Reconstruction for Missed Monteggia Lesion
DEFINITION
Monteggia fracture-dislocations are rare complex traumatic upper limb injuries defined by fracture of the ulna associated with proximal radioulnar joint dissociation and radiocapitellar joint dislocation. Theseinjuries typically affect patients between 4 and 10 years of age. 19The diagnosis of an acute Monteggia fracture-dislocation is often missed by skilled radiologists, emergency room physicians, pediatricians, and orthopaedic surgeons. 4,21Late presentation of a previously undetected traumatic dislocation of the radial head occurs.In children with a seemingly isolated dislocation of the radial head, scrutiny of forearm radiographs often demonstrates plastic deformation or fracture malunion of the ulna ( FIG 1). The combination of these radiographic findings establishes the diagnosis of a chronic Monteggia fracture-dislocation or chronicMonteggia lesion, as opposed to a congenital dislocation of the radial head. 4Patients with chronic Monteggia lesions can present for evaluation at a variety of time points. 21In some children, radial head dislocation is first noted several weeks after initiating treatment for a misdiagnosed, isolated ulnar fracture.In other patients, the diagnosis may not be established for months to years following injury due to the development of pain, loss of motion, and/or valgus malalignment.Even a few weeks after injury, treatment of a Monteggia lesion is much more complicated than acute recognition and treatment. 21Nonetheless, due to pain, restriction of motion, and functional disability, most patients with chronic Monteggia lesions are offered surgical correction.
ANATOMY


FIG 1 • Chronic Monteggia lesion in a 7-year-old girl with a 5-week history of elbow pain and loss of motion following trauma. A. Initial lateral forearm radiograph demonstrates an abnormal ulnar bow line, or deviation of the ulna from its normally straight dorsal border, and is suggestive of plastic deformation. Anterior dislocation of the radial head is also noted. These findings were not detected in the emergency department where dedicated elbow films were not obtained, and the child was diagnosed with an elbow sprain. B. AP elbow radiograph 5 weeks after injury demonstrates a normal radiocapitellar line with a poorly characterized calcification overlying the lateral aspect of the capitellum. On the AP view, the radiocapitellar line is often normal in acute or chronic Bado type I Monteggia lesions. C. Lateral elbow radiograph 5 weeks after injury demonstrates disruption of the radiocapitellar line and anterior translation of the radial head. There is calcification of the displaced annular ligament and anterior elbow capsule, which can be mistaken for heterotopic ossification.
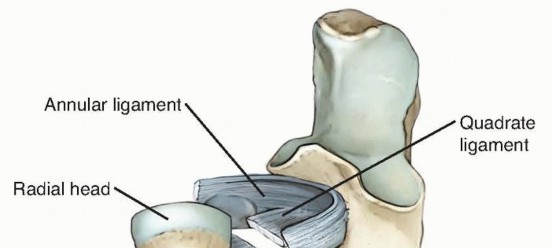
FIG 2 • Ligamentous anatomy of the proximal radioulnar joint. The annular ligament is the principal stabilizer of the radial head during forearm rotation. In supination, the annular and quadrate ligaments are taught and increase stability of the proximal radioulnar joint.
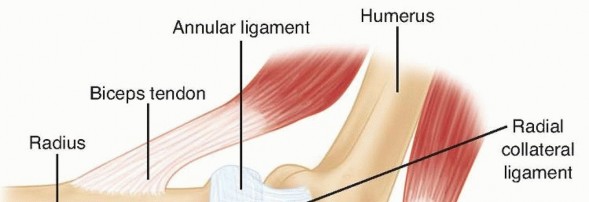
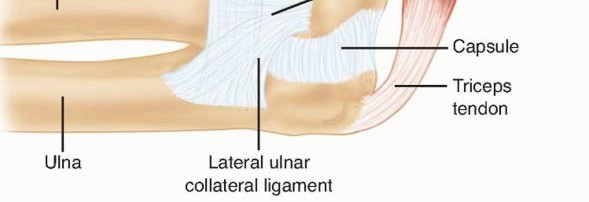
FIG 3 • The Y-shaped lateral ligamentous complex of the elbow consists of the radial collateral ligament, the lateral ulnar collateral ligament, and the annular ligament.
