DEFINITION
Arthritis of the metacarpophalangeal (MCP) or proximal interphalangeal (PIP) joints may cause pain, deformity, and decreased motion. Rheumatoid arthritis (RA), osteoarthritis, and posttraumatic arthritis are common causes.Silicone implant arthroplasty may be considered as a surgical option after failure of nonoperative treatment in the patient with pain, functional disability, or both secondary to arthritis at the MCP or PIP joint.The primary function of the silicone implant is to serve as a dynamic spacer until the joint is encapsulated; thereafter, the joint can be expected to maintain alignment and provide a satisfactory range of motion.
ANATOMY
METACARPOPHALANGEAL JOINT
The MCP joint is condyloid with motion in three planes: flexion-extension, abduction-adduction, and rotation.The head of the metacarpal is wider on its volar aspect, providing greater stability in flexion. The radial condyle is larger as well, contributing to the ulnar deviation posture most commonly seen in RA patients.Collateral ligaments arise dorsal to the center of rotation; this, together with the shape of the metacarpal head, contributes to the cam effect that is manifest by collateral ligament laxity in extension and tightness in flexion.Hyperextension of the MCP joints is common; however, the volar plate limits excessive motion.
PROXIMAL INTERPHALANGEAL JOINT
The PIP joint is a hinge joint with an average arc of motion of 0 to 100 degrees of flexion.The bony anatomy is crucial to PIP joint stability in all positions; the base of the middle phalanx is wider volarly, thus helping to prevent dorsal dislocation. The PIP joint is more stable in all positions compared to the MCP joint.The proper collateral ligaments originate from the center of rotation of the proximal phalanx head and insert onto the volar base of the middle phalanx; they provide stability in all positions. The accessory collateral ligaments insert onto the volar plate and provide more stability in extension. There is no significant cam effect with the PIP joint.The volar plate resists hyperextension and is a key supporting structure of the joint.
PATHOGENESIS
Arthritis of the MCP or PIP joints may be idiopathic, posttraumatic, or inflammatory (RA).Idiopathic osteoarthritis involves the distal interphalangeal joint most commonly, but the PIP joint is also affected; the MCP joint is less commonly involved.The PIP joint is the most frequently traumatized finger joint and, thus, has the highest incidence of posttraumaticarthritis. Given the shortcomings of the salvage procedures for PIP joint arthritis, an anatomic joint reduction and aggressive restoration of the normal anatomy after trauma is critical to reduce the risk of arthritis.The bony congruity of the PIP joint makes it poorly tolerant of any loss of cartilage; deformity and loss of motion may progress quickly.Inflammatory arthritis (RA) most commonly affects the MCP joint but may also involve the PIP joint. In RA, a proliferative synovitis compromises the soft tissue support of the affected joint and may lead to the characteristic deformities at the MCP joint, including volar subluxation (and a flexed posture) and ulnar deviation. The PIP joint is less predictable because attenuation of the volar supporting structures may lead to joint hyperextension, whereas compromise of the central slip insertion will lead to a joint flexion deformity.The efficacy of the disease-modifying antirheumatic drugs has dramatically decreased the need for joint arthroplasty in these patients.
NATURAL HISTORY
The natural history of osteoarthritis or posttraumatic arthritis of the PIP joint is progression with loss of motion, pain, and, in some patients, deformity. The MCP joint is less commonly affected and is also more tolerant of arthritis, given its increased mobility in all planes.In the patient with severe RA not controllable by disease-modifying antirheumatic drugs, joint inflammation will lead to progression of the arthritis.The functional effect of the arthritis depends on the degree of involvement, the specific joint, and the involvement of the adjacent joints.
PATIENT HISTORY AND PHYSICAL FINDINGS
It is vital that the surgeon understand how the arthritis specifically affects the function of a particular patient. This depends on many factors, including adjacent joint involvement, specific patient activities, and the degree of pain experienced.
