Reduction and Stabilization of the Distal Radioulnar Joint following Galeazzi Fractures
DEFINITION
Fracture of the radial shaft with an associated distal radioulnar joint (DRUJ) dislocation ( FIG 1A,B)It is well established that anatomic stabilization of the radial shaft fracture typically results in a stable DRUJ that can be treated nonoperatively with a period of immobilization.When the DRUJ is either irreducible or unstable, following anatomic reduction and compression plating of the radius fracture, operative stabilization of the DRUJ is required.Pediatric injury is not discussed in this chapter.
ANATOMY


FIG 1 • Classic Galeazzi injury. A. A distal-third radial shaft fracture with ulnar angulation of the distal fragment, radial shortening, and DRUJ widening. B. Apex dorsal angulation of radial shaft fracture with dorsal dislocation of ulnar head. Triangular fibrocartilage complex (TFCC)The dorsal and volar radioulnar ligaments of the TFCC are considered the primary stabilizers of the DRUJ. 18 The deep fibers of the radioulnar ligaments attached at the fovea are located at the base of the ulnar styloid.For this reason, in the less common instance when an ulnar styloid base fracture accompanies a Galeazzi fracture-dislocation, fixation of ulnar styloid fracture may restore DRUJ stability.Distal interosseous membrane (DIOM) and distal oblique bundle (DOB)The DIOM lies deep to the pronator quadratus and connects the radius and ulna ( FIG 2A).Biomechanical studies demonstrate that the distal membranous portion of the interosseous membrane functions as a secondary stabilizer of the DRUJ. 14,20When present, the DOB originates at the distal ulna and inserts at the inferior rim of the sigmoid notch of the radius blending with the capsular tissue of the DRUJ. 18 Cadaveric studies report the DOB is present in 40% of specimens (FIG 2B).15Moritomo 14 has hypothesized that in Galeazzi fracture-dislocations, when there is loosening but not rupture of the DOB, instability can be managed by anatomic reduction of the radius.Radius reduction and the subsequent retensioning of the DOB restore stability even when a TFCC injury ispresent. Persistent DRUJ instability after radial fracture restoration may be the result of DOB disruption. 14 RadiusThe majority of Galeazzi fracture-dislocations occurs in distal third of the radius but can occur anywhere along the radius. 12Greater than 50% of radial shaft fractures less than 7.5 cm from the distal radial articular surface are associated with injury to the DRUJ compared to 6% of more proximal radial shaft fractures. 17
PATHOGENESIS




NATURAL HISTORY
Galeazzi fracture-dislocations account for approximately 6% of all closed forearm fractures in adults with a male predominance. 13Nonoperative management results in an apex dorsal radius malunion with a dorsally prominent ulnar head. Limitations in pronation, supination, wrist flexion, and wrist extension are common. Pain occurs at the ulnar side of the wrist over the prominent ulnar head.In contrast, early operative management typically results in excellent or satisfactory results following anatomic reduction and stabilization of radius fracture and DRUJ.
PATIENT HISTORY AND PHYSICAL FINDINGS
A high percentage of associated injuries occur, and life-threatening injuries should be assessed first. Patients report severe forearm and wrist pain. Deformity is typically present with a prominent ulnar head. Open injuries of the radius and ulna can occur, and close evaluation of the skin should be performed.Neurovascular injuries and compartment syndrome have not been widely reported with a Galeazzi injury but should be assessed for completeness and documented even when “negative.” Therefore, all splints, dressings, and clothing need to be removed for proper inspection and palpation and neurovascular examination.Examination of the DRUJ of the noninjured contralateral extremity is helpful prior to surgical management of the Galeazzi injury to understand the patient's native DRUJ laxity, especially at the limits of pronation and supination.
IMAGING AND OTHER DIAGNOSTIC STUDIES
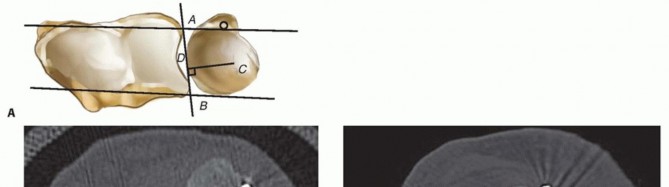
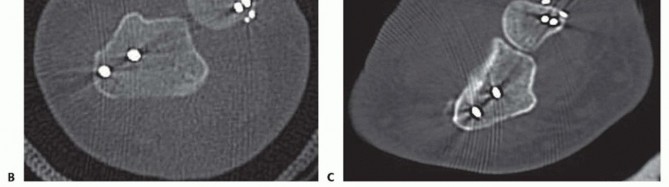
FIG 3 • A. Radioulnar ratio method to measure DRUJ subluxation on a CT scan. See text for details. B. Axial CT scan demonstrating dorsally dislocated ulna following ulnar styloid open reduction internal fixation (ORIF). C. Axial CT scan following reduction and pinning of the dislocated DRUJ. (A: Adapted from Lo IK, MacDermid JC, Bennett JD, et al. The radioulnar ratio: a new method of quantifying DRUJ subluxation. J Hand Surg Am 2001;26:236-243.)