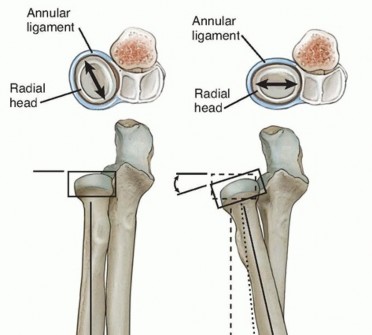
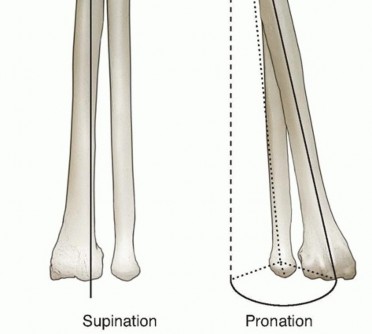
FIG 4 • The radial head is most stable with the forearm in a position of supination. The radial head is elliptical and is stabilized at the proximal radioulnar joint by the annular ligament. In forearm supination, the long axis of the radial head is perpendicular to the lesser sigmoid notch, causing the annular ligament and the anterior segment of the quadrate ligament to tighten and maximize stability.




FIG 5 • Diagram of the anterior elbow. The radial nerve emerges above the elbow in the interval between the brachioradialis and the brachialis. The radial nerve divides into the superficial sensory branch and the posterior interosseous branch. The posterior interosseous nerve passes under the arcade of Frohse and through the supinator. The proximity of the posterior interosseous nerve to the radial head and neck makes the nerve susceptible to injury during reconstruction of a chronic Monteggia lesion.
PATHOGENESIS
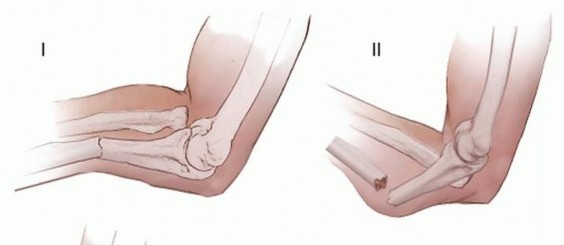
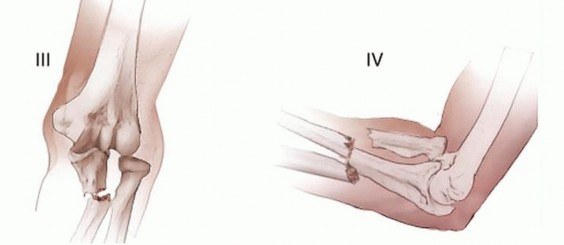
FIG 6 • Schematic diagram of the Bado classification of Monteggia fracture-dislocations, which is based on the direction of the radial head dislocation and the ulnar fracture. Type I, anterior dislocation, is the most common pattern in children. Type II is posterior dislocation. Type III, lateral dislocation, is the second most common Monteggia lesion in children. Type IV is anterior dislocation with radial shaft fracture distal to the associated ulnar fracture. Bado type II lesions are characterized by posterior or posterolateral dislocation of the radial ahead associated with a posterior ulnar diaphyseal or metaphyseal fracture. This is the most common pattern in adults butrepresents approximately 5% of Monteggia lesions in children. 19Bado type III lesions demonstrate lateral dislocation of the radial head and are associated with an apex lateral (varus) fracture of the proximal ulna. This is the second most common Monteggia lesion in children andrepresents nearly 30% of all pediatric injuries. 19Bado type IV lesions are characterized by anterior dislocation of the radial head and fractures of both the radius and ulna. Type IV lesions are rare in children.The initial diagnosis of a Monteggia fracture-dislocation is often missed by qualified physicians. 4,21 Because the ulna heals rapidly in children, a chronic Monteggia lesion can develop over a period of 3 to 4 weeks. Due to the frequency of Bado type I lesions, most chronic Monteggia lesions in children are characterized by anteriordislocation of the radial head and apex anterior ulnar fracture malunion or plastic deformation. 13,21 Suboptimal treatment of the ulnar fracture in an acute Monteggia lesion can also result in unrecognized or late subluxation or dislocation of the radial head, resulting in a chronic Monteggia lesion.19In general, only plastic and greenstick ulnar fractures should be treated with closed reduction and casting. All complete fractures should be treated surgically to avoid late instability. 20Transverse or short oblique ulnar fractures should be treated with intramedullary pin fixation and long oblique or comminuted fractures should be treated with open reduction and plate fixation. 20Always obtain dedicated elbow radiographs to evaluate congruency of the radiocapitellar reduction following reduction of the ulnar fracture.Chronic Monteggia lesions can result in substantial loss of function and are far more complex than acute injuries in terms of surgical decision making and management. 21
NATURAL HISTORY
Initial reports on chronic Monteggia fracture-dislocations suggested that the natural history of the untreated lesion was not problematic. In these reports, results from late surgical reconstruction were complicated by scarring, arthrosis, and loss of motion. For these reasons, the classic treatment was neglect and radial head excision at skeletal maturity if necessary.More recent data suggests that most chronic Monteggia lesions are not tolerated well over time. 6,21 Patients can develop pain, arthrosis and loss of motion, functional impairment, progressive cubitus valgus, and late neuropathy even if initial symptoms are mild.2,6,21 Loss of elbow flexion and forearm pronation can occur.21 Thebest treatment for this problem remains preventative.Tardy ulnar, median, and posterior interosseous nerve palsy have been reported secondary to cubitus valgus and radial head dislocation in the setting of chronic Monteggia lesions. 3,11
