DEFINITION
Proximal row carpectomy (PRC) involves removal of the proximal carpal row (scaphoid, lunate, and triquetrum).PRC has been described as a treatment option for a number of pathologic conditions: Scaphoid nonunion advanced collapse (SNAC) wristScapholunate advanced collapse (SLAC) wristKienböck diseaseChronic or missed perilunate dislocation Scaphoid osteonecrosis or Preiser disease Wrist deformity or contracture
ANATOMY
The proximal row of the wrist consists of three bones: scaphoid, lunate, and triquetrum.The proximal row moves as a single unit through intercarpal ligamentous attachments and bony congruity.The proximal row flexes with radial deviation and extends with ulnar deviation.The capitate, in the distal row, articulates with the lunate.The proximal capitate articular surface is relatively, although not completely, congruous with the lunate facet of the radius.
PATHOGENESIS
A number of pathologic conditions lead to wrist degeneration requiring PRC. Patients with progressive pain and limited motion can gain relief following this procedure.SNAC and SLACStage I: degenerative changes along the radial half of the radioscaphoid articulation. In SNAC wrists, the degenerative changes are typically limited to the articulation between the distal scaphoid fragment and the radius.Stage II: degenerative changes involving the entire radioscaphoid articulation (FIG 1). In SNAC wrists, the articulation between the proximal scaphoid fragment and the radius is preserved, and instead, stage II degeneration occurs in the scaphocapitate joint.Stage III: degenerative changes at the capitolunate joint. The radiolunate joint is spared.Kienböck diseaseStage I: normal plain radiographs with wrist pain and positive magnetic resonance imaging (MRI) finding Stage II: sclerosis without collapse of the lunateStage IIIa: lunate collapse without instabilityStage IIIb: where there is lunate collapse with carpal instability (dorsal intercalated segmental instability [DISI]: flexion of the scaphoid with extension of the lunate)Stage IV: fixed carpal instability with pancarpal degenerative changes Missed perilunate dislocationScaphoid osteonecrosis (Preiser disease)Congenital or spastic wrist and hand flexion contractures severe enough that a PRC allows deformity correction that tendon lengthening procedures alone would be unable to correct.
PATIENT HISTORY AND PHYSICAL FINDINGS

IMAGING AND OTHER DIAGNOSTIC STUDIES
Plain radiographs assist with making the underlying diagnosis (eg, SNAC wrist, SLAC wrist, Kienböck disease).Evaluate the articular facets and surfaces, specifically the head of the capitate and lunate facet of the radius.Look for other sources of limited wrist motion, diminished grip strength, and pain (eg, thumb carpometacarpal arthritis, scapholunate instability without degenerative changes, fracture).MRI has limited use with the exception of suspected Kienböck disease or Preiser disease.
DIFFERENTIAL DIAGNOSIS
Triangular fibrocartilage complex or distal radioulnar joint pathology Extensor carpi ulnaris, flexor carpi ulnaris, flexor carpi radialis tendinitis De Quervain tenosynovitisThumb carpometacarpal arthritisScapholunate or lunotriquetral instability without degenerative changes
SURGICAL MANAGEMENT
The integrity of the articular cartilage on the head of the capitate and the lunate facet of the radius are critical. The ultimate assessment is made intraoperatively.IndicationsSLAC and SNAC wrist degeneration: stage I, II, or III (only if the degenerative changes at proximal capitate are limited to thinning or minor fissuring)Kienböck disease (stage IIIb)Chronic or missed perilunate dislocations Scaphoid osteonecrosis (Preiser disease) Wrist deformity or contractureContraindicationsActive inflammatory arthritis (rheumatoid arthritis). PRC may be used for inflammatory arthritis patients with “burnout” disease (those without active synovitis).Advanced degenerative changes at the proximal articular surface of the capitate or lunate facet of the radius Ulnar carpal translation or subluxation of the radiocarpal jointRelative contraindicationsHeavy laborersYoung (younger than 35 years) active patients8
PREOPERATIVE PLANNING
Review the plain radiographs of the wrist. Scrutinize the location of degenerative changes.Obtain consent for alternative procedures from the patient (ie, if you find excessive degenerative changes on the capitate head, you might proceed with an intercarpal arthrodesis).Regional anesthesia, general anesthesia, or a combination of the two (for postoperative analgesia) is suitable.
POSITIONING
The patient is supine with the arm on a radiolucent arm board.A nonsterile tourniquet preset at 250 mm Hg is on the upper arm.The shoulder, elbow, and hand are positioned such that the hand rests in pronation at the center of the arm board.
TECHNIQUES
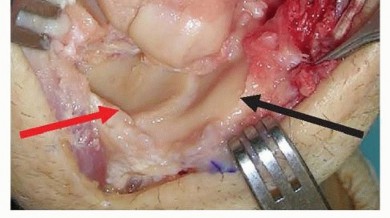
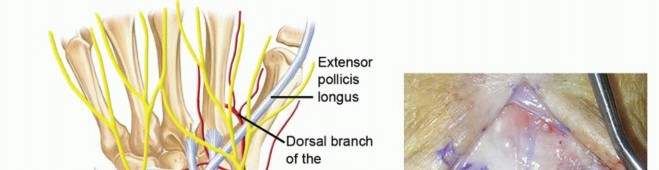
INCISION AND EXPOSURE