DIFFERENTIAL DIAGNOSIS
Isolated radial shaft fractureRadial head or neck fracture with DRUJ injury (Essex-Lopresti lesion) Distal radius fracture with DRUJ injuryUlnar-sided carpal or ligamentous injuries
NONOPERATIVE MANAGEMENT
No role exists for nonoperative care of a Galeazzi injury in a patient who is medically able to have surgery. Hughston's 7 classic series demonstrated that 35 of 38 patients treated without surgery resulted in failure.
SURGICAL MANAGEMENT
Galeazzi fracture-dislocations need to be treated expeditiously. Delay in treatment more than 10 days may negatively impact final range of motion of the forearm. 13The need for operative stabilization of the DRUJ can only be determined intraoperatively after the radius fracture has been stabilized, and the DRUJ is examined for instability.
PREOPERATIVE PLANNING
Preoperatively, the surgeon decides the surgical approach and method of fixation of the radius fracture. It is presumed that at a minimum, the TFCC is injured and the DRUJ will be evaluated intraoperatively.Decision making and technique regarding approach and fixation of the radius has been described in detail in the chapter entitled Open Reduction Internal Fixation of Diaphyseal Forearm Fractures (also in Chap. 1).Examination under anesthesia of the uninjured wrist is performed.Depending on intraoperative findings, the surgeon must be prepared to pin the radius to the ulna, explore the dorsal DRUJ, and possibly repair the TFCC using either open or an arthroscopic technique.Evaluation of DRUJ instability following radial fixationThe decision to proceed with operative stabilization of the DRUJ for residual instability following radius fixation is not straightforward. Unfortunately, there is no reference standard for evaluating DRUJ stability.DRUJ instability should always be evaluated after radius stabilization.Classically, the elbow is flexed to 90 degrees, and the ulna is stressed both volarly and dorsally in supination, neutral, and pronation while laxity, subluxation, or dislocation is assessed. Any laxity less than full dislocation is difficult to quantify even when measured against the examination of the uninjured wrist.Giannoulis and Sotereanos 4 suggested that instability is confirmed following fixation of the radius if the ulnar head can be translated dorsally out of the sigmoid notch (with the forearm fully supinated).Jupiter 8 has suggested that laxity at the DRUJ should be expected (in displaced distal radius fractures) and that the traditional method of stressing the ulna dorsally and volarly is subjective and lacks interobserver validity. He recommends that the surgeon compress the ulna to the radius after bony fixation and rotate the hand and wrist. Only when a palpable “clunk” is present is true instability present. This implies that the distal oblique band of the interosseous membrane has been disrupted.
POSITIONING
The patient is placed supine with the injured arm out on a radiolucent arm table. A nonsterile padded pneumatic tourniquet is placed on the upper arm.If arthroscopy is planned to address an unstable DRUJ, the upper arm should be stabilized to the arm table or a distraction device be made available.
