Radial Head Replacement
DEFINITION
Radial head fractures are the most common fracture of the elbow and usually can be managed either nonoperatively or with open reduction and internal fixation (ORIF). 12Radial head arthroplasty is indicated for unreconstructable displaced radial head fractures with an associated elbow dislocation or a known or possible disruption of the medial collateral, lateral collateral, or interosseous ligaments. 26Most comminuted radial head fractures have an associated ligament injury, so radial head excision without replacement is uncommonly indicated in the setting of an acute radial head fracture.Biomechanical studies have shown that the kinematics and stability of the elbow are altered by radial head excision, even in the setting of intact collateral ligaments, 24 and are improved with a metallic radial head arthroplasty.6,31,39Radial head replacement is also indicated to treat posttraumatic conditions such as radial head nonunion and malunion and to manage elbow or forearm instability after radial head excision. 41
ANATOMY
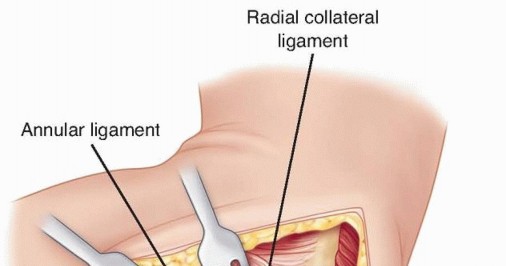
The radial head has a circular concave dish that articulates with the spherical capitellum and an articular margin that articulates with the lesser sigmoid notch of the ulna.The articular dish has an elliptical shape that varies considerably in size and shape and is variably offset from the axis of the radial neck. 44There is a poor correlation between the size of the radial head and the medullary canal of the radial neck, making a modular implant desirable for an optimal fit. 30Elbow stability is maintained by joint congruity, capsuloligamentous integrity, and an intact balanced musculature.The radial head is an important valgus stabilizer of the elbow, particularly in the setting of an incompetent medial collateral ligament, which is the primary stabilizer against valgus force.The radial head is also important as an axial stabilizer of the forearm and resists varus and posterolateral rotatory instability by tensioning the lateral collateral ligament. 25The lateral ulnar collateral ligament is an important stabilizer against varus and posterolateral rotational instability of the elbow 37 and should be preserved or repaired after radial head arthroplasty (FIG 1).The radial head accounts for up to 60% of the load transfer across the elbow. 19
PATHOGENESIS
Displaced radial head fractures typically result from a fall on the outstretched arm.Axial, valgus, and posterolateral rotational patterns of loading are all thought to be potentially responsible for these fractures.Injuries of the medial collateral or lateral collateral ligament or the interosseous ligament are typically associated with comminuted displaced unreconstructable radial head fractures. 9In more severe injuries, dislocations of the elbow and forearm and fractures of the coronoid, olecranon, and capitellum can occur and further impair stability.
NATURAL HISTORY
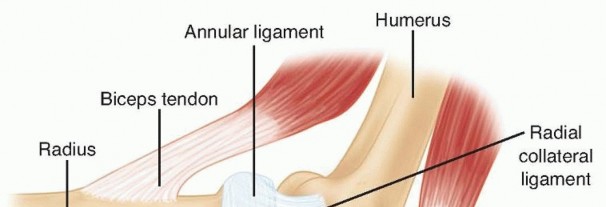
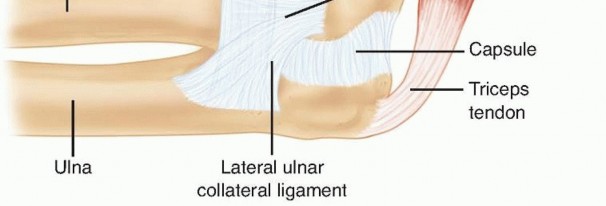
FIG 1 • The ligaments on the lateral aspect of the elbow include the lateral ulnar collateral ligament, the radial collateral ligament, and the annular ligament. The lateral ulnar collateral ligament is an important stabilizer against varus and posterolateral rotational instability of the elbow and should be preserved or repaired after radial head arthroplasty. P.175Metallic radial head replacement in elbows with intact ligaments restores the kinematics and stability similar to that of a native radial head and has been shown to provide good clinical and radiographic outcome in mostpatients at medium-term follow-up; however, long-term outcome studies are lacking. 6
PATIENT HISTORY AND PHYSICAL FINDINGS