PATIENT HISTORY AND PHYSICAL FINDINGS
Most patients presenting with a chronic Monteggia lesion note a distinct history of trauma. The traumatic episode often involves significant force and is frequently characterized by a fall on to an outstretched hand with the elbow in extension and the forearm in pronation.A history of trauma aids in distinguishing a traumatic radial head dislocation form a congenital radial head dislocation.A history of acute elbow pain and temporary loss of motion in a child younger than 4 years of age secondary to minor trauma should prompt consideration of radial head subluxation or nursemaid's elbow. Radiographs will reveal an aligned radial head and no ulnar fracture or deformity. Children with a nursemaid's elbow usually have prompt resolution of discomfort and restoration of movement following closed reduction maneuvers.The timing of the injury and nature of prior medical treatment should be clarified. Patients presenting within 2 weeks of injury may still be candidates for standard treatment strategies for acute Monteggia fracture-dislocations.Physical examination may reveal cubitus valgus as well as loss of forearm rotation and elbow flexion. Nerve functional testing should be performed.On inspection, anterior fullness in the cubital fossa may be detected. This corresponds to a palpable anterior dislocation of the radial head. The dislocated radiocapitellar joint should be palpated during forearm rotation to detect crepitation or other signs of elbow arthrosis.The elbow carrying angle should be evaluated. The carrying angle in normal children increases with age and averages 9.3 degrees in males and 11.5 degrees in females. 7 Patients with chronic Monteggia lesionsfrequently demonstrate cubitus valgus and can present with carrying angles that exceed 30 degrees. 21 For some patients and families, this represents a significant aesthetic concern.Elbow motion and forearm rotation should be precisely assessed. Normal elbow motion varies by child andaverages 4 degrees of hyperextension to 145 degrees of flexion. 7 Loss of elbow motion is common, particularly in chronic Bado type I Monteggia lesions where anterior dislocation of radial head results inabutment against the humerus. 21 Elbow flexion is limited in the majority of patients with chronic Bado type I lesions and averages 110 degrees.13 Terminal elbow flexion may be associated with visible discomfort. Lossof forearm rotation, particularly pronation, is also common. 21 Many children with chronic Monteggia lesions demonstrate compensatory radiocarpal and midcarpal rotation which can obscure assessment of true forearm rotation. In order to careful track true forearm rotation, the examiner must assess rotation of the radial styloid relative to the axis of the ulna.P.96A detailed neurologic examination should be performed to assess peripheral nerve function, including the ulnar nerve, median nerve, and posterior interosseous nerve (see Exam Table at the end of the volume). Sensibility can be assessed subjectively with light touch or objectively with two-point discrimination in a cooperative child older than 5 years of age. Hand and wrist strength is tested.In tardy ulnar nerve palsy, patients may demonstrate diminished sensibility at the volar pad of the small finger (autonomous zone). Patients may also present with intrinsic muscle atrophy, clawing of the small finger and ring finger, diminished digital abduction strength, a positive Froment sign, or a positiveWartenberg sign. 3Patients with a tardy posterior interosseous nerve palsy will demonstrate weakness with fingermetacarpophalangeal joint extension and thumb retropulsion. 11 Because the extensor carpi radialis longus is innervated by the radial nerve, patients may demonstrate preserved wrist extension with a tendency toward radial deviation. Sensation at the first dorsal web space is typically normal.