APPROACH
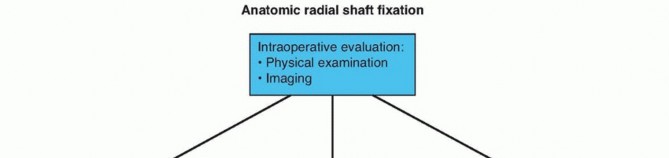
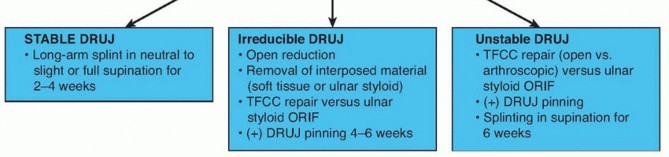
FIG 4 • Algorithm for management of DRUJ stability. Treatment of the unstable DRUJ after radial fixation with large ulnar styloid base fractureInstability with an associated ulnar styloid fracture is less frequent in Galleazi injuries. Maintenance of stabilityhas been reported with operative fixation of the ulnar styloid base. 10 Screw or tension band fixation is commonly performed.Treatment of the irreducible DRUJ after radial fixationIf the DRUJ remains irreducible after anatomic reduction of the radial shaft fracture, soft tissue interposition is suspected. Open reduction to remove soft tissue and TFCC repair should be performed. 10
TECHNIQUES
RADIUS AND ULNA TRANSFIXATION PINNING
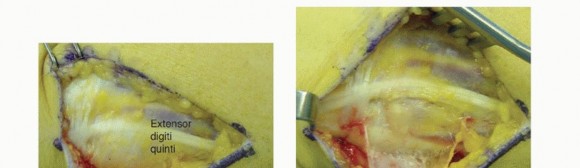
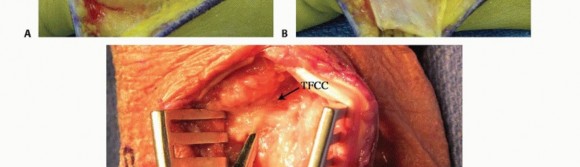
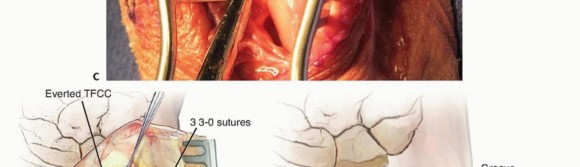
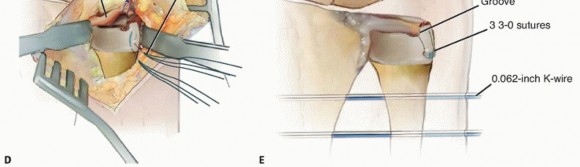
TECH FIG 2 • Open DRUJ/TFCC exposure and repair. A. Incision. B. Extensor retinaculum opened exposing fifth compartment. C. TFCC and DRUJ exposed. D. 3-0 nonabsorbable sutures placed through TFCC and ulna bone tunnels. E. Final construct demonstrating transfixation with 0.062-inch K-wires and TFCC repair.




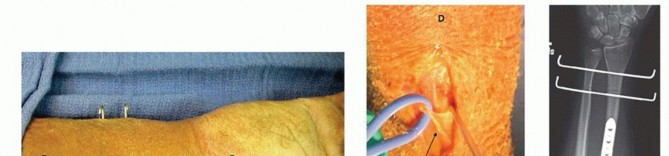
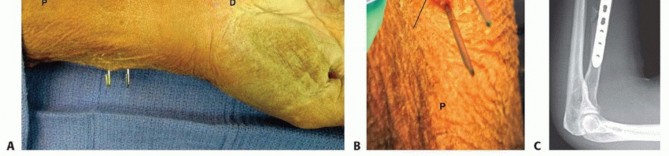
TECH FIG 3 • Wrist arthroscopy to address TFCC injury. A. The patient is placed supine with an arm board; a strap is used to securely fashion the arm to the table. A boom is placed on the contralateral side. B. Finger traps are positioned, the weight is attached. Fluoroscopy is used to access DRUJ reduction. C.