The mechanism of injury is typically a fall on the outstretched hand.The patient will complain of pain and limitation of elbow or forearm motion. A history of forearm or wrist pain should be sought.Inspection may reveal ecchymosis along the forearm or medial aspect of the elbow. Deformity may be evident if there is an associated dislocation.Careful palpation of the radial head, the medial and lateral collateral ligaments of the elbow, the interosseous ligament of the forearm, and the distal radioulnar joint should be performed. Local tenderness over one or all of these structures implies a possible derangement of the relevant structure.Because associated injuries of the shoulder, forearm, wrist, and hand are common, these areas should be carefully examined.Range of motion, including forearm rotation and elbow flexion-extension, should be evaluated. The presence of palpable and auditory crepitus should be noted.Loss of terminal elbow flexion and extension is expected as a consequence of a hemarthrosis in acute fractures, whereas loss of forearm rotation typically is caused by a mechanical impingement.A careful neurovascular assessment of all three major nerves that cross the elbow should be performed.The examiner should observe for localized or diffuse swelling in the elbow. Effusion represents hemarthrosis due to intra-articular fracture.The examiner should compare active and passive range of motion to the uninjured side. Reduced range of motion may be a result of hemarthrosis or mechanical block from a broken fragment. Intra-articular injection of a local anesthetic helps differentiate between reduced range of motion due to a mechanical block versus pain inhibition.The examiner should look for varus-valgus instability. Any gapping on the medial or lateral side beneath the examiner's hand is noted. Positive findings suggest medial or lateral collateral ligament insufficiency. Typically, this test is positive only when performed under a regional or general anesthetic, hence these injuries are easy to miss if an examination under anesthesia is not performed.The lateral pivot shift test is performed. Positive apprehension or a clunk that is seen or felt when the ulna and radius reduce on the humerus suggests posterolateral rotatory instability.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Anteroposterior (AP), lateral, and oblique elbow radiographs, with the x-ray beam centered on the radiocapitellar joint, usually provide sufficient information for the diagnosis and treatment of radial head fractures.Bilateral posteroanterior radiographs of both wrists in neutral rotation should be performed to evaluate ulnar variance in patients with wrist discomfort or a comminuted radial head fracture because there is a higherincidence of an associated interosseous ligament injury in these patients. 9Computed tomography with sagittal, coronal, and three-dimensional (3-D) reconstructions may assist with preoperative planning and can help the surgeon predict whether a displaced radial head fracture can be repaired with ORIF or if an arthroplasty will likely be needed.
DIFFERENTIAL DIAGNOSIS
Acute radial head fracturesOther fractures or dislocations about the elbow (eg, supracondylar, capitellar, coronoid, osteochondral fractures)Radial head nonunion or malunion, posttraumatic arthritis Congenital dislocation of the radial headForearm or elbow instability Lateral epicondylitisRheumatoid arthritis or osteoarthritis Synovitis, inflammatory or infectious Tumors
NONOPERATIVE MANAGEMENT
The indications for surgical management of radial head fractures are not well defined in the literature. Fragment size, number of fracture fragments, degree of displacement, and bone quality influence decision making regarding the optimal management.Nondisplaced fractures or small ( <33% of the radial head) minimally displaced fractures (<2 mm of displacement) can be treated with early motion with an excellent outcome in the majority of patients.21Associated injuries and a block to motion are also important factors to consider when deciding between nonoperative and surgical management.
