DEFINITION
Radial dysplasia represents a spectrum of longitudinal deficiency in radial growth. This deficiency can be mild or severe based on the deficiency in the radius.
ANATOMY
The anatomic relations of the radial aspect of the wrist are altered due to the variable absence of the radius. Table 1 Bayne and Klug Classification of Radial Dysplasia




A consistent but highly abnormal brachiocarpalis muscle has been described in thrombocytopenia-absent radius(TAR) syndrome.14 This muscle spans from just distal to the deltoid insertion directly into the radial side of the carpus and inserts as a broad aponeurotic fan into the carpus, joint capsule, and tendons of the radial wrist.Many patients have associated thumb hypoplasia.10Bayne and Klug2 have provided a classification based on radiographic findings (Table 1).Several authors have proposed alterations to this classification in order to better describe the spectrum ofpresentation. James et al12 added N and 0 categories. N represents patients with a normal radius and carpus but hypoplastic thumb and 0 for patients with carpal abnormalities andnormal radial length. Goldfarb et al9 proposed a type V for more proximal deficiencies.P.1351
PATHOGENESIS
Radial dysplasia develops during the period of embryogenesis. During this period, other organ systems are developing and may also be affected, as discussed later in this chapter.
NATURAL HISTORY
The natural history of patients with radial dysplasia clearly depends on the type of dysplasia present and the associated conditions.Patients with isolated type I or II radial dysplasia usually do not require surgical intervention to address the wrist and radial deformity.Patients with more severe dysplasia can frequently benefit from surgical intervention.Many times radial dysplasia is part of a syndrome, and the associated sequelae clearly affect these patients more than the underlying radial dysplasia. The most common associations are with Holt-Oram syndrome, TAR syndrome, Fanconi anemia, and VACTERL (vertebral anomalies, anal atresia, cardiovascular anomalies,tracheoesophageal fistula, esophageal atresia, renal or radial anomalies, limb anomalies).10,11 An association with several craniofacial syndromes has been well documented.8No matter what procedure is used for treating the radial dysplasia, the patients all have a high incidence ofrecurrent deformity as they get older.2,4,17
PATIENT HISTORY AND PHYSICAL FINDINGS
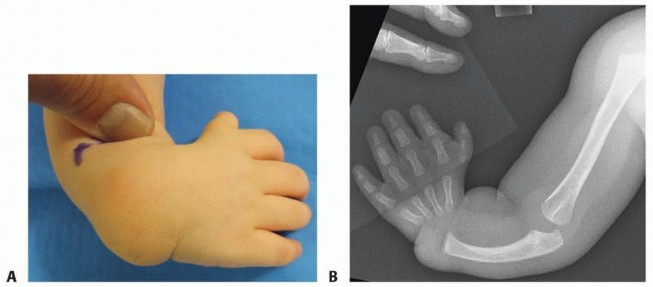
FIG 1 • A. Preoperative photo showing radial deviation of the wrist. B. Anteroposterior (AP) radiograph of the same child demonstrating type IV radial deficiency. Because of its frequent association with systemic conditions, all patients require careful examination of their spine and cardiac, renal, and hematologic systems.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Radiographs should be taken of both forearms to assess stage of radial dysplasia (see Table 1).In addition, all patients warrant a workup for syndromes and associated conditions, such as Holt-Oram syndrome, Fanconi anemia, TAR syndrome, and VACTERL.This may require echocardiogram, renal ultrasound, hematologic studies (complete blood count [CBC] and chromosomal fragility studies), and spinal evaluation.Each treating physician should consider these associations and not assume they have already been worked up, especially if surgical care of the limb is contemplated.
NONOPERATIVE MANAGEMENT
All patients warrant stretching and splinting before consideration of any surgical intervention. The splints should be large enough to be effective and also to minimize any choking hazard.