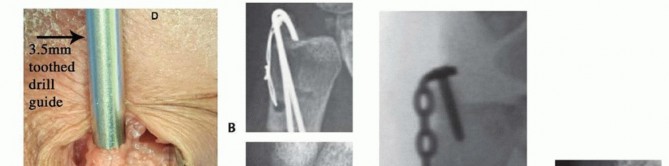
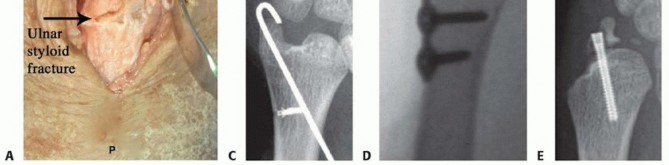
TECH FIG 4 • Ulnar styloid fracture fixation. A. The distal ulna is exposed at the ulnar styloid and a 3.5-mm drill guide is used to reduce the fracture and to pass K-wires. B. Anteroposterior (AP) radiograph of a tension band open reduction internal fixation (ORIF). C. Tension band construct with a suture anchor. D. ORIF with plate and screw construct. E. Loss of fixation using headless compression screw. A transverse (dorsal to volar) 2-mm drill hold is made proximally through the ulnar neck, and a 27-gauge wire is placed through the TFCC at its insertion on the ulnar styloid.A figure-of-eight bend is made, and one limb is passed volar to dorsal through the transverse bone hole, whereas the other is passed dorsal to volar.The wire is then twisted to tension, and the pins are bent and cut. The bent tips are pointed radially and driven into the styloid with a small bone tamp, capturing the wire ( TECH FIG 4B).Alternatively, after placing the pins through the ulnar styloid, a 2-0 suture anchor can be placed in the ulnar neck and the sutures passed in opposite directions around the styloid. The limbs are tied down to the medial ulnar shaft, and the pins are bent and cut as previously discussed ( TECH FIG 4C).Plate and screw construct may also be used for buttress effect, but implant prominence must be considered ( TECH FIG 4D).Headless compression screw fixation is advocated by some. We have noted frequent failure and malreduction with this technique. If screw fixation is used, bicortical fixation is recommended ( TECH FIG 4E).If the DRUJ is still unstable, proceed with radioulnar transfixation pinning. Wound closure, sterile dressings, and long posterior splint are applied.P.250PEARLS AND PITFALLS
|1.Confirm reduction with intraoperative radiographs. Immobilize forearm|Radius is anatomicallyreduced and DRUJ is irreducible.1.Proceed with open reduction to removed interposed soft tissuestructures and open repair of TFCC (with radioulnar pinning).Radius is anatomicallyreduced and DRUJ is grossly unstable.1.Proceed with radioulnar pinning (4-6 weeks) verses supination splintingfor 6 weeks.2.Consideration can be giving to open verses arthroscopic TFCC repair (with radioulnar pinning).Follow-up examination1.Confirm at each follow-up DRUJ reduction radiographically. If there isany question of subluxation, evaluate axial imaging with CT scan.in neutral to slight supination in long-arm cast or splint in neutral for 2-4 weeks to allow for TFCC healing.Radius is stabilized and DRUJ is stable.
POSTOPERATIVE CARE
Stable internal fixation of the radius and stable DRUJLong-arm splint with forearm in neutral for 2 weeks.A retrospective review of patients with a stable DRUJ following radial fixation found that immobilization in supination for 4 weeks has no advantage over immobilization in neutral for a shorter time. 16Internal fixation of radius and DRUJ stabilization (pinning or open TFCC repair)Long-arm splint with forearm in neutral to slight supination for 4 to 6 weeks.If the radius and ulna have been pinned together, the patient is seen every 2 to 3 weeks to evaluate pin sites when they are left out of the skin.Full range of motion of the shoulder as allowed with long-arm immobilization. At minimum, patients are encouraged to do shoulder pendulum exercises. Finger range of motion is encouraged as well.At each postoperative visit, radiographs must confirm reduction of the DRUJ. If there is any concern that the DRUJ is not reduced, CT scan is obtained.Pins are removed at 4-6 weeks. Following pin removal, pronosupination exercises are encouraged. Supervised therapy is recommended.
OUTCOMES
A study of 17 patients with near-anatomically reduced radial shaft fractures, 10 without a DRUJ dislocation and 7 with a DRUJ dislocation, found comparable results whether the DRUJ was injured or not. There was an average follow-up of 19 years, and neither pinning of the radius to ulna nor TFCC repair wasperformed. 19Specifically, no significant differences in the Mayo Modified Wrist Score or Disabilities of the Arm, Shoulder, and Hand questionnaire were found. No differences in DRUJ laxity compared to the contralateral wrist were present. 16Pinning the radius to the ulna in a position of DRUJ reduction is the most commonly reported procedure in larger cases series, with excellent results reported. 10,17A recent study evaluated 40 patients who had a single 1.2- or 1.6-mm smooth stainless steel pin placed proximal to the sigmoid notch with the forearm in supination for 6 weeks for DRUJ instability after radial fixation. At 6.8-year follow-up, none of these patients required more DRUJ surgery or had persistentDRUJ instability. 10Instability with an associated ulnar styloid fracture is less frequent in Galleazi injuries. Maintenance ofstability has been reported with operative fixation of the ulnar styloid base. 16 Screw or tension band fixation is commonly performed.Classically, Mikić 12 defined an excellent result as radius union, perfect alignment, no loss of length, no subluxation of the DRUJ, and no limitation of supination or pronation. Using this criteria, Rettig andRaskin 17 reported 95% excellent results in 40 Galeazzi fracture-dislocations. Twenty-seven patients demonstrated DRUJ stability after radial fixation only. Ten patients demonstrated DRUJ instability and were treated with radioulnar pinning with two 1.6-mm smooth stainless steel pins only. Three patients had irreducible DRUJs and required open reduction, TFCC repair, and pinning of the DRUJ. None of the patients treated for an unstable or irreducible DRUJ had a poor result.Loss of pronosupination and wrist flexion are commonly reported, although the amount reported varies significantly in published literature.