SURGICAL MANAGEMENT
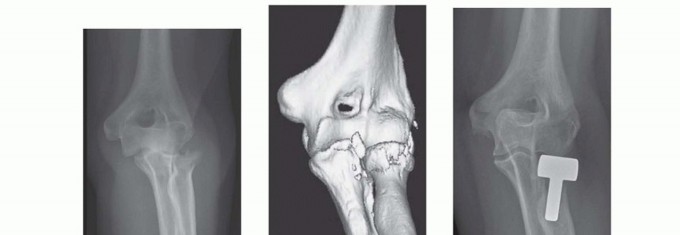
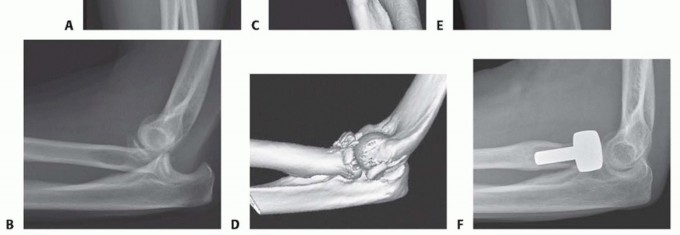
FIG 2 • A,B. AP and lateral radiographs of a 54-year-old woman who sustained a posterolateral elbow dislocation associated with a comminuted fracture of the radial head and coronoid—the “terrible triad.” C,D. Preoperative 3-D reconstruction images demonstrating a comminuted radial head fracture with a small undisplaced coronoid fracture. E,F. Postoperative radiographs after modular radial head arthroplasty (Evolve, Wright Medical Technology, Arlington, TN) and repair of the lateral collateral ligament. Medial collateral ligament and coronoid repairs were not required because the elbow was sufficiently stable at the end of the procedure. A good functional outcome was achieved at the final follow-up.
PREOPERATIVE PLANNING
Currently available devices include smooth stem spacer implants, press-fit ingrowth stems, monoblock and bipolar devices, and metallic or pyrolytic carbon articulations.Most implants have an axisymmetric circular design; however, one currently available device has a more anatomic nonaxisymmetric elliptical shape. 33,40,47Silicone radial head implants offer little in the way of axial or valgus stability to the elbow and have been complicated by a high incidence of implant wear, fragmentation, and silicone synovitis leading to generalizedjoint damage. As a result, they have fallen out of favor and have been replaced by metallic implants. 18Most metallic radial head implants that are currently available are modular with separate heads and stems, allowing improved size matching of the native radial head and neck relative to older monoblock designs. 17,28,30Precise implant sizing and placement are critical with these devices to ensure correct capitellar tracking and to avoid a cam effect with forearm rotation, which may cause premature capitellar wear due to shearing of thecartilage and stem loosening due to increased loading of the stem-bone interface. 15Preoperative radiographic templating of the contralateral normal radial head should be employed in the setting of a secondary radial head replacement but is not needed for acute fractures because the excised radial head is available for accurate implant sizing.
POSITIONING

TECHNIQUES
SURGICAL APPROACH
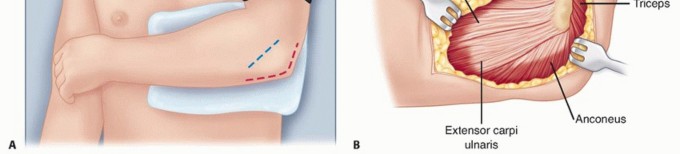
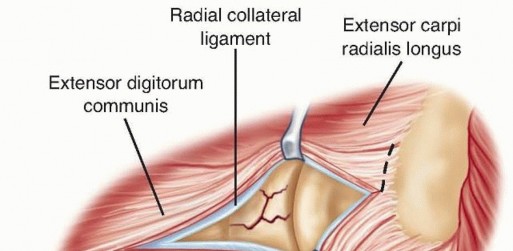
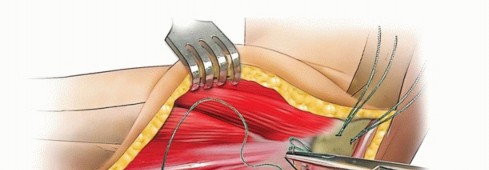
COMMON EXTENSOR SPLIT
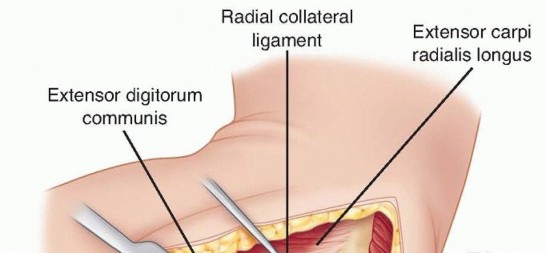
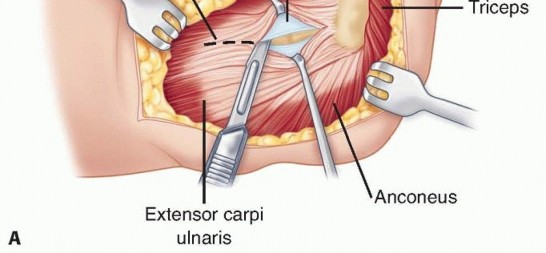
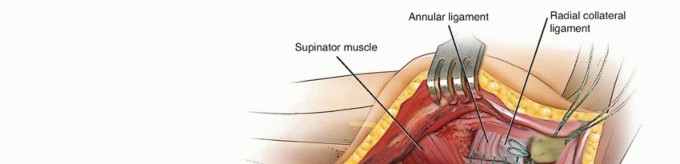
TECH FIG 2 • A. The common extensor tendon is split longitudinally at the middle aspect of the radial head, and the underlying radial collateral and annular ligaments are incised. The forearm is pronated to protect the posterior interosseous nerve.(continued)
TECH FIG 2 •(continued)B. The humeral origin of the radial collateral ligament and the overlying extensor muscles are elevated anteriorly off the lateral epicondyle to improve the exposure if needed.
