DEFINITION
Rheumatoid arthritis is a disorder that can affect the hands and can cause systemic symptoms of fatigue, muscle pain, loss of appetite, depression, weight loss, anemia, and immunocompromise. The effect on the hands is a combination of tenosynovitis and inflammation of the metacarpophalangeal (MCP) synoviallining of the joints (synovitis).14,17Rheumatoid arthritis less frequently involves the proximal interphalangeal (PIP) joints of the hand; more commonly, the PIP joints are affected by degenerative arthritis or psoriatic arthritis. Degenerative arthritismay occur after trauma or infection or may arise as an idiopathic process.1
ANATOMY
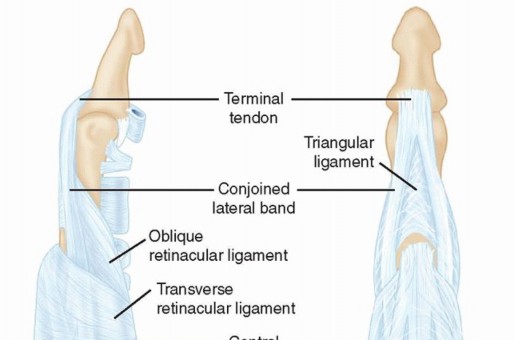
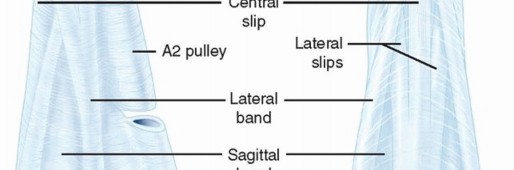
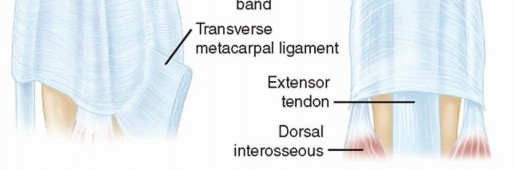
FIG 1 • Anatomy of the extensor mechanism of the finger.
PATHOGENESIS
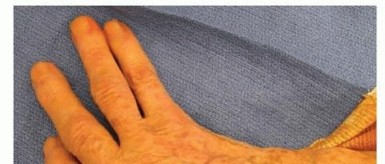

FIG 2 • Ulnar drift of the digits. P.1100
NATURAL HISTORY
Rheumatoid arthritis has a variable prognosis based on the severity of the disease and the structuresinvolved. Mild presentations may go undiagnosed for years, whereas severe presentations may progress to rapid joint destruction in the third or fourth decade of life.Three clinical stages of rheumatoid arthritis exist.First, swelling of the synovial lining, which causes pain, warmth, stiffness, redness, and fullness around the jointSecond, synoviocyte hypertrophy and proliferation leading to synovial thickeningThird, enzymatic release causing bone and cartilage destruction, ligamentous laxity, and tendon rupturesMedical management as well as surgical management, including synovectomy, can halt or minimize progression of rheumatoid arthritis.
PATIENT HISTORY AND PHYSICAL FINDINGS
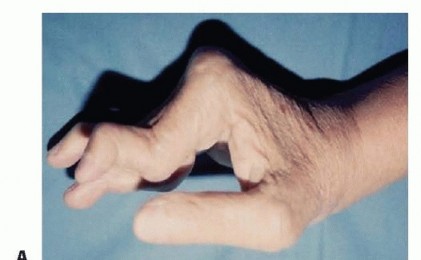
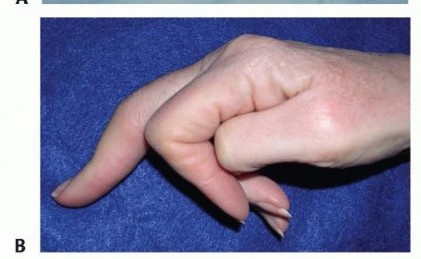
FIG 3 • A. Rheumatoid arthritis of the hand demonstrating swan-neck deformity and volar subluxation of the MCP joints. B. Boutonnière deformity of the digit. It is important to distinguish intrinsic tightness from extrinsic tightness. Extrinsic tightness is encountered when the long extensors of the digits are adherent to either the surrounding soft tissues or the metacarpals. The result is increased resistance to flexion of the PIP joint with the MCP in flexion. In either instance, the limitation of motion is important to clarify, as it can affect the outcome of implant arthroplasty of the MCP or the PIP joint.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Posteroanterior, lateral, and oblique views of the hands will adequately image the MCP joints. Brewerton views may add additional information.Posteroanterior and lateral views of the digits are preferred to image the PIP joints.