SURGICAL MANAGEMENT
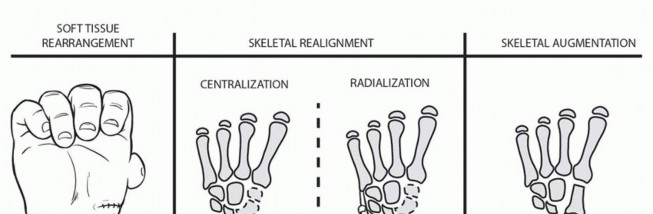
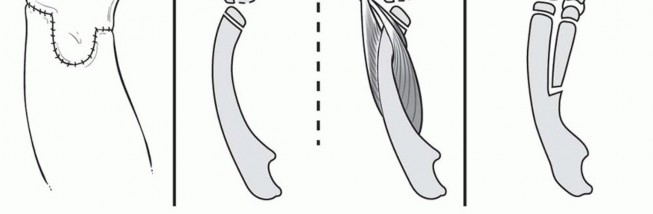
FIG 2 • Surgical options for correction of radial dysplasia. Centralization has been the most common procedure and was first described by Sayre in 1893.15 These procedures bring the carpus in line with the distal ulna and many create a notch to stabilize the carpus in amortise and tenon fashion. Buck-Gramcko3 described radialization, where the carpus is brought across to the ulnar side of the ulna and the extensor carpi radialis (ECR) and flexor carpi radialis (FCR) muscle are transposed. This was proposed to improve balance and limit the recurrence seen after centralization.Ulnar growth disturbance has been found to be increased in patients who have undergone centralization procedures.16Nonvascularized bone transfer has been tried with or without epiphyseal transfer1,18 and largely abandoned due to a lack of ongoing growth leading to recurrent deformity.Vascularized bone transfer can be used in selective cases to provide stabilization of the radial side of thewrist.19 A vascularized second toe metatarsophalangeal (MTP) joint as described by De Jong et al5 and Vilkki20 or proximal fibular transfer, provide structural support to the deficient radial side of the wrist and allow for continued growth with the growth of the child. These potentially limit recurrence while maintaining wrist motion.The long-term problem for any surgical procedure is the recurrence rate.Interventions should aim to minimize risk of further growth abnormality and preserve motion. Total range ofmotion of the fingers and wrist are more important to activity and participation than the angulation at the wrist.6 Preservation of range of motion should be the goal of any selected surgical procedure.We have had experience with various procedures for the treatment of radial dysplasia, including centralization, free toe MTP transfer for stabilization of the radial wrist, and soft tissue release alone. We no longer use formal centralization procedures, as we have found the recurrence rate to be similar to our soft tissue release procedure. In addition, this procedure jeopardizes the ulnar epiphysis, which can lead to an extraordinarily short forearm. Also, loss of mobility results when a centralization procedure is successful.For our patients, soft tissue release with a bilobed flap reconstruction has provided the most reliable, effective results. This maintains motion, improves position, and minimizes injury to the distal ulnar physis. This does not preclude vascularized free joint transfer or other procedures at a subsequent juncture.
PREOPERATIVE PLANNING
Timing of surgery. Younger patients have the most to gain from soft tissue release with bilobed flap. Our preference is to perform this procedure between 12 months and 2 years of age; however, older patients will also benefit.May be combined with other indicated surgical procedures, including flexor digitorum superficialis (FDS) opponensplastyWe prefer to perform pollicization or thumb reconstructive procedures for associated types IIIB to V thumb hypoplasia in a staged manner.Others have combined centralization procedures with bilobed flaps. Radiographs are performed to confirm clinical findings (see FIG 1B).Clearance of associated comorbidities—appropriate consultation or investigation in particular to exclude cardiacand hematologic abnormalities that may influence safety of anesthesia and surgical complications. Before surgery, the patient must have undergone adequate soft tissue stretching.In the first few months, this is accomplished by splinting. In severe cases, serial casting may be necessary.P.1353After about 6 months of age, active stretching is started by the parents with use of nighttime splinting.External fixator-assisted soft tissue distraction is reserved for the most severe cases and, in our experience, is uncommonly indicated prior to a bilobed flap; it may be beneficial in older children.
POSITIONING
The patient is placed in the standard supine position, and a general anesthetic is used in all cases.We do not use a standard tourniquet, as we have found this to be inadequate in young children. Instead, we use the elastic Esmarch bandage as a tourniquet on the upper arm.
TECHNIQUE
APPROACH
VOLAR BILOBED FLAP
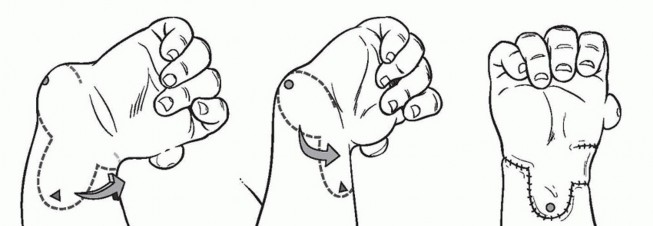
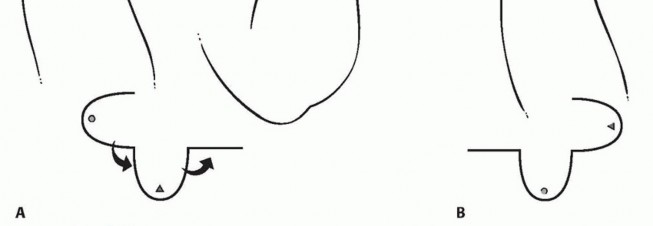
TECH FIG 1 • A. Flap design. B. Flap rotation and final positioning.(continued)

TECH FIG 1 •(continued)C-E. Markings for bilobed flap.