Preparation of the Radial Head and Neck

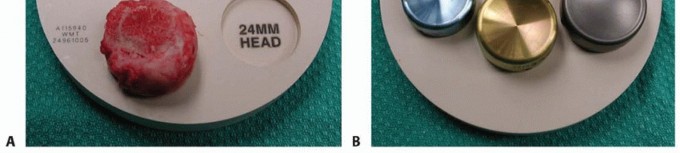
TECH FIG 3 • The resected radial head is reassembled in the provided sizing template (A) to assist in the accurate sizing of the prosthesis in terms of diameter (B) and height (C) and to ensure that all the fragments have been removed from the elbow.(continued)
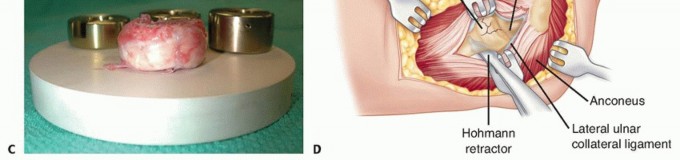
TECH FIG 3 •(continued)D. The radial neck is delivered laterally using a Hohmann retractor carefully placed around the posterior aspect of the proximal radial neck. An anteriorly based retractor should be avoided because of the risk of injury to the posterior interosseous nerve.
RADIAL HEAD REPLACEMENT
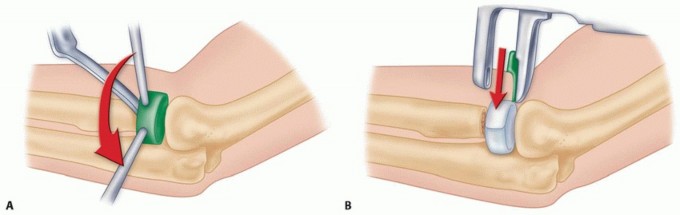
TECH FIG 4 • A. A trial stem is inserted. A trial head is inserted onto the stem and the diameter, height, tracking, and congruency of the prosthesis are evaluated both visually and with the aid of an image intensifier. B. Some modular and bipolar implants allow insertion of the stem first, then placement of the head onto the stem with coupling in situ, which significantly reduces the surgical exposure needed.

TECH FIG 5 •(continued)D. A second stitch is used in a similar manner to repair the common extensor muscle fascia. E. The sutures are pulled into the holes drilled in the distal humerus using suture retrievers, tensioned while keeping the forearm pronated and while avoiding varus forces, and eventually tied over the lateral supracondylar ridge.
