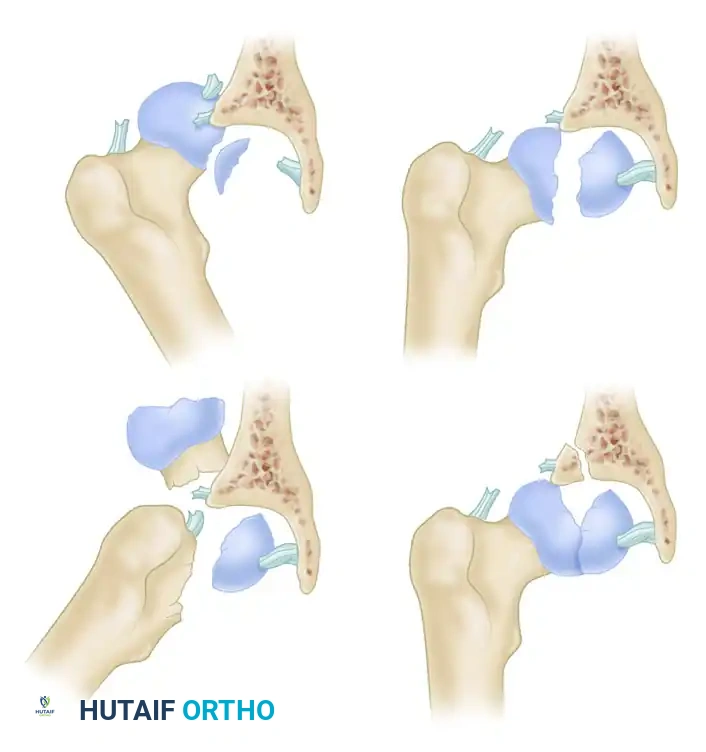
Figure: Pipkin Types III and IV. Note the associated femoral neck and acetabular fractures.
SURGICAL MANAGEMENT OF PIPKIN FRACTURES
Similar to pure hip dislocations, reduction of a hip dislocation with an associated femoral head fracture (Pipkin types I and II) should be performed immediately. Following closed reduction, a fine-cut Computed Tomography (CT) scan is absolutely essential to assess the size, location, and concentric reduction of the femoral head fragment, as well as to identify any occult intra-articular loose bodies.
Management of Pipkin Type I and II Fractures
- Type I: Most orthopedic trauma surgeons argue that large Pipkin type I femoral head fragments, especially with fragment displacement, should be rigidly fixed. With larger femoral head fragments, the likelihood of joint instability increases. More controversy exists over smaller, comminuted femoral head fragments. Some recommend acute excision of small fragments to prevent third-body wear, whereas others believe the fragment can be treated nonoperatively if it does not impede concentric reduction.
- Type II: Assessment of reduction with CT is essential. Any Pipkin type II fracture that is not anatomically reduced must be treated surgically to restore the weight-bearing articular surface.
Surgical Approach for Types I & II:
Reduction and fixation can be accomplished through an anterior (Smith-Petersen) approach, a posterior (Kocher-Langenbeck) approach, or a posterior approach with surgical dislocation. We typically utilize a Smith-Petersen approach for Pipkin type I and II femoral head fractures, as it provides direct, orthogonal access to the anterior and superior aspects of the femoral head. The fractures usually are fixed with countersunk 2.7-mm or 3.5-mm cortical screws, or headless compression screws, ensuring the hardware is buried beneath the articular cartilage.
Management of Pipkin Type III Fractures
Pipkin type III fractures are rare, and high-level data to guide the management of these injuries are lacking. The presence of a femoral neck fracture drastically increases the risk of AVN.
* Young Patients: In physiologically young patients, we usually proceed with emergent open reduction and internal fixation (ORIF) of both the femoral neck and the femoral head to preserve the native joint.
* Older Patients: Physiologically older patients are best treated with arthroplasty (Total Hip Arthroplasty or Hemiarthroplasty), as the risk of fixation failure and AVN is unacceptably high.