IMAGING AND OTHER DIAGNOSTIC STUDIES
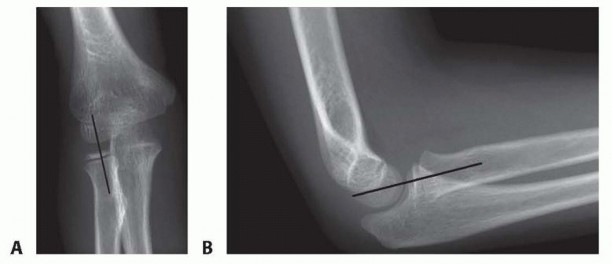
FIG 7 • In a normal elbow, the radiocapitellar line generally bisects the capitellum. A disruption of the radiocapitellar line is concerning for radial head subluxation or dislocation but due to variation in the normal pediatric population is not pathognomonic for a Monteggia lesion. A. AP elbow radiograph in a 7-year-old girl demonstrating a normal radiocapitellar line. B. Lateral elbow radiograph in a 7-year-old girl demonstrating a normal radiocapitellar line.

FIG 8 • Congenital dislocation of the radial head in a 7-year-old boy with limited forearm rotation. A. AP radiograph demonstrates an abnormal radiocapitellar line. B. Lateral elbow radiograph also demonstrates an abnormal radiocapitellar line with anterior dislocation of the radial head. The dysplasia of the radial head and hypoplastic appearance of the capitellum are consistent with a congenital etiology despite the anterior radial head dislocation which is more frequently seen following trauma. (From Shah AS, Waters PM. Monteggia fracture-dislocation in children. In: Rockwood and Wilkins' Fractures in Children, ed 8. Philadelphia: Lippincott Williams & Wilkins. In press.)
DIFFERENTIAL DIAGNOSIS
Congenital radial head dislocation (see FIG 8) Nursemaid's elbow (pulled elbow, radial head subluxation) Isolated traumatic radial head dislocationTraumatic elbow dislocation
NONOPERATIVE MANAGEMENT
The indications for reconstruction of a chronic Monteggia lesion are not well defined in the literature.Nonoperative management can be considered in an asymptomatic child, but yearly clinical and radiographic follow-up is recommended.There are important contraindications for chronic Monteggia reconstruction. Some surgeons have advocated patient age (before age 12 years) or time from injury ( <3 years) as discriminating factors for surgicalconsideration, 10,17 but it is more important to consider the morphology of the radial head and thecapitellum. 18,22,25 In older patients or more chronic lesions, MRI can be obtained to further delineate cartilage quality and potential joint congruity. Patients with radial head enlargement or deformity, flattening of the capitellum, or joint arthrosis are not candidates for reconstruction.10,22,25 In these patients, radial head excisioncan be considered if pain does not resolve with nonoperative means but does place the patient at risk ofdeveloping wrist pain or progressive cubitus valgus.