COMPLETION
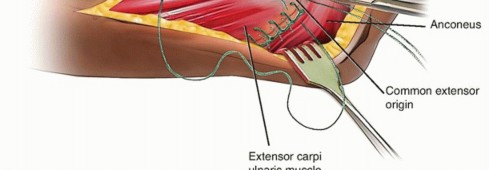
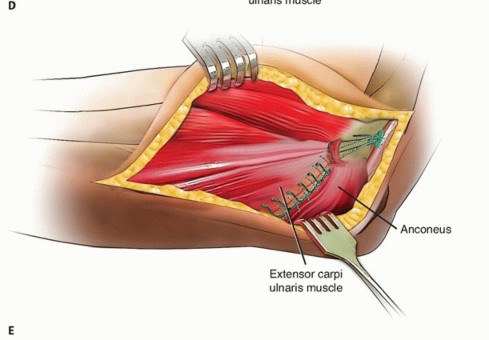
KOCHER APPROACH
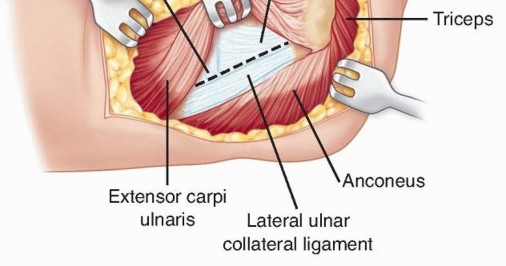
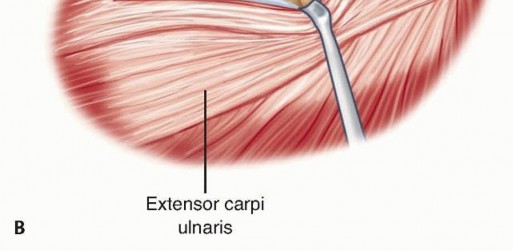
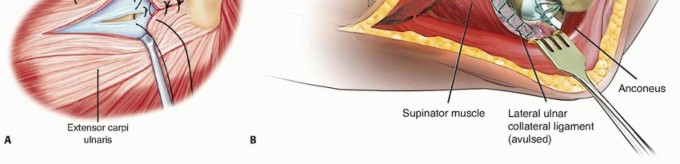
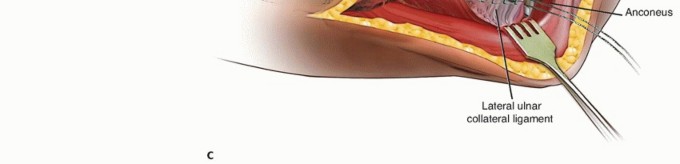
TECH FIG 6 • The extensor carpi ulnaris is elevated anteriorly, and an arthrotomy is performed at the midportion of the radial head. Care should be taken to preserve the lateral ulnar collateral ligament, which is vulnerable as the dissection is carried deeper through the capsule.
PEARLS AND PITFALLS
|Indications ▪ Displaced unreconstructable fracture of the radial head with known or probable associated medial or lateral collateral or interosseous ligament injuryPearls ▪ A preoperative radiographic template of the contralateral native radial head should be used in the setting of a secondary radial head replacement.|1.Dissection should stay anterior to the lateral ulnar collateral ligament to prevent the development of posterolateral rotatory instability.2.The radial head should be sized based on the minor diameter and thickness of the excised radial head.3.The radial head implant is typically 2 mm smaller than the major diameter of the native elliptical radial head.4.Radial head articular surface height should be at the level of the proximal radioulnar joint.5.If the radial head does not track well on the capitellum, the stem should be downsized.6.If the native radial head is in between implant sizes, the implant should, in general, be downsized.7.Intraoperative fluoroscopy is used to assess the alignment of the radiocapitellar and distal radioulnar joints and to avoid overlengthening of the radius.Pitfalls ▪ Hohmann retractors should not be used around the anterior aspect of the radial neck, and the forearm should be kept pronated to avoid damage to the posterior interosseous nerve.8.The surgeon should avoid overstuffing the thickness or diameter of the radial head because of the risk of capitellar wear and pain. Filling the gap between the capitellum and radial neck is not a useful landmark for prosthesis thickness because lateral soft tissues are often deficient owing to the surgical exposure or initial injury.