Management of Pipkin Type IV Fractures
Pipkin type IV fractures most commonly consist of a femoral head fracture combined with a posterior wall acetabular fracture. This complex combination may be best treated with surgical dislocation of the hip (the Ganz approach).
Treatment generally is dictated by the morphology of the acetabular fracture. A recent multicenter study evaluating the complications associated with surgical hip dislocation concluded that the procedure is safe with a low incidence of complications. Of 334 hips treated with surgical hip dislocation for various hip pathological processes, none developed osteonecrosis. The rate of trochanteric nonunion was a mere 1.8%.
Although the number of hips in this specific series is large, only one patient had surgical dislocation strictly for trauma. However, osteonecrosis also has not been reported as a complication in series where this approach was used specifically for the treatment of femoral head fractures or for joint debridement and treatment of acetabular fractures. Surgical dislocation allows 360-degree, excellent visualization for open reduction and internal fixation of large femoral head fragments, or precise debridement and excision of small, irreparable femoral head fragments.
COMPLEX ASSOCIATED INJURIES: FEMORAL NECK AND SHAFT FRACTURES
Closed reduction of a posterior hip dislocation can be severely complicated by the presence of an ipsilateral femoral neck or femoral shaft fracture.
🚨 Surgical Warning: The Ipsilateral Femoral Neck Fracture
An anteroposterior (AP) view of the pelvis must be obtained and reviewed before any reduction attempt. Attempts at closed reduction of a posterior hip dislocation with an associated femoral neck fracture may result in catastrophic displacement or further displacement of the femoral neck fracture, leading to irreversible injury to the retinacular vessels supplying the femoral head.
- Management of Dislocation with Neck Fracture: Physiologically older patients with this combined injury should be treated directly with arthroplasty. Younger patients should be treated with open reduction of the femoral neck fracture (if displaced), rigid fixation, and then reduction of the hip dislocation. We do not attempt closed reduction of dislocated hips with associated femoral neck fractures unless the neck fracture is strictly nondisplaced and can be provisionally stabilized with percutaneous guidewires prior to the reduction maneuver.
- Management of Dislocation with Shaft Fracture: Dislocated hips with ipsilateral femoral shaft fractures are treated differently. An attempt at closed reduction should be made. However, the lack of a continuous lever arm makes this difficult. If difficulty is encountered, the patient is taken emergently to the operating room. A 5.0-mm Schanz pin is inserted into the proximal aspect of the femoral shaft (proximal to the fracture) to act as a "joystick" to aid in the reduction of the hip joint, followed by standard intramedullary nailing of the shaft.
POSTOPERATIVE CARE AND REHABILITATION PROTOCOLS
The postoperative rehabilitation protocol must be tailored to whether the injury was a pure dislocation or a fracture-dislocation.
Pure Hip Dislocations
After the successful reduction of pure hip dislocations (without associated fractures), weight-bearing is generally allowed as tolerated (WBAT) on crutches, with progression as pain allows. Patients with posterior hip dislocations are strictly instructed in posterior hip precautions (avoiding hip flexion past 90 degrees, adduction across the midline, and internal rotation) and must follow these for at least 6 weeks to allow capsular healing. Patients are followed closely with serial radiographs for the first 2 years, because if osteonecrosis is going to develop, it likely will present within this critical time frame.
Hip Dislocations with Femoral Head (Pipkin) Fractures
Hip dislocations with associated femoral head fractures that undergo internal fixation are managed with touch-down weight bearing (TDWB) for 12 weeks to protect the articular cartilage repair and hardware.
* Exception: A patient who undergoes isolated femoral head fragment excision (without fixation) is allowed to bear weight as tolerated (WBAT) on crutches immediately.
* Precautions: All patients are instructed on strict hip precautions based on the surgical approach used (anterior vs. posterior) and are told to follow these for at least the first 6 weeks after surgery to prevent recurrent instability. Routine clinical and radiographic surveillance for AVN and post-traumatic arthritis remains mandatory for a minimum of 24 months.