SURGICAL MANAGEMENT
At present, there is limited evidence and conflicting retrospective literature on the management of chronic Monteggia lesions. Evidence regarding management of chronic Monteggia lesions is limited to small, single-center retrospective case series.Unless there is concern regarding the morphology of the radial head or capitellum, we believe that symptomatic patients with chronic Monteggia lesions are candidates for surgical reconstruction.Descriptions of surgical reconstructions for patients with chronic Monteggia lesions include annular ligament repair or reconstruction alone, 2,8,12,13,21,22 ulnar osteotomy alone,5,9,10,12,14,21,23 combined ulnar osteotomyand annular ligament repair/reconstruction, 8,12,13,14,17,21,22,25,28 and radial osteotomy.12,13,25 The relative merit of each surgical technique has not been well elucidated and is likely to vary by patient and lesion.However, almost every series advocates for an ulnar realignment osteotomy when reconstructing a chronic Monteggia lesion. The principal controversy revolves around whether an annular ligament reconstruction should be performed in addition to the ulnar osteotomy.The technique for open reduction of the radial head and annular ligament reconstruction in the setting of achronic Monteggia fracture-dislocation is attributed to Bell Tawse. 2 This technique for radiocapitellar reduction in chronic Monteggia lesions employed the Boyd approach and reconstructed the annular ligament by turning down a strip of triceps fascia.Our overall approach for surgical treatment of chronic Monteggia lesions includes an open osteotomy of the ulna with plate fixation, open reduction of radiocapitellar joint, and repair or reconstruction of the annular ligament.To avoid potential complications of posterior interosseous nerve injury and compartment syndrome, the reconstruction is performed via an extensile posterior approach that permits identification and protection of the posterior interosseous nerve and prophylactic forearm fasciotomies.There are surgeons who advocate extra-articular osteotomy of the ulna alone, including use of external or intramedullary fixation of the ulna.
PREOPERATIVE PLANNING
The morphology of the radial head and capitellum should be evaluated on plain radiographs and, if necessary, on MRI to define the concavity of the radial head and the reducibility of the proximal radioulnar joint and radiocapitellar joints. A normal concave radial head articular surface and normal convex capitellar articular surface are requirements for reconstruction. Three-dimensional imaging in children with radial head dislocation more than 3 years from injury can reveal flattening of the radial head and even development of a dome-shapeddeformity. 18 Corresponding flattening of the lesser sigmoid notch can also be observed.18Preoperative elbow flexion-extension and forearm supination-pronation should be measured and recorded.
POSITIONING
General anesthesia is preferred over a regional block to allow postoperative assessment of peripheral nervefunction and compartment syndrome.The patient is placed in a supine position on the operating table with the elbow, forearm, and hand outstretched onto a hand table. The entire upper limb including the axilla should be included in the surgical field.A sterile pneumatic tourniquet is employed to maximize access to the upper arm, which is required for the extensile surgical approach.
APPROACH
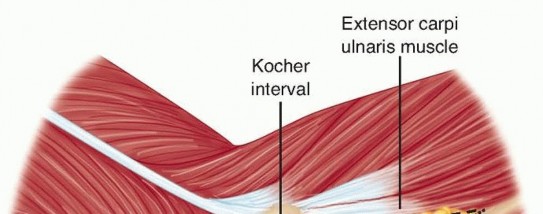
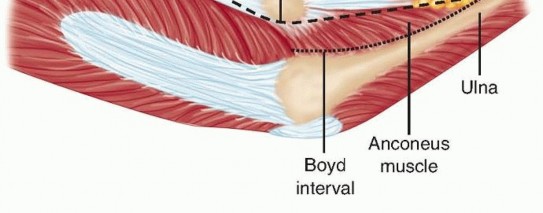
FIG 9 • Surgical intervals for the Boyd approach and the Kocher approach.
TECHNIQUES
EXTENSILE POSTEROLATERAL APPROACH

TECH FIG 1 • Surgical exposure for reconstruction of a chronic Monteggia lesion. A. A curvilinear posterolateral approach to the elbow is planned. The proximal and distal extent of the incision is used as necessary. B. The posterior interosseous nerve should be identified at its bifurcation from the radial nerve and traced distally. The posterior interosseous nerve should be carefully dissected off of the anterior elbow capsule to avoid iatrogenic injury during radiocapitellar reduction. C. The interval between the anconeus and the extensor carpi ulnaris is used to access the radiocapitellar joint. (© COSF, Boston. From Flynn J, ed.


TECH FIG 2 • The dislocated radial head and the collapsed annular ligament are identified. (© COSF, Boston. From Flynn J, ed. Pediatric Hand and Upper Limb Surgery. Philadelphia: Lippincott Williams & Wilkins, 2012.)