DIFFERENTIAL DIAGNOSIS
Psoriatic arthritis Chronic septic arthritis OsteomyelitisGoutArticular malunions of the MCP and PIP joints Scleroderma
NONOPERATIVE MANAGEMENT
Nonoperative management in rapidly progressing rheumatoid arthritis is largely ineffective.In the quiescent forms of rheumatoid arthritis, nighttime wrist and hand splinting in conjunction with medical management may provide pain relief. Various combinations of prednisone, remitting agents (eg, methotrexate, hydroxychloroquine sulfate, sulfasalazine, adalimumab, etanercept, infliximab, minocycline), and nonsteroidal anti-inflammatory agents may prove effective for extended periods in certain cases.During periods of active rheumatoid arthritis of the MCP joints, corticosteroid injections into the joint may provide acute pain relief and improve function in the short term.The symptoms of MCP and PIP joint degenerative arthritis may come and go, successfully responding to nighttime wrist and hand splinting and nonsteroidal anti-inflammatory agents.Corticosteroid injection into the MCP and PIP joints for advanced degenerative arthritis seldom provides longterm benefits.
SURGICAL MANAGEMENT
The indications for surface replacement or pyrocarbon MCP arthroplasty are similar to those for flexible MCP implants. These include pain in the face of deformity and worsening function.Surface replacement implants are designed to recreate the anatomy of a native joint, potentially resulting in greater stability than with flexible MCP implants.The enhanced stability of these implants is best demonstrated in the index and long fingers, where flexible MCP implants are prone to fracture and failure due to the increased forces born by these joint in pinch.Contraindications to surface replacement implant arthroplasty of the MCP joint include infection, lack of adequate bone stock, insufficient radial or ulnar collateral ligament support, lack of adequate soft tissue coverage, and excessively small metacarpal or proximal phalanx medullary canals.These implants rely on intact soft tissue elements. This includes functioning flexors and extensors as well as intact radial and ulnar collateral ligaments.Indications for PIP joint surface replacement arthroplasty are pain and diminishing function in the context of advanced radiographic articular degeneration.1,8Contraindications to PIP joint surface replacement arthroplasty include inadequate bone stock of either the proximal or the middle phalanx, ulnar or radial collateral ligament insufficiency, acute or chronic infection, inadequate soft tissue coverage, insufficient digital flexor function, or disruption of the extensor central slip insertion on the middle phalanx.Relative contraindications include the presence of a static swan-neck or boutonnière deformity.10The importance of postoperative therapy should be emphasized. To ensure that the implants heal with a stable and a functional range of motion, the patient must wear a combination of static and dynamic splints for several weeks to months after. Patients must also be aware that heavy lifting or gripping must be avoided indefinitely.
PREOPERATIVE PLANNING
Sizing templates with a 3% parallax enlargement are available for MCP and PIP joint systems and should be used preoperatively to give the surgeon an idea of the size implant required.
POSITIONING
The patient is positioned supine, with the arm placed on an arm board for either MCP or PIP joint surface replacement arthroplasty.A nonsterile tourniquet is placed proximal to the drapes on the arm and can be accommodated at the forearm or upper level. Some surgeons prefer the use of a simple finger tourniquet.The hand is pronated to allow access to the dorsum.