POSTOPERATIVE CARE
The elbow with stable ligaments should be splinted using anterior plaster slabs in extension and elevated for 24 to 48 hours to diminish swelling, decrease tension on the posterior wound, and minimize the tendency to develop a flexion contracture.In the setting of a more tenuous ligamentous repair or the presence of some residual instability at the end of the operative procedure, the elbow should initially be splinted in 60 to 90 degrees of flexion in the optimal position of forearm rotation to maintain stability.Perioperative antibiotics are continued for 24 hours postoperatively.Indomethacin 25 mg three times daily for 3 weeks may be considered in patients undergoing radial head arthroplasty to decrease postoperative pain, reduce swelling, and potentially lower the incidence of heterotopic ossification.Indomethacin should be avoided in elderly patients and those with a history of peptic ulcer disease, asthma, known allergy, or other contraindications to anti-inflammatory medications.For an isolated radial head replacement treated with a lateral ulnar collateral ligament-sparing approach, active range of motion should be initiated on the day after surgery.A collar and cuff with the elbow maintained at 90 degrees is employed for comfort between exercises.A static progressive extension splint is fabricated for nighttime use for patients without associated ligamentous disruptions and is employed for a period of 12 weeks. The splint is adjusted weekly as extension improves.P.183In patients with associated elbow dislocations or residual instability, extension splinting is not implemented until 6 weeks after surgery.Patients with associated fractures, dislocations, or ligamentous injuries should commence active flexion and extension motion within a safe arc 1 day postoperatively.Active forearm rotation is performed with the elbow in flexion to minimize stress on the medial or lateral ligamentous injuries or repairs.Extension is performed with the forearm in the appropriate rotational position—that is, pronation if the lateralligaments are deficient, 13 supination if the medial ligaments are deficient,2 and neutral position if both sides have been injured.A resting splint with the elbow maintained at 90 degrees and the forearm in the appropriate position of forearm rotation is employed for 3 to 6 weeks.Passive stretching is not permitted for 6 weeks to reduce the incidence of heterotopic ossification.Strengthening exercises are initiated once the ligament injuries and any associated fractures have adequately healed, usually at 8 weeks postoperatively.
OUTCOMES
Silicone radial head arthroplasty, although initially successful in many patients, 8,42 has fallen out of favor because of problems with residual instability and arthritis, implant fracture, and silicone synovitis due to particulate debris.45Although the short- and medium-term results of metallic radial head implants are encouraging, there is a paucity of literature demonstrating the long-term outcome with respect to loosening, capitellar wear, and arthritis. 14,17Metallic radial head replacement in elbows with intact ligaments restores the kinematics and stability similar to that measured with a native radial head. Moreover, when the fractured radial head occurs in combination with ligamentous and soft tissue disruption, a metallic prosthesis restores elbow stability, with only mild residual deficits in strength and motion.Results appear to be better if surgery is performed early ( <10 days from injury).3,34Moro et al 36 reported the functional outcome of 25 cases managed with a metallic radial head arthroplasty for unreconstructable fractures of the radial head at an average follow-up of 39 months. The results were rated as 17 good or excellent, 5 fair, and 3 poor.The radial head prosthesis restored elbow stability when the fractured radial head occurred in combination with a dislocation of the elbow, rupture of the medial collateral ligament, fracture of the coronoid, or fracture of the proximal ulna.There were mild residual deficits in strength and motion, and no patient required removal of the implant.Grewal et al 17 reported high satisfaction rate among 26 patients, 2 years following a modular, monopolar radial head arthroplasty with a loose press-fit stem for unreconstructable radial head fractures.Zunkiewicz et al 47 reported good functional outcome in 29 patients managed with a bipolar radial head prosthesis with a smooth unfixed telescoping stem with an average follow-up of 34 months. Theprosthesis effectively restored stability and joint congruency to elbows with comminuted radial headfractures and valgus instability.Flinkkilä et al 15 reported high failure rate and early loosening of press-fit radial head implants which were used in acute unstable elbow injuries, 12 of 37 press-fit stems were radiographically loose at a mean follow-up of 11 months, with 9 of them necessitating implant removal.Harrington et al 20 reported their experience with metallic radial head arthroplasty in 20 patients at an average follow-up of 12 years. The results were excellent or good in 16 and fair or poor in 4.Improvements in radial head arthroplasty designs, sizing, and implantation techniques may lead to improved outcomes for unreconstructable radial head fractures.
COMPLICATIONS
Posterior interosseous nerve injury can occur as a consequence of dissection distal to the radial tuberosity and placement of anterior retractors around the distal radial neck.InfectionLoss of motion, mainly terminal extension due to capsular contracture, heterotopic ossification, or retained cartilaginous or osseous fragmentsProsthetic loosening, failure or polyethylene wear 15,43 Capitellar wear and pain due to implant overstuffing Complex regional pain syndromeInstability or recurrent dislocations of the elbow due to an inadequate or failed ligament repairOsteoarthritis of the capitellum as a consequence of articular cartilage damage from the initial injury, from component insertion, from persistent instability, or due to loading from a radial head implant that is too thick
REFERENCES
- Antuna SA, Sánchez-Márquez JM, Barco R. Long-term results of radial head resection following isolated radial head fractures in patients younger than forty years old. J Bone Joint Surg Am 2010;92(3):558-566.