ULNAR OSTEOTOMY


TECH FIG 3 • Ulnar osteotomy. A. An osteotomy of the ulna is performed at the apex of the malunion using an oscillating saw. B. The ulnar osteotomy is stabilized with appropriately contoured plate and screw fixation. In younger children, double-stacked one-third tubular plates are employed as illustrated in this case. C. Four to six cortices of fixation should be obtained on either side of the ulnar osteotomy.
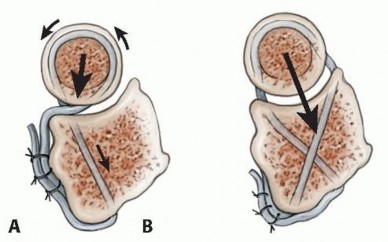
TECH FIG 4 • Schematic representation of annular ligament reconstruction techniques. A. The Bell Tawse reconstruction which results in a posteriorly directed force. 2 B. The technique suggested by Seel and Peterson. In this technique, crossing drill holes are created at the anterior and posterior rim of the lessersigmoid notch. The resulting reconstruction may improve stability of the radial head. 22 (Adapted from Seel MJ, Peterson HA. Management of chronic posttraumatic radial head dislocation in children. J Pediatr Orthop 1999;19:306-312.)P.1014. Prophylactic Forearm FasciotomiesUnder direct visualization, limited prophylactic fasciotomies of the volar and dorsal compartments are performed to minimize risk of postoperative compartment syndrome.Prophylactic fasciotomies have the secondary advantage of facilitating periosteal closure.5. Final Evaluation of Reduction and Wound ClosureFinal orthogonal fluoroscopy images should be obtained to verify stable reduction of the radiocapitellar and proximal radioulnar joints.Continued wire fixation of the radiocapitellar joint is rarely needed if the ulnar osteotomy and annular ligament repair/reconstruction are performed correctly.In our experience, this has been occasionally necessary in revision reconstruction of a chronic Monteggia lesion where reconstructive options are more limited.In this case, a wire of sufficient size is mandatory to avoid fatigue and breakage. As always, a smooth wire should be used to avoid physeal injury. The wire is typically removed 3 to 4 weeks postoperatively.Following radiocapitellar reduction, annular ligament repair or reconstruction, and ulnar osteotomy, a layered wound closure is performed. The periosteum overlying the ulna is repaired to expedite bone healing.The capsule is repaired and the extensor-supinator origin is reattached to the lateral epicondyle and lateral supracondylar ridge of the humerus. Intermuscular intervals are reapproximated, and the wound is closed over a Jackson-Pratt drain.PEARLS AND PITFALLS
|Distinguish ▪ Hypoplasia of the capitellum and convex deformity of the radial head is indicative congenital and of a congenital radial head dislocation.traumatic dislocation of the radial headAvoidance of ▪ Avoid preoperative regional block to monitor the child following reconstruction. compartment ▪ Prophylactic volar and dorsal forearm fasciotomies can be performed to minimize syndrome risk of postoperative compartment syndrome.1.Wounds should be closed over a drain if there is a concern for hemostasis.Protection of ▪ When planning an intra-articular reconstruction of a long-standing lesion or in the posterior the presence of a preoperative radial neuropathy, the radial nerve should be interosseous identified in the brachioradialis-brachialis interval and then followed distally as it nerve branches into the superficial radial nerve and the posterior interosseous nerve.||1.The posterior interosseous nerve can be adherent to the joint capsule and displaced radial head or incarcerated at the radiocapitellar joint. Careful identification and protection of the posterior interosseous nerve during surgical exposure can help avoid iatrogenic injury during the reconstruction.Late ▪ Combined annular ligament reconstruction and ulnar osteotomy is advocated. subluxation of ▪ After completion of the ulnar osteotomy, setting the radiocapitellar alignment first the radial is helpful as this determines the amount of ulnar correction needed to maintain a head stable reduction.2.Overcorrection of the ulna is often required for stable reduction of the radial head.3.Carefully scrutinize the reduction with intraoperative fluoroscopy, and do not accept subtle malalignment.4.Serial radiographs should be obtained 2-6 weeks after surgical intervention in order to detect unexpected loss of reduction early.Ulnar ▪ If an oscillating saw is used for the osteotomy, copious irrigation should be nonunion employed to minimize thermal necrosis.5.Plate fixation is mandatory to avoid loss of fixation.6.Fracture callous and periosteal bone at the site of the malunion can be used as local bone graft after completion of the osteotomy.7.If needed, allograft bone is added to the osteotomy site.|------
POSTOPERATIVE CARE
P.102Following wound closure, a bivalved long-arm cast is applied, typically with the elbow in 80 to 90 degrees of flexion and the forearm in 60 to 90 degrees of supination to maximize stability of the radiocapitellar and proximal radioulnar joints.All children should be admitted overnight for pain control and neurovascular monitoring.Casting is discontinued 4 to 6 weeks after surgical reconstruction and children are transitioned to a protective long-arm splint for an additional 3 to 4 weeks. Splint removal for active motion, particularly forearm rotation, is important. Formal rehabilitation is initiated and maximal recovery is anticipated at 6 months. Elbow flexion and extension return more rapidly than forearm rotation.