APPROACH
For MCP surface replacement arthroplasty, two different incisions can be used.A transverse incision across the dorsum of the hand, centered over the MCP joints, will facilitate access to multiple joints.Alternatively, multiple longitudinal incisions can be used to address all four MCP joints individually. If a single joint is being addressed, a longitudinal incision should be used.For PIP joint surface replacement arthroplasty, a midline longitudinal incision is preferred.Alternative approaches include the lateral approach and the volar approach.P.1102
TECHNIQUE
Metacarpophalangeal Joint Surface Replacement Arthroplasty
METACARPOPHALANGEAL JOINT SURFACE REPLACEMENT ARTHROPLASTY
EXPOSURE
The extensor mechanism is exposed through either a dorsal longitudinal incision or through a transverse incision, depending on surgeon preference.Preserve the dorsal veins.Incise the extensor hood just ulnar to the extensor mechanism. Retract the extensor hood and extensor mechanism radially.In the rheumatoid patient, the extensor tendon ulnarly translates with destruction of the radial sagittal band. If possible, dissect the sagittal bands from the capsule and preserve them so that the extensor tendon can be relocated and the sagittal bands imbricated at the end of the procedure in order to maintain a centralized extensor tendon position.Incise the remnants of the MCP joint capsule and use small Hohmann retractors to deliver the head of the metacarpal into the wound.After the joint is exposed, perform a synovectomy, carefully preserving the collateral ligaments.If the joint is irreducible, it may be necessary to release one or both collateral ligaments from their origins.Tag the ends of the collateral ligaments with 4-0 nonabsorbable suture for later repair to bone at their tuberosity origins. Joint Preparation and Trial Implant Insertion

TECH FIG 1 • A. Exposure of the MCP joint demonstrating the bone cuts for preparation of MCP surface replacement arthroplasty. B. Broaching of the metacarpal preparing for MCP surface replacement arthroplasty. (Courtesy of Small Bone Innovations, Morrisville, PA.) Remove the articular surface along with a small portion of the base of the proximal phalanx, preserving the collateral ligaments (TECH FIG 1A).Contracture of the ulnar capsule may require detaching the ulnar collateral ligament to achieve alignment of the finger in some circumstances.Insert an awl into the dorsal aspect of the intramedullary canal of the metacarpal (TECH FIG 1B). Perform sequential broaching for the metacarpal until a proper fit has been attained.For the index and long fingers, the broaching is slightly ulnarly displaced. This provides a better moment arm for the radial intrinsic and extrinsic tendons to compensate for ulnar drift.Repeat the broaching in a similar fashion for the proximal phalanx.A plastic impactor with a concave surface aids insertion of the metacarpal proximal trial component.Avoid forceful impaction in order to avoid fracture.A convex impactor aids insertion and seating of the distal component.Once the trial components are inserted and the joint is reduced, check component fit and position using an image intensifier. Then assess range of motion, component tracking, and stability.Revisions of bone cuts may be necessary for soft tissue balancing and to ensure adequate range of motion.If release of the collateral ligaments was required, drill two holes through the tuberosity at the dorsoradial and dorsoulnar aspect of the remaining metacarpal head for reattachment of the ligaments. Insert sutures for repair of the collateral ligament (4-0 nonabsorbable suture preferred).
FINAL IMPLANT INSERTION
Irrigate the intramedullary canal with saline and 0.5% neomycin solution, then dry it.Inject polymethylmethacrylate (PMMA) in a liquid state into the metacarpal and the proximal phalanx using a size no. 14 plastic Angiocath catheter attached to a 10-mL syringe.Under some circumstances, “finger packing” may be necessary.P.1103Insert the distal component first. Convex and concave plastic impactors are provided to assist in implant insertion (TECH FIG 2).Avoid impacting with metallic instruments, which can accelerate prosthetic wear.The joint is extended and viewed under the image intensifier before allowing the cement to harden so that last-minute corrections in alignment can be made.Cement fixation of one finger at a time is advisable if positioning is difficult.If multiple MCP joints are to be implanted, it may be easier to do the distal components as a group, followed by the proximal components.After the cement has cured, check passive range of motion to ensure adequate range without impingement or prosthetic binding.For MCP joint arthroplasty using pyrocarbon implants, a press-fit technique is typically used instead of cement.
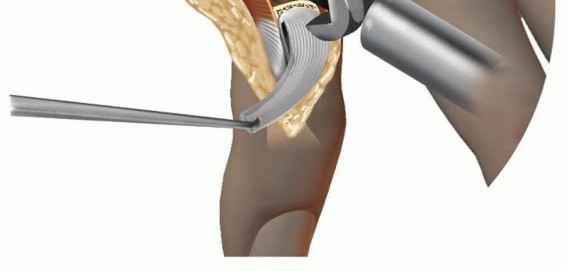
CLOSURE AND SOFT TISSUE BALANCING

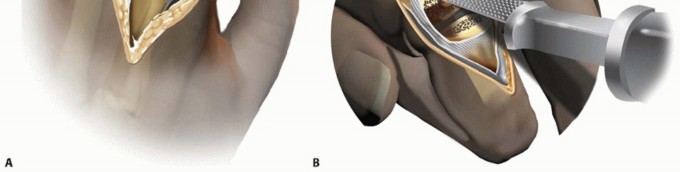
TECH FIG 2 • Insertion of the metacarpal component of the MCP surface replacement arthroplasty. (Courtesy of Small Bone Innovations, Morrisville, PA.) Close any remaining capsule with absorbable suture before extensor apparatus closure.Centralize the extensor tendon and imbricate the radial sagittal bands in rheumatoid hands using nonabsorbable suture.A pants-over-vest centralization of the sagittal bands may be required in moderate to severe ulnar drift along with intrinsic releases or crossed-intrinsic transfers (TECH FIG 3).With the finger held in slight overcorrection, imbricate the radial sagittal band over the extensor tendon.The skin is closed in a routine manner and a splint is applied with the MCP joints in slight flexion.