PHYSICAL EXAMINATION
Key components in the physical examination are as follows:Palpate along the joint line to confirm the site of pain and presence of synovitis.P.1092Measure active and passive range of motion of the joint with a goniometer. Joint motion is lost with arthritis. Pain with motion is noted.Measure coronal plane deformity (angulation) of the joint with a goniometer. Progressive arthritis leads to joint deformity.Stress the joint in a radial-ulnar directions to evaluate the collateral ligaments. The MCP should be tested in flexion; the PIP joint may be tested in any position but is most commonly tested in extension. Attenuation of collateral ligaments may occur in RA or after trauma.Assess the integrity of intrinsic and extrinsic tendon function and strength: most commonly abnormal in RA or after prior traumaAssess for tendon shortening or lengthening (eg, after repair of an open injury) and the presence of tendon adhesions, which is most important in posttraumatic conditions.Perform the Elsen test: Integrity of the central slip is important when contemplating PIP joint arthroplasty.Evaluate alignment and function of the adjacent joints (including the wrist), as there is an intimate relationship between the joints.In inflammatory conditions, the more proximal joints, most importantly the wrist, are also examined. If wrist deformity is not corrected before surgical correction of distal disease, surgical correction (such as MCP arthroplasty) will have a higher incidence of failure due to the uncorrected deforming forces.Assess for intrinsic or extrinsic contractures after hand trauma.Perform the intrinsic tightness (Bunnell) test: If the intrinsics are tight, therapy or surgical intervention may be needed.
IMAGING AND OTHER DIAGNOSTIC STUDIES


FIG 1 • A. RA affecting hand, with most notable disease affecting MCP joints. The wrist is also affected. B. Isolated osteoarthritis of the MCP joint of the long finger. C. Posttraumatic arthritis affecting the small finger PIP joint. Magnetic resonance imaging (MRI) and computed tomography (CT) are of limited use in the evaluation of the MCP and PIP joints.
DIFFERENTIAL DIAGNOSIS
Acute fracture with or without joint subluxation Collateral ligament injuryJoint infectionFlexor or extensor mechanism injury
NONOPERATIVE MANAGEMENT
Anti-inflammatory medications Steroid injectionsHand therapy to address contractures, including splinting
SURGICAL MANAGEMENT
Surgery is considered if nonoperative management fails. Given the limitations of silicone implant arthroplasty as noted in the following text, the decision for surgical intervention should be patient driven.The best outcome is expected in patients with joint-based pain and a well-preserved arc of motion and minimal deformity. Patients without pain and presenting with deformity or a lack of motion are not ideal candidates for arthroplasty, especially if the adjacent joints are functioning well. Joint arthroplasty, of any variety, does not reliably increase motion at long-term follow-up.In RA, an ulnar drift and volar subluxation of the MCP joints with a flexion posture of the joints may lead to weakness and a loss of the ability to grasp larger objects. These deformities are also unsightly. Surgical intervention in these patients can be expected to improve the appearance and function of the hand.
PREOPERATIVE PLANNING
All imaging studies are reviewed. Involvement of adjacent joints is assessed.P.1093Multiple MCP or PIP joints can be treated with silicone arthroplasty at the same surgical setting, but we do not typically recommend MCP and PIP joint silicone arthroplasty in the same finger.In patients with symptomatic disease at both the MCP joint and the PIP joint, the MCP is typically treated with silicone implant arthroplasty and the PIP joint is fused.An assessment of the ligamentous stability of the MCP and PIP joints is performed under anesthesia.MCP and PIP arthroplasty is performed cautiously in the index (or long) finger, as pinch forces may be problematic for joint stability if the collateral ligaments are elongated or compromised with surgery.Templating is performed to ensure that appropriate-sized implants are available.
POSITIONING
The patient is supine with the extremity on an arm table. A nonsterile arm tourniquet is used.General or axillary block anesthesia is used.
APPROACH
The MCP joint is approached from dorsally with a midline incision.The PIP joint may be approached from either the dorsal or volar approach.