OUTCOMES
Data on outcomes following reconstruction of chronic Monteggia lesions is limited to small, retrospective case series. Most reports lack long-term follow-up and fail to report validated functional outcome measures.Nakamura et al 17 reported long-term clinical and radiographic outcomes in 22 children that underwent combined ulnar osteotomy and annular ligament reconstruction, at an average follow-up of 84 months.The radial head remained stable in nearly 80% of patients and was subluxated (but not frankly dislocated) in approximately 20% of patients, which is representative of other results reported in the literature. 8,12,21,23Postoperative functional outcomes (Mayo Elbow Performance Index) reliably improved, with the vastmajority of patients experiencing excellent (19 of 22) or good (2 of 22) results.Average elbow flexion improved from 124 to 138 degrees. Average postoperative forearm pronation exceeded 65 degrees. Improvement in elbow motion is reliable and similar results have been described by other investigators. Loss of some forearm rotation, particularly pronation, can beexpected. 8,12,13,21,23The complication rate for chronic Monteggia reconstruction is high and includes late radial head subluxation, notching of the radial neck, osteoarthritis, delayed ulnar union, ulnar nonunion, compartment syndrome, peripheral nerve injury, and stiffness, amongst others. 17,21Good results can more reliably be obtained in children younger than 12 years of age or within 3 years of injury. 17
COMPLICATIONS
Restricted elbow or forearm motion, particularly pronationPostoperative compartment syndrome can occur. Routine perioperative neurovascular monitoring is recommended for early detection. Pain out of proportion to examination or increasing narcotic requirements represent early signs of compartment syndrome and should prompt immediate evaluation. Prophylactic intraoperative forearm fasciotomies are advocated to lessen the risk.Posterior interosseous nerve palsy can occur following reconstruction. If the nerve was identified and protected during surgery, expectant management is recommended. Serial clinical examination will demonstrate an advancing Tinel sign and progressive return of motor function. Failure of recognizable clinical recovery by 6 months is a relative indication for surgical exploration.Ulnar nerve palsy can occur with extensive lengthening of the ulna and may be an indication for decompression.Recurrent subluxation or dislocation of the radial head does occur and negates the original purpose for surgical reconstruction. This is not an operation for the uninitiated.Notching of the radial neck if the annular ligament reconstruction is too taut. 17Ulnar nonunion can occur. An incomplete hinged osteotomy, supplemental bone grafting, stable fixation, and periosteal repair lessen the risk.
REFERENCES
- Bado JL. The Monteggia lesion. Clin Orthop Relat Res 1967;50: 71-86.
- Bell Tawse AJ. The treatment of malunited anterior Monteggia fractures in children. J Bone Joint Surg Br 1965;47:718-723.
- Chen WS. Late neuropathy in chronic dislocation of the radial head. Report of two cases. Acta Orthop Scand 1992;63:343-344.
- Dormans JP, Rang M. The problem of Monteggia fracture-dislocations in children. Orthop Clin North Am 1990;21:251-256.
- Exner GU. Missed chronic anterior Monteggia lesion. Closed reduction by gradual lengthening and angulation of the ulna. J Bone Joint Surg Br 2001;83:547-550.