- Armstrong AD, Dunning CE, Faber KJ, et al. Rehabilitation of the medial collateral ligament-deficient elbow: an in vitro biomechanical study. J Hand Surg Am 2000;25(6):1051-1057.
- Ashwood N, Bain GI, Unni R. Management of Mason type-III radial head fractures with a titanium prosthesis, ligament repair, and early mobilization. J Bone Joint Surg Am 2004;86-A(2):274-280.
- Athwal GS, Rouleau DM, MacDermid JC, et al. Contralateral elbow radiographs can reliably diagnose radial head implant overlengthening. J Bone Joint Surg Am 2011;93(14):1339-1346.
- Bain GI, Ashwood N, Baird R, et al. Management of Mason type III radial head fractures with a titanium prosthesis, ligament repair, and early mobilization. J Bone Joint Surg Am 2005;87(suppl, 1 pt 1):136-147.
- Beingessner DM, Dunning CE, Gordon KD, et al. The effect of radial head excision and arthroplasty on elbow kinematics and stability. J Bone Joint Surg Am 2004;86-A(8):1730-1739.
- Boulas HJ, Morrey BF. Biomechanical evaluation of the elbow following radial head fracture. Comparison of open reduction and internal fixation versus excision, silastic replacement, and non-operative management. Chir Main 1998;17:314-320.
- Carn RM, Medige J, Curtain D, et al. Silicone rubber replacement of the severely fractured radial head. Clin Orthop Relat Res 1986;(209):259-269.P.184
- Davidson PA, Moseley JB Jr, Tullos HS. Radial head fracture. A potentially complex injury. Clin Orthop Relat Res 1993;(297):224-230.
- Diliberti T, Botte MJ, Abrams RA. Anatomical considerations regarding the posterior interosseous nerve during posterolateral approaches to the proximal part of the radius. J Bone Joint Surg Am 2000;82(6):809-813.
- Dowdy PA, Bain GI, King GJ, et al. The midline posterior elbow incision. An anatomical appraisal. J Bone Joint Surg Br 1995;77(5): 696-699
- Duckworth AD, Clement ND, Jenkins PJ, et al. The epidemiology of radial head and neck fractures. J Hand Surg Am 2012;37(1):112-119.
- Dunning CE, Zarzour ZD, Patterson SD, et al. Muscle forces and pronation stabilize the lateral ligament deficient elbow. Clin Orthop Relat Res 2001;(388):118-124.
- El Sallakh S. Radial head replacement for radial head fractures. J Orthop Trauma 2013;27:e137-e140.
- Flinkkilä T, Kaisto T, Sirniö K, et al. Short- to mid-term results of metallic press-fit radial head arthroplasty in unstable injuries of the elbow. J Bone Joint Surg Br 2012;94(6):805-810.
- Frank SG, Grewal R, Johnson J, et al. Determination of correct implant size in radial head arthroplasty to avoid overlengthening. J Bone Joint Surg Am 2009;91(7):1738-1746.
- Grewal R, MacDermid JC, Faber KJ, et al. Comminuted radial head fractures treated with a modular metallic radial head arthroplasty. Study of outcomes. J Bone Joint Surg Am 2006;88(10):2192-2200.
- Gupta GG, Lucas G, Hahn DL. Biomechanical and computer analysis of radial head prostheses. J Shoulder Elbow Surg 1997;6:37-48.
- Halls AA, Travill A. Transmission of pressures across the elbow joint. Anat Rec 1964;150:243-247.
- Harrington IJ, Sekyi-Otu A, Barrington TW, et al. The functional outcome with metallic radial head implants in the treatment of unstable elbow fractures: a long-term review. J Trauma 2001;50:46-52.
- Herbertsson P, Josefsson PO, Hasserius R, et al. Displaced Mason type I fractures of the radial head and neck in adults: a fifteen- to thirty-three-year follow-up study. J Shoulder Elbow Surg 2005;14:73-77.
- Ikeda M, Oka Y. Function after early radial head resection for fracture: a retrospective evaluation of 15 patients followed for 3-18 years. Acta Orthop Scand 2000;71:191-194.
- Janssen RP, Vegter J. Resection of the radial head after Mason type-III fracture of the elbow: follow-up at 16 to 30 years. J Bone Joint Surg Br 1998;80(2):231-233.