TECHNIQUE
Metacarpophalangeal Joint Silicone Arthroplasty
METACARPOPHALANGEAL JOINT SILICONE ARTHROPLASTY
INCISION AND DISSECTION

TECH FIG 1 • A. Transverse dorsal incision for MCP arthroplasty of all four fingers. The incision may be straight or undulating. B. The interval between the extensor tendons may be chosen to approach the joint for the index or small fingers. The interval between the extensor digitorum communis and the extensor indicis proprius is illustrated. C. The joint is débrided. This can be an extensive process in severe rheumatoid disease. It may be necessary to recess the collateral ligaments off their origin from the metacarpal head. Carefully protect their insertion onto the base of the proximal phalanx.In osteoarthritis or posttraumatic arthritis, the collateral ligaments need not be released if adequate exposure can be obtained.If the joint is volarly subluxated, it may exhibit a flexion contracture that must be released.Perform a soft tissue release using a Freer to elevate the volar plate off the volar distal metacarpal; this, together with bony resection, will allow joint reduction.A sufficient release has been accomplished once the proximal phalanx can be mobilized dorsal to the metacarpal head.
BONE PREPARATION
TECH FIG 2 • A. An oscillating saw is used to cut the metacarpal head just distal to the collateral ligament origin perpendicular to the long axis of the bone. B. The metacarpal is prepared by reaming and then broaching as depicted. C. The importance of supination of the index finger is apparent in this clinical picture of pinch. Broaching in slight supination can improve pinch position. Prepare the base of the proximal phalanx by removing the articular cartilage using an osteotome or rongeur. Carefully protect the collateral ligament insertions.Use an awl to identify the metacarpal medullary canal first.The awl typically enters the canal dorsal to the apparent center of the cut end of the metacarpal given the dorsovolar bone curvature.Use hand reamers to prepare the bone.Use progressive broaches, taking care to ensure correct broach alignment and integrity of the cortex (TECH FIG 2B).The ring finger metacarpal is frequently narrower and may require more reaming, use of a burr, and potentially a smaller implant.Once the metacarpal is prepared, initiate the same procedure for the proximal phalanx.The base of the proximal phalanx can be reamed in slight supination for the index finger to improve pinch (TECH FIG 2C).
IMPLANT PLACEMENT AND CLOSURE

TECH FIG 3 • A. A trial implant is placed to test range of motion and implant fit. B. After final implant placement, the collateral ligaments are repaired through drill holes placed in the metacarpal. This is most important for the radial collateral ligament in RA.

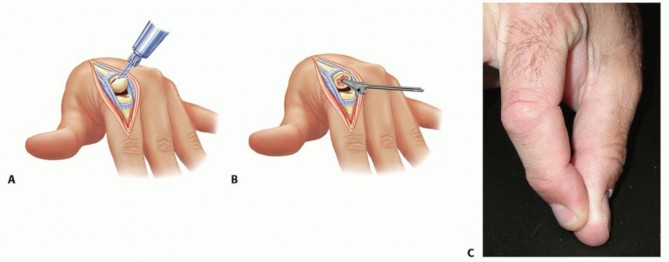
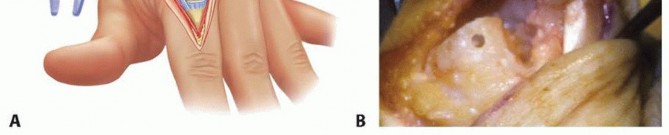
TECH FIG 4 • A. A volar skin incision is centered at the PIP joint in a Brunner fashion. B,C. The flexor tendon sheath is incised between the A2 and A4 pulleys to allow retraction of the tendons. D. The volar plate is released proximally for exposure.

TECH FIG 5 • Postoperative radiograph of patient with diffuse osteoarthritis. Note the silicone implant arthroplasties for the PIP joints of the index and long fingers as well as the fusions of the distal interphalangeal joints of the long and ring fingers. Clinical alignment was excellent.