- Fahey JJ. Fractures of the elbow in children. Instr Course Lect 1960;17:13-46.
- Golden DW, Jhee JT, Gilpin SP, et al. Elbow range of motion and clinical carrying angle in a healthy pediatric population. J Pediatr Orthop B 2007;16:144-149.
- Gyr BM, Stevens PM, Smith JT. Chronic Monteggia fractures in children: outcome after treatment with the Bell-Tawse procedure. J Pediatr Orthop B 2004;13:402-406.
- Hasler CC, Von Laer L, Hell AK. Open reduction, ulnar osteotomy and external fixation for chronic anterior dislocation of the head of the radius. J Bone Joint Surg Br 2005;87:88-94.
- Hirayama T, Takemitsu Y, Yagihara K, et al. Operation for chronic dislocation of the radial head in children. Reduction by osteotomy of the ulna. J Bone Joint Surg Br 1987;69:639-642.
- Holst-Nielsen F, Jensen V. Tardy posterior interosseous nerve palsy as a result of an unreduced radial head dislocation in Monteggia fractures: a report of two cases. J Hand Surg Am 1984;9:572-575.
- Horii E, Nakamura R, Koh S, et al. Surgical treatment for chronic radial head dislocation. J Bone Joint Surg Am 2002;84-A(7):1183-1188.
- Hui JH, Sulaiman AR, Lee HC, et al. Open reduction and annular ligament reconstruction with fascia of the forearm in chronic monteggia lesions in children. J Pediatr Orthop 2005;25:501-506.
- Inoue G, Shionoya K. Corrective ulnar osteotomy for malunited anterior Monteggia lesions in children. 12 patients followed for 1-12 years. Acta Orthop Scand 1998;69:73-76.
- Kunkel S, Cornwall R, Little K, et al. Limitations of the radiocapitellar line for assessment of pediatric elbow radiographs. J Pediatr Orthop 2011;31:628-632.
- Martin BF. The annular ligament of the superior radio-ulnar joint. J Anat 1958;92:473-482.
- Nakamura K, Hirachi K, Uchiyama S, et al. Long-term clinical and radiographic outcomes after open reduction for missed Monteggia fracture-dislocations in children. J Bone Joint Surg Am 2009;91: 1394-1404.
- Oka K, Murase T, Moritomo H, et al. Morphologic evaluation of chronic radial head dislocation: three-dimensional and quantitative analyses. Clin Orthop Relat Res 2010;468:2410-2418.
- Ramski DE, Hennrikus WP, Bae DS, et al. Pediatric Monteggia fractures: a multicenter examination of treatment strategy and early clinical and radiographic results. J Pediatr Orthop 2015;35(2):115-120.
- Ring D, Waters PM. Operative fixation of Monteggia fractures in children. J Bone Joint Surg Br 1996;78:734-739.P.103
- Rodgers WB, Waters PM, Hall JE. Chronic Monteggia lesions in children. Complications and results of reconstruction. J Bone Joint Surg Am 1996;78:1322-1329.
- Seel MJ, Peterson HA. Management of chronic posttraumatic radial head dislocation in children. J Pediatr Orthop 1999;19:306-312.
- Song KS, Ramnani K, Bae KC, et al. Indirect reduction of the radial head in children with chronic Monteggia lesions. J Orthop Trauma 2012;26:597-601.
- Spinner M, Kaplan EB. The quadrate ligament of the elbow—its relationship to the stability of the proximal radio-ulnar joint. Acta Orthop Scand 1970;41:632-647.
- Stoll TM, Willis RB, Paterson DC. Treatment of the missed Monteggia fracture in the child. J Bone Joint Surg Br 1992;74:436-440.
- Tompkins DG. The anterior Monteggia fracture: observations on etiology and treatment. J Bone Joint Surg Am 1971;53: 1109-1114.
- Tubbs RS, O'Neil JT Jr, Key CD, et al. The oblique cord of the forearm in man. Clin Anat 2007;20:411-415.
- Wang MN, Chang WN. Chronic posttraumatic anterior dislocation of the radial head in children: thirteen cases treated by open reduction, ulnar osteotomy, and annular ligament reconstruction through a Boyd incision. J Orthop Trauma 2006;20:1-5.