POSTOPERATIVE CARE
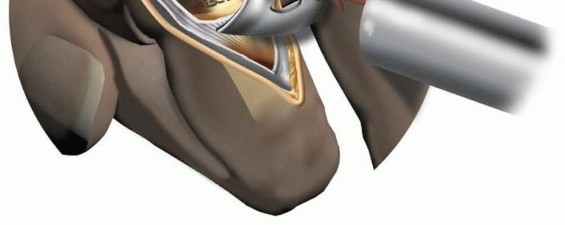
TECH FIG 3 • Radially directed “pants-over-vest” reefing of the extensor mechanism after MCP surface replacement arthroplasty. (Courtesy of Small Bone Innovations, Morrisville, PA.)
Proximal Interphalangeal Joint Surface Replacement Arthroplasty
Proximal Interphalangeal Joint Surface Replacement Arthroplasty
EXPOSURE
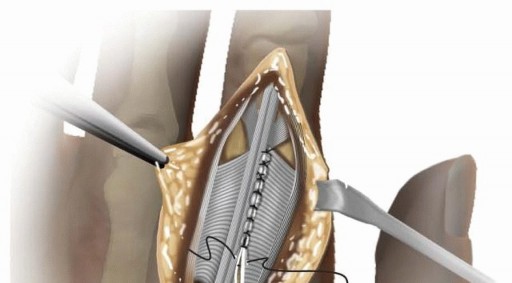
Through a midline longitudinal incision, reflect the extensor tendon distally by creating a distally based flap, as described by Chamay2 (TECH FIG 4A).Identify and incise remnants of the dorsal PIP joint capsule.Protect the radial and ulnar collateral ligaments using small Hohmann retractors while bringing the articular surface of the middle phalanx into view. Joint Preparation and Trial Implant Insertion


TECH FIG 4 • A. Proximal phalanx exposed using the Chamay approach. An oscillating saw is used to accomplish an osteotomy in preparation for the PIP joint surface replacement arthroplasty placement. B. Broaching of the proximal phalanx in preparation for PIP joint surface replacement arthroplasty. During the osteotomy, protect the origins of the radial and ulnar collateral ligaments by using small retractors or by hyperflexing the joint.It may be necessary to release a small portion of the proximal phalangeal origin of the collateral ligaments to facilitate the proximal phalangeal osteotomy and prosthesis insertion.Minamikawa et al10 have shown that the PIP joint remains stable after removal of 50% of the collateral ligament substance.While protecting the volar plate with a small retractor, use a 2-mm burr to assist in making a small back cut (or chamfer cut) to accept the posterior aspect of the prosthetic condyles of the proximal phalangeal component.This can also be accomplished with the oscillating saw but that can place the volar plate and flexor tendons at risk.Make a perpendicular osteotomy at the base of the middle phalanx with a small oscillating saw blade or a small rongeur and remove no more than 1 to 2 mm of bone.Protect the collateral ligament insertions with small retractors or by hyperflexing the digit.Broach the proximal and middle phalanges with specific and sequential instruments.Broach the proximal and middle phalanges to the largest size possible (TECH FIG 4B). Undersized components can result in limited motion due to bony impingement during flexion.Insert the trial components using proximal and middle phalanx-specific impactors.The components are not modular and are generally not interchanged. Under certain circumstances, such as revision surgery, it is permissible to implant unmatched sizes, but no more than one size up or one size down should be used and this is considered an off-label use of the prosthesis.After trial component insertion, examine the digit for implant position, range of motion, and stability as detailed for the MCP joint. Make appropriate adjustments.