Release of the Radial Deviation of the Wrist



TECH FIG 2 • A. After release of radial tethering tissue, protection of finger flexors, extensors, and neurovascular structures. B. Rotation of flaps. C,D. Skin is sutured. E. Dorsal view with protective pin. Care must be taken not to dissect excessively near the ulnar epiphysis to prevent injury to the vascular supply to this area.After release is accomplished, the wrist is placed in a neutral position and pinned with a 0.062-inch Kirschner wire.The Kirschner wire is temporary and is put across the joint from either direction (ie, there is no specific location for the exit or entrance site). Our preferred trajectory is one which avoids crossing the ulnar physis.The flaps are then rotated and sutured in place (TECH FIG 2B-E).The tourniquet is removed to ensure perfusion to the fingers, and a long-arm cast is placed.P.1355
PEARLS AND PITFALLS
POSTOPERATIVE CARE
The long-arm cast is left on for 3 to 4 weeks.At that point, the pin is removed and the patient is changed to a removable splint.
OUTCOMES


FIG 3 • Postoperative results. A. Early healing and resting wrist position. B. Volar bilobed flap, post staged pollicization procedure. C. Functional positioning post pollicization.
COMPLICATIONS
Few complications are associated with this procedure.Partial flap loss can occur, but the risk seems to be minimized by appropriate flap design, transfixion with a Kirschner wire, and immobilization after the procedure.
REFERENCES
- Albee FH. Formation of radius congenitally absent: condition seven years after implantation of bone graft. Ann Surg 1928;87(1):105-110.
- Bayne LG, Klug MS. Long-term review of the surgical treatment of radial deficiency. J Hand Surg Am1987;12(2):169-179.
- Buck-Gramcko D. Radialization as a new treatment for radial club hand. J Hand Surg Am 1985;10(6 pt 2):964-968.
- Damore E, Kozin SH, Thoder JJ, et al. The recurrence of deformity after surgical centralization for radial clubhand. J Hand Surg Am 2000;25(4):745-751.
- De Jong JP, Moran SL, Vilkki SK. Changing paradigms in the treatment of radial club hand: microvascular joint transfer for correction of radial deviation and preservation of long-term growth. Clin Orthop Surg 2012;4(1):36-44.
- Ekblom AG, Dahlin LB, Rosberg HE, et al. Hand function in children with radial longitudinal deficiency. BMC Musculoskelet Disord 2013;14:116.
- Evans DM, Gateley DR, Lewis JS. The use of a bilobed flap in the correction of radial club hand. J Hand Surg Br 1995;20(3):333-337.
- Goldberg MJ, Bartoshesky LE. Congenital hand anomaly: etiology and associated malformations. Hand Clin 1985;1(3):405-415.
- Goldfarb CA, Manske PR, Busa R, et al. Upper-extremity phocomelia reexamined: a longitudinal dysplasia. J Bone Joint Surg Am 2005;87(12):2639-2648.
- Goldfarb CA, Wall L, Manske PR. Radial longitudinal deficiency: the incidence of associated medical and musculoskeletal conditions. J Hand Surg Am 2006;31(7):1176-1182.
- James MA, Green HD, McCarroll HR, et al. The association of radial deficiency with thumb hypoplasia. J Bone Joint Surg Am 2004; 86-A(10):2196-2205.
- James MA, McCarroll HR Jr, Manske PR. The spectrum of radial longitudinal deficiency: a modified classification. J Hand Surg Am 1999;24(6):1145-1155.
- Manske PR, McCarroll HR Jr, Swanson K. Centralization of the radial club hand: an ulnar surgical approach. J Hand Surg Am 1981;6(5):423-433.
- Oishi SN, Carter P, Bidwell T, et al. Thrombocytopenia absent radius syndrome: presence of brachiocarpalis muscle and its importance. J Hand Surg Am 2009;34(9):1696-1699.
- Sayre RH. A contribution to the study of club-hand. Trans Am Orthop Assn 1893;6:208-216.
- Sestero AM, Van Heest A, Agel J. Ulnar growth patterns in radial longitudinal deficiency. J Hand Surg Am 2006;31(6):960-967.
- Shariatzadeh H, Jafari D, Taheri H, et al. Recurrence rate after radial club hand surgery in long term follow up. J Res Med Sci 2009;14(3):179-186.
- Starr DE. Congenital absence of the radius: a method of surgical correction. J Bone Joint Surg Am 1945;27(4):572-577.
- Vilkki SK. Distraction and microvascular epiphysis transfer for radial club hand. J Hand Surg Br 1998;23(4):445-452.
- Vilkki SK. Vascularized metatarsophalangeal joint transfer for radial hypoplasia. Semin Plast Surg 2008;22(3):195-212.