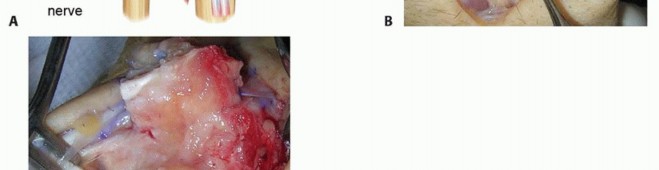

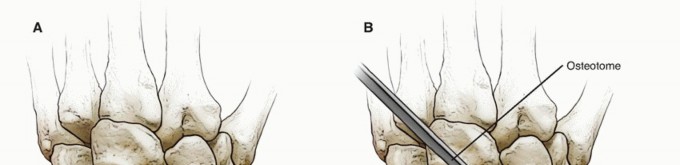
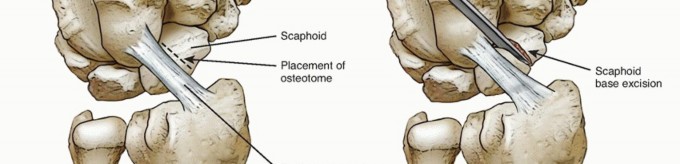


TECH FIG 2 • A,B. The appropriate location for the scaphoid osteotomy. C. A large threaded pin inserted into the lunate is used to facilitate resection. D. An elevator placed in the lunotriquetral joint and then levered against the triquetrum helps strip the volar capsule off the lunate. E. Resected lunate.
ASSESSMENT OF REDUCTION AND IMPINGEMENT
RADIAL STYLOIDECTOMY
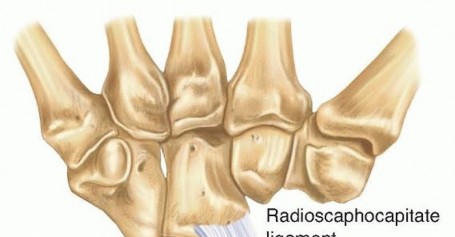
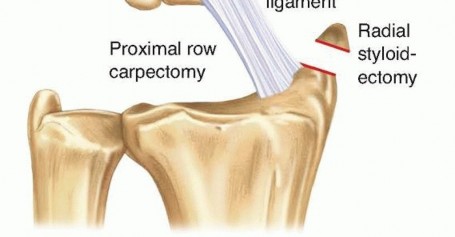
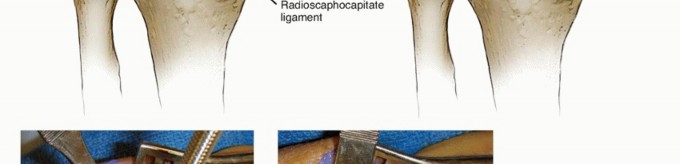
TECH FIG 3 • The amount of radial styloid that is removed and the direction of the osteotomy. The origin of the radioscaphocapitate ligament is carefully preserved.
WOUND CLOSURE
Proximal Row Carpectomy with Interposition Arthroplasty