FINAL IMPLANT INSERTION AND CLOSURE
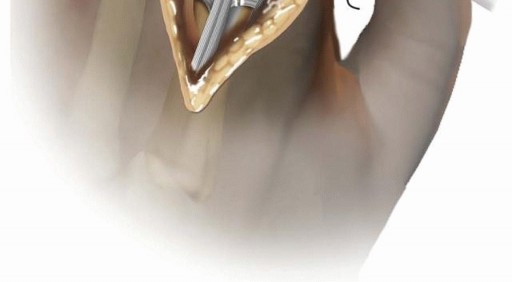
Implant the permanent components by “press-fit” using the “no-touch” technique.Cementing is discouraged except perhaps in cases with capacious canals or in patients with substantial bone loss or substantial articular erosion. In these circumstances, the prosthetic stems and flanges are simply coated with cement. Excessive cement packing into the medullary canal is not necessary.Another technique is to pack the canal with morselized allograft bone. This is analogous to the Ling technique described for revision total hip arthroplasty.5Using specific impactors, seat the permanent components (TECH FIG 5). Repair the extensor mechanism with 3-0 braided nonabsorbable suture. Release the tourniquet before skin closure.The patient leaves the operating room with a sterile dressing, splinted in extension.
POSTOPERATIVE CARE

TECH FIG 5 • Insertion of the proximal phalangeal component of the PIP surface replacement arthroplasty. (Courtesy of Small Bone Innovations, Morrisville, PA.) The static bedtime splint is used for an additional 6 weeks. Heavy lifting or gripping is not permitted.The rehabilitation program is enhanced by the close supervision of a hand therapist. The first week of therapy is best carried out with daily supervision.Follow-up examinations should include range-of-motion assessment for all the joints of the hand and wrist. Static deformities, grip strength, and pinch strength should also be assessed and recorded.Follow-up radiographic examination includes posteroanterior, lateral, and oblique views of the hand. Any residual deformity should also be assessed and recorded.For the PIP joint surface replacement arthroplasty, a controlled rehabilitation protocol is needed to prevent central slip failure.PEARLS AND PITFALLS
|||PIP joint|1. Take care to preserve the insertion of the central slip.|surface|1. Osteotomy of the proximal phalanx must avoid the origin of the PIP jointreplacement|collateral ligaments.arthroplasty|1. Remove only a small amount of bone from the middle phalanx.MCP jointsurface replacement arthroplasty1. Contracture of the ulnar capsule may require detaching the ulnar collateralligament.2. Broaching of the index finger should be slightly ulnarly displaced.3. Centralization of the extensor tendon is generally necessary in rheumatoid hands; it can be achieved by imbricating the radial sagittal bands.4. Imbrication of the radial sagittal bands should be performed with the digit in radial deviation.5. “Watertight” closure of the extensor mechanism is necessary to prevent PIP joint flexion lag or contracture.1. Broach the proximal phalanx to the largest size that can be accommodated. Failure to use appropriate-sized implants may result in subsidence of the implants and posterior cortical impingement of the phalanges.
OUTCOMES
Initial results after 76 PIP joint surface replacement arthroplasties were published.9 At a mean follow-up of 4.5 years, 32 joints had good results, 19 fair, and 25 poor.Better results were obtained with arthroplasties performed through a dorsal approach rather than thevolar approach.Range of motion at follow-up averaged -14 degrees of extension and 61 degrees of flexion. There was a 12-degree improvement in the flexion-extension arc compared to the preoperative examination.A longer term outcome review of 67 metal polyethylene PIP arthroplasties has recently been published from the same institution.12With a mean follow up of 8.8 years, the study concluded that this technique yielded joints with minimal pain and ranges of motion similar to preoperative levels.There were 22 complications in 14 patients, resulting in four interphalangeal fusions and two amputations.A review of 43 PIP surface replacement arthroplasties in 25 patients was published.7 Follow-up time averaged 37 months (range, 12 to 72 months).It was notable that 10 of the 11 failed arthroplasties requiring revision were due to looseningassociated with lack of cement use.A retrospective review of 31 pyrocarbon arthroplasties of the PIP joint performed by a single surgeon in 17 patients with interphalangeal joint osteoarthritis has also been published.16At mean follow-up of 55 months, the postoperative range of motion decreased from 57 degrees to 31 degrees.“Complications included implant fracture (one joint), dislocation (five joints), squeaking (eleven), loosening (fifteen), and interphalangeal joint contracture (twenty).P.1106Six joints required a reoperation (an arthrodesis in four joints, a silicone arthroplasty in one, and excision of exostosis in one). Implant migration was severe for seven proximal phalanx implants andthree distal phalanx implants, and one implant breached the phalangeal cortex.”The MCP joint surface replacement arthroplasty (Small Bone Innovations, Morrisville, PA) has been available in Europe for 8 years and is under clinical trial in the United States. No series has been published reporting results of this implant. Although from a theoretical perspective there are advantages to the use of the MCP joint surface replacement arthroplasty, it currently cannot be considered a replacement for the Swanson silastic MCP joint spacer.Previous primate studies have shown no evidence of debris or inflammatory reaction after implantation of the pyrolytic carbon MCP joint arthroplasty. Good bone incorporation of the prosthesis was also observed.In a 1999 study, a series of 151 pyrolytic carbon MCP prostheses (Ascension Orthopedics, Austin, TX) implanted over an 8-year period, mostly in patients with rheumatoid arthritis, were followed up at anaverage of 11.7 years.3The arc of MCP joint motion improved an average of 13 degrees. The 10-year survivorship was 81.4%.At follow-up, the degree of digital ulnar drift was the same as preoperative. Complications led to 18 implant revisions (12%).