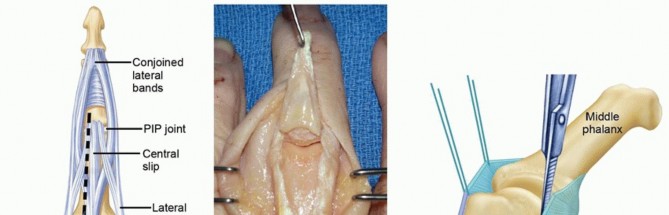
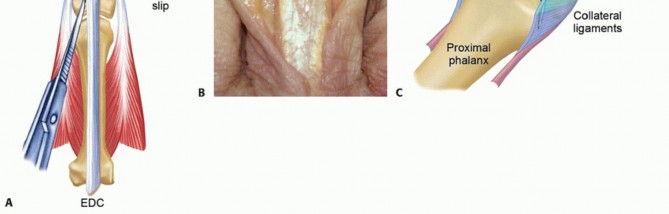
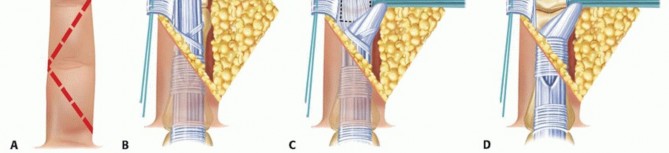
TECH FIG 6 • A. Preservation of the central slip is crucial for successful postoperative rehabilitation. B. The Chamay approach may be used for PIP joint exposure. C. The collateral ligaments may be recessed off the head of the proximal phalanx. Obtain C-arm or standard radiographs to confirm clinical alignment (TECH FIG 5). The flexor sheath need not be repaired.Use 4-0 nylon sutures to close the skin. Dorsal Approach for Proximal Interphalangeal Joint Arthroplasty Make a straight or gently curved longitudinal incision centered over the dorsal PIP joint. Raise full-thickness flaps off of the extensor mechanism.Split the central slip longitudinally and elevate it radially and ulnarly, taking care not to injure the central slip insertion and create an iatrogenic boutonnière deformity. Other alternatives for improved joint exposure include the following:The longitudinal split of the extensor mechanism may be carried to one or both sides of the central slip insertion for its protection. We prefer the exposure between the lateral and central slips (TECH FIG 6A).The Chamay approach may be used. A distally based triangular flap of the extensor mechanism is created; this provides excellent joint exposure and allows adjustment of any preoperative imbalance ofthe extensor mechanism during later repair (TECH FIG 6B).1Recess the collateral ligaments off their origin on the proximal phalanx head for later repair. Before final implant placement, drill holes adjacent to the collateral ligament origin to allow suture passage for ligament repair (TECH FIG 6C).The volar plate is protected with the dorsal approach.The remaining portion of the procedure is similar to that described as part of the volar approach.P.1097
PEARLS AND PITFALLS
Indications ▪ Painless loss of motion is not an ideal indication; the operation does not reliably increase motion at long-term assessment.1. Osteoarthritis and posttraumatic arthritis are more common in the PIP joint than in the MCP joint.2. MCP arthroplasty has traditionally been performed for RA but has declined in frequency due to better control of disease in RA patients.3. PIP joint arthroplasty is helpful in maintaining motion in the ring and small fingers (for grip); PIP fusion is more acceptable in the index and long fingers (especially in workers) due to concerns of stability with pinch after arthroplasty.4. Avoid arthroplasty at both the MCP and PIP joints in one finger.Technique ▪ Broaching is carefully performed to avoid penetration of the cortex or rotation of the implant.5. Collateral ligament origin and insertion may be compromised with bone preparation; careful repair is performed.6. The dorsal approach is straightforward but requires careful protection of the central slip insertion.7. The volar approach minimizes the danger to the central slip and the extensor mechanism.8. The implant fit is carefully assessed. Buckling of the implant requires bony or soft tissue adjustments to increase space before final implant placement.Rehabilitation ▪ Motion is carefully progressed until joint encapsulation is complete.9. Rotation or deformity after arthroplasty may be corrected with dynamic splinting.