- Jensen SL, Olsen BS, Søjbjerg JO. Elbow joint kinematics after excision of the radial head. J Shoulder Elbow Surg 1999;8:238-241.
- Johnson JA, Beingessner DM, Gordon KD, et al. Kinematics and stability of the fractured and implant-reconstructed radial head. J Shoulder Elbow Surg 2005;14:195S-201S.
- Johnston GW. A follow-up of one hundred cases of fracture of the head of the radius with a review of the literature. Ulster Med J 1962;31: 51-56.
- Karlsson MK, Herbertsson P, Nordqvist A, et al. Long- term outcome of displaced radial neck fractures in adulthood: 16-21 year follow-up of 5 patients treated with radial head excision. Acta Orthop 2009;80:368-370.
- King GJ. Management of radial head fractures with implant arthroplasty. J Am Soc Surg Hand 2004;4:11-26.
- King GJ, Patterson SD. Metallic radial head arthroplasty. Tech Hand Up Extrem Surg 2001;5:196-203.
- King GJ, Zarzour ZD, Patterson SD, et al. An anthropometric study of the radial head: implications in the design of a prosthesis. J Arthroplasty 2001;16:112-116.
- King GJ, Zarzour ZD, Rath DA, et al. Metallic radial head arthroplasty improves valgus stability of the elbow. Clin Orthop Relat Res 1999;(368):114-125.
- Kocher T. Textbook of Operative Surgery. London: Adam and Charles Black, 1911.
- Lamas C, Castellanos J, Proubasta I, et al. Comminuted radial head fractures treated with pyrocarbon prosthetic replacement. Hand 2011;6:27-33.
- Lapner M, King GJ. Radial head fractures. J Bone Joint Surg Am 2013;95(12):1136-1143.
- Lindenhovius AL, Felsch Q, Doornberg JN, et al. Open reduction and internal fixation compared with excision for unstable displaced fractures of the radial head. J Hand Surg Am 2007;32(5):630-636.
- Moro JK, Werier J, MacDermid JC, et al. Arthroplasty with a metal radial head for unreconstructiblefractures of the radial head. J Bone Joint Surg Am 2001;83-A(8):1201-1211.
- Morrey BF, An KN. Articular and ligamentous contributions to the stability of the elbow joint. Am J Sports Med 1983;11:315-319.
- Patterson SD, Bain GI, Mehta JA. Surgical approaches to the elbow. Clin Orthop Relat Res 2000; (370):19-33.
- Pomianowski S, Morrey BF, Neale PG, et al. Contribution of monoblock and bipolar radial head prostheses to valgus stability of the elbow. J Bone Joint Surg Am 2001;83-A(12):1829-1834.
- Sarris IK, Kyrkos MJ, Galanis NN, et al. Radial head replacement with the MoPyC pyrocarbon prosthesis. J Shoulder Elbow Surg 2012;21:1222-1228.
- Shore BJ, Mozzon JB, MacDermid JC, et al. Chronic posttraumatic elbow disorders treated with metallic radial head arthroplasty. J Bone Joint Surg Am 2008;90(2):271-280.
- Swanson AB, Jaeger SH, La Rochelle D. Comminuted fractures of the radial head. The role of silicone-implant replacement arthroplasty. J Bone Joint Surg Am 1981;63(7):1039-1049.
- van Riet RP, Sanchez-Sotelo J, Morrey BF. Failure of metal radial head replacement. J Bone Joint Surg Br 2010;92(5):661-667.
- van Riet RP, Van Glabbeek F, Neale PG, et al. The noncircular shape of the radial head. J Hand Surg Am 2003;28(6):972-978.
- Vanderwilde RS, Morrey BF, Melberg MW, et al. Inflammatory arthritis after failure of silicone rubber replacement of the radial head. J Bone Joint Surg Br 1994;76(1):78-81.
- Zarattini G, Galli S, Marchese M, et al. The surgical treatment of isolated mason type 2 fractures of the radial head in adults: comparison between radial head resection and open reduction and internal fixation. J Orthop Trauma 2012;26:229-235.
- Zunkiewicz MR, Clemente JS, Miller MC, et al. Radial head replacement with a bipolar system: a minimum 2-year follow-up. J Shoulder Elbow Surg 2012;21:98-104.