COMPLICATIONS
Specific to Galeazzi fracture-dislocations, subluxation or dislocation of the DRUJ can occur. This is most commonly a result of nonanatomic alignment of the radius.Pin site infection and pin breakage of radioulnar transfixation pins can also occur.As with all forearm fractures, malunion and nonunion can occur, although rare with appropriately applied compression plating.Both open and arthroscopic TFCC repair are associated with dorsal ulnar nerve cutaneous branch postoperative neuropathy. Notably, there is some evidence that the risk is increased with open repair. 1
REFERENCES
- Anderson ML, Larson AN, Moran SL, et al. Clinical comparison of arthroscopic versus open repair of triangular fibrocartilage complex tears. J Hand Surg Am 2008;33(5):675-682.
- Cetti NE. An unusual cause of blocked reduction of the Galeazzi injury. Injury 1977;9(1):59-61.
- Garcia-Elias M, Hagert E. Surgical approaches to the distal radioulnar joint. Hand Clin 2010;26(4):477-483.
- Giannoulis FS, Sotereanos DG. Galeazzi fractures and dislocations. Hand Clin 2007;23(2):153-163.
- Hagert E, Hagert CG. Understanding stability of the distal radioulnar joint through an understanding of its anatomy. Hand Clin 2010;26(4):459-466.P.251
- Henry AK. Extensile Exposure, ed 2. Baltimore: Williams & Wilkins, 1970.
- Hughston JC. Fracture of the distal radial shaft; mistakes in management. J Bone Joint Surg Am 1957;39-A(2):249-264.
- Jupiter JB. Commentary: the effect of ulnar styloid fractures on patient-rated outcomes after volar locking plating of distal radius fractures. J Hand Surg Am 2009;34(9):1603-1604.
- Kleinman WB. Repairs of chronic peripheral tears/avulsions of the triangular fibrocartilage. In: Blair WF, ed. Techniques in Hand Surgery. Baltimore: Williams & Wilkins, 1996.
- Korompilias AV, Lykissas MG, Kostas-Agnantis IP, et al. Distal radioulnar joint instability (Galeazzi type injury) after internal fixation in relation to the radius fracture pattern. J Hand Surg Am 2011;36(5):847-852.
- Lo IK, MacDermid JC, Bennett JD, et al. The radioulnar ratio: a new method of quantifying distal radioulnar joint subluxation. J Hand Surg Am 2001;26(2):236-243.
- Mikic' ZD. Galeazzi fracture-dislocations. J Bone Joint Surg Am 1975;57(8):1071-1080.
- Moore TM, Klein JP, Patzakis MJ, et al. Results of compression-plating of closed Galeazzi fractures. J Bone Joint Surg Am 1985;67(7): 1015-1021.
- Moritomo H. The distal interosseous membrane: current concepts in wrist anatomy and biomechanics. J Hand Surg Am 2012;37(7): 1501-1507.
- Noda K, Goto A, Murase T, et al. Interosseous membrane of the forearm: an anatomical study of ligament attachment locations. J Hand Surg Am 2009;34(3):415-422.
- Park MJ, Pappas N, Steinberg DR, et al. Immobilization in supination versus neutral following surgical treatment of Galeazzi fracture-dislocations in adults: case series. J Hand Surg Am 2012;37(3): 528-531.
- Rettig ME, Raskin KB. Galeazzi fracture-dislocation: a new treatment-oriented classification. J Hand Surg Am 2001;26(2):228-235.
- Thomas BP, Sreekanth R. Distal radioulnar joint injuries. Indian J Orthop 2012;46(5):493-504.
- van Duijvenbode DC, Guitton TG, Raaymakers EL, et al. Long-term outcome of isolated diaphyseal radius fractures with and without dislocation of the distal radioulnar joint. J Hand Surg Am 2012;37(3): 523-527.
- Watanabe H, Berger RA, Berglund LJ, et al. Contribution of the interosseous membrane to the distal radioulnar joint constraint. J Hand Surg Am 2005;30(6):1164-1171.