PEARLS AND PITFALLS
POSTOPERATIVE CARE
PRC tends to be an outpatient procedure; an overnight stay may be necessary for postoperative pain or nausea.A short splint is applied in the operating room with the wrist in neutral and the fingers and thumb free at the metacarpophalangeal joints.Passive thumb and finger motion is encouraged immediately postoperatively, along with elevation and ice for the first 48 hours.At the first postoperative follow-up visit (in 10 to 14 days), the splint is removed, plain wrist AP and lateral radiographs are obtained to ensure the capitate is located in the radial lunate facet, and sutures are removed.At 2 weeks postoperatively, gentle active wrist extension and flexion and radioulnar deviation are added and a removable cock-up wrist splint or custom Orthoplast wrist splint is worn between exercises.Scar massage can begin once the incision is healed.Edema control may be necessary with compressive dressings.The removable splint can be discontinued as the patient feels comfortable (typically in 3 to 4 weeks).Therapy is initiated if the patient struggles to regain finger motion by 10 to 14 days. Therapy for wrist motion is initiated, if necessary, at 6 to 8 weeks.At 3 months, full activities are permitted.
OUTCOMES
A broad range in grip strength outcome has been reported postoperatively.A 60% to 100% grip strength of the contralateral wrist (and a 20% to 30% increase in postoperative grip vs. preoperative grip) can be expected.1,4,8A decrease in postoperative wrist motion can be expected, as well as a decrease in flexion-extension by 20%, a decrease in radioulnar deviation by 10%,4 and a 72- to 76-degree arc of motion in flexion and extension.3,7,8Satisfactory pain relief can be expected in 80% to 100% of patients.4,5P.981A Brazilian prospective randomized control trial comparing four-corner fusion to PRC showed similar functional results, decreased pain in both groups, and no statistically significant differences in range ofmotion or grip strength.2Return to work for manual laborers after PRC has been unpredictable, varying from 20% in one series4 to 85% in another.5A study with a minimum of 20-year follow-up showed 65% survival of the PRC, with failure (conversion to arthrodesis) at an average of 11 years postoperatively.9Age younger than 35 years has been shown to be predictive of early failure with PRC.
COMPLICATIONS
Use of pins has been associated with pin site infections and rapid degenerative changes when placed through the radiocapitate articulation (because of this, pins are not routinely recommended as they once were).Reflex sympathetic dystrophyExcessive styloidectomy and compromise of the radioscaphocapitate ligament Compromise of the radioscaphocapitate ligament can lead to ulnar carpal subluxation.Conversely, failure to check intraoperatively for radialsided impingement may lead to radial-sided wristpain postoperatively.Damage to sensory nerves (radial sensory and dorsal ulnar branches) Progressive arthritis
REFERENCES
- Begley BW, Engber WD. Proximal row carpectomy in advanced Kienböck's disease. J Hand Surg Am 1994;19(6):1016-1018.
- Bisneto EN, Freitas MC, Paula EJ, et al. Comparison between proximal row carpectomy and four-corner fusion for treating osteoarthrosis following carpal trauma: a prospective randomized study. Clinics 2011;66:51-55.
- Calandruccio JH. Proximal row carpectomy. J Am Soc Surg Hand 2001;1:112-122.
- Culp RW, McGuigan FX, Turner MA, et al. Proximal row carpectomy: a multicenter study. J Hand Surg Am 1993;18:19-25.
- Imbriglia JE, Broudy AS, Hagberg WC, et al. Proximal row carpectomy: clinical evaluation. J Hand Surg Am 1990;15:426-430.
- Mathiowetz V, Kashman N, Volland G, et al. Grip and pinch strength: normative data for adults. Arch Phys Med Rehabil 1985;66:69-74.
- Richou J, Chuinard C, Moineau G, et al. Proximal row carpectomy: long-term results. Chir Main 2010;29:10-15.
- Stern PJ, Agabegi SS, Kiefhaber TR, et al. Proximal row carpectomy. J Bone Joint Surg Am 2005;87(suppl 1, pt 2):166-174.
- Wall LB, Didonna ML, Kiefhaber TR, et al. Proximal row carpectomy: minimum 20-year follow-up. J Hand Surg Am 2013;38:1498-1504.