POSTOPERATIVE CARE
The patient is placed in a plaster splint after surgery for 3 to 5 days. The MCP and PIP joints are immobilized in extension.Some surgeons advocate 3 to 4 weeks of immobilization after MCP joint implant arthroplasty before the initiation of hand therapy.Early joint motion is important for appropriate joint encapsulation.An engaged hand therapist is crucial in obtaining a satisfactory surgical outcome.Early therapy emphasizes edema control and patient comfort through splinting. Subsequent therapy focuses on range of motion.MCP joint arthroplasty, especially in the rheumatoid patient, requires meticulous postoperative hand therapy.Dynamic extension (daytime) splints, static extension (nighttime) splints, or both are fabricated.The alignment and motion of the fingers are carefully monitored. Adjustments to the splints are commonlyrequired as the encapsulation process and the healing process progress. Active and gentle passive motion are progressively allowed.After PIP joint implant arthroplasty through a volar approach, the flexor and extensor mechanism need not be protected. Active and gentle passive motion may be initiated quickly, although the collateral ligament repairs should be protected for at least 6 weeks.Dynamic extension splinting may be used during the first 6 weeks.If the central slip was spared during a dorsal PIP joint approach and implant placement, early active motion is initiated with progression to gentle passive motion.If the approach for PIP implant arthroplasty required central slip takedown and repair, the extensor mechanism should be carefully protected during the rehabilitation period.
OUTCOMES
Pain is reliably improved in patients with MCP or PIP joint arthroplasty.2,3,4,5,6,7Most patients are improved functionally after silicone MCP arthroplasty. Patients with RA and a markedflexion and ulnar deviation posture of the MCP joints stand to benefit most.2,3 Although the arc of motion may be improved in the early postoperative period, at long-term follow-up the arc of motion is notdramatically increased; however, the arc is moved to a more extended and a more functional position.2,3 The ulnar drift of the MCP joints most commonly seen in RA is improved (although some recurrence in drift over time may also occur).2,3MCP arthroplasty for osteoarthritis can be expected to decrease pain and maintain or somewhat improve MCP range of motion and strength. In contrast to RA patients, MCP joint flexion may be increased in patients treated for osteoarthritis.2,5PIP arthroplasty will place the PIP joint in a more extended and functional posture but should not be expected to increase range of motion at long-term follow-up. Total joint motion depends on the preoperative motion but typically averages about 45 degrees. Pain relief is reliable for most patients nomatter the diagnosis.4,6,7PIP arthroplasty for RA may have a lesser outcome compared for PIP arthroplasty performed for posttraumatic arthritis or osteoarthritis. Patients with a boutonnière or swan-neck deformity are most likelyto be unchanged or worse in regard to their deformity.7PIP silicone implant survivorship decreases from 98% at 2 years to 80% at 10 years to 49% at 16 years (in a mixed population analysis).7
COMPLICATIONS
InfectionImplant fracture (which may or may not necessitate revision arthroplasty; if the encapsulated joint is stable, a fractured implant may be observed)Rotational malalignment Joint subluxationP.1098Silicone synovitisIn RA patients, recurrent ulnar drift may occur.
REFERENCES
- Chamay A. A distally based dorsal and triangular tendinous flap for direct access to the proximal interphalangeal joint. Ann Chir Main 1988;7:179-183.
- Goldfarb CA, Stern PJ. Metacarpophalangeal joint arthroplasty in rheumatoid arthritis: a long- term assessment. J Bone Joint Surg Am 2003;85-A(10):1869-1878.
- Kirschenbaum D, Schneider LH, Adams DC, et al. Arthroplasty of the metacarpophalangeal joints with use of silicone-rubber implants in patients who have rheumatoid arthritis. Long-term results. J Bone Joint Surg Am 1993;75(1):3-12.
- Lin HH, Wyrick JD, Stern PJ. Proximal interphalangeal joint silicone replacement arthroplasty: clinical results using an anterior approach. J Hand Surg Am 1995;20(1):123-132.
- Rettig LA, Luca L, Murphy MS. Silicone implant arthroplasty in patients with idiopathic osteoarthritis of the metacarpophalangeal joint. J Hand Surg Am 2005;30(4):667-672.
- Schneider LH. Proximal interphalangeal joint arthroplasty: the volar approach. Semin Arthroplasty 1991;2:139-147.
- Takigawa S, Meletiou S, Sauerbier M, et al. Long-term assessment of Swanson implant arthroplasty in the proximal interphalangeal joint of the hand. J Hand Surg Am 2004;29:785-795.