COMPLICATIONS
PIPFailure of the central slip can occur, resulting in extensor lag or, more commonly, a flexion contracture or boutonnière deformity. An analysis of reoperations following PIP joint arthroplasty found that 76 of 294 PIP joints required reoperation. Extensor mechanisms dysfunction was the most common reasonfor reoperation which occurred in 51 of the 76 cases.13With the volar approach, failure of the volar plate may occur, leading to swan-neck deformity. Tenodesis as well as joint instability and joint subluxation can occur.Postoperative infection or prosthesis loosening is seldom seen.9 MCPStiffness Loosening SubluxationProliferative synovitisSqueaking in pyrocarbon implants
REFERENCES
- Amadio PC, Murray PM, Linscheid RL. PIP arthroplasty. In: Morrey BF, ed. Joint Replacement Arthroplasty, ed 3. New York: Churchill Livingstone, 2003:163-174.
- Chamay A. A distally based dorsal and triangular tendinous flap for direct access to the proximalinterphalangeal joint. Ann Chir Main 1988;7:179-183.
- Cook SD, Beckenbaugh RD, Redondo J, et al. Long-term follow-up of pyrolytic carbon metacarpophalangeal implants. J Bone Joint Surg Am 1999;81(5):635-648.
- Flatt AE. Some pathomechanics of ulnar drift. Plast Reconstr Surg 1966;37:295-303.
- Halliday BR, English HW, Timperley AJ, et al. Femoral impaction grafting with cement in revision total hip replacement. Evolution of the technique and results. J Bone Joint Surg Br 2003;85(6):809-817.
- Ito J, Koshino T, Okamoto R, et al. Radiologic evaluation of the rheumatoid hand after synovectomy and extensor carpi radialis longus transfer to extensor carpi ulnaris. J Hand Surg Am 2003;28(4): 585-590.
- Jennings CD, Livingstone DP. Surface replacement arthroplasty of the proximal interphalangeal joint using the PIP-SRA implant: results, complications, and revisions. J Hand Surg Am 2008;33(9):1565. e1-e11.
- Linscheid RL. Implant arthroplasty of the hand: retrospective and prospective considerations. J Hand Surg Am 2000;25(5):796-816.
- Linscheid RL, Murray PM, Vidal MA, et al. Development of a surface replacement arthroplasty for proximal interphalangeal joints. J Hand Surg Am 1997;22(2):286-298.
- Minamikawa Y, Horii E, Amadio PC, et al. Stability and constraint of the proximal interphalangeal joint. J Hand Surg Am 1993;18: 198-204.
- Murray PM. New-generation implant arthroplasties of the finger joints. J Am Acad Orthop Surg 2003;11:295-301.
- Murray PM, Linscheid RL, Cooney WP III, et al. Long-term outcomes of proximal interphalangeal joint surface replacement arthroplasty. J Bone Joint Surg Am 2012;94(12):1120-1128.
- Pritsch T, Rizzo M. Reoperations following proximal interphalangeal joint nonconstrained arthroplasties. J Hand Surg Am 2011;36(9): 1460-1466.
- Smith RJ, Kaplan EB. Rheumatoid deformities at the metacarpophalangeal joints of the fingers: a correlative study of anatomy and pathology. J Bone Joint Surg Am 1967;49A:31-47.
- Stack HG, Vaughan-Jackson OJ. The zigzag deformity in the rheumatoid hand. Hand 1971;3:62-67.
- Sweets TM, Stern PJ. Pyrolytic carbon resurfacing arthroplasty for osteoarthritis of the proximal interphalangeal joint of the finger. J Bone Joint Surg Am 2011;93(15):1417-1425.
- Wilson RL, Carlblom ER. The rheumatoid metacarpophalangeal joint. Hand Clin 1989;5:223-237.
