DEFINITION
Complete transection of a peripheral nerve is defined as interruption of all of the axons within the nerve. Primary nerve repair is the tension-free reapproximation of severed nerve ends performed within a week of injury.Delayed primary repair is performed up to 3 weeks from injury when local soft tissue injuries do not permit primary wound closure.The healing of an injured peripheral nerve is different from the healing of other tissue types. Injury is followed by an immediate degeneration, followed by incomplete recovery.Irreversible changes in the motor and sensory end organs make timing of repair critical to achieve useful recovery.
ANATOMY
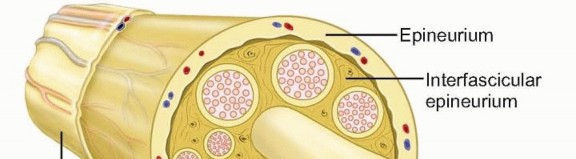
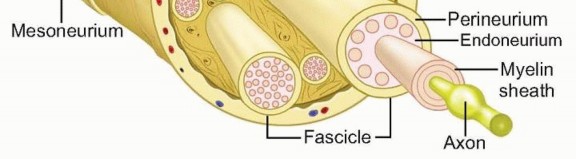
FIG 1 • Schematic of ultrastructure of the nerve. The smallest nerve unit visible to the naked eye is the nerve fascicle. Endoneurium. Delicate connective tissue that supports and surrounds each axonal fiber and associated Schwann cellsConsists of longitudinally arranged collagen fibrils and intrinsic blood vesselsPerineurium. The connective tissue that surrounds groups of axons, creating bundles referred to as fascicles.The fascicle is the smallest visible unit of the nerve at surgery.The fascicle is several layers thick and acts as a protective membrane and a barrier to diffusion.Epineurium. Surrounds groups of fascicles to form the superstructure of a peripheral nerveForms a sheath about the entire nerve and also supports the fascicular structure by passing between all the fasciclesForms 60% to 85% of the cross-sectional area of a peripheral nerveComposed on longitudinally oriented collagen fibers, fibroblasts, and intrinsic vesselsParaneurium or mesoneurium. Loose areolar tissue surrounding the epineurium Limited to the outer surface of the nerveLocation for the extrinsic vascular supply of the nerveMakes up the gliding apparatus of a peripheral nerveFascicles have a definite topographic arrangement within a peripheral nerve.Fascicular segregation into motor and sensory components is important when aligning a sectioned nerve before primary repair or nerve grafting.This concept of functional segregation allows for use of part of a donor healthy nerve for nerve transfer with minimal functional deficit.
PATHOGENESIS
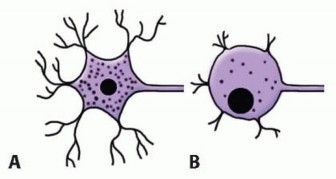
FIG 2 • Comparison of a normal neuron cell body (A) with that of a nerve after transection (B). Note cellular swelling, dissolution of Nissl granules in the cytoplasm, and retraction of the dendritic processes.
NATURAL HISTORY
Complete transection of a nerve results in retraction of the nerve ends. The nerve will not heal without surgical intervention to approximate the nerve ends.Wallerian degeneration occurs in the nerve segment distal to the level of transection.The axon distal to the injury degenerates and does not directly contribute to repair. The axonal and myelin debris are cleared by macrophages. Schwann cells proliferate, releasing nerve growth factors or neurotrophic factors. The distal stump does produce a complex protein, neurotropic factor, that attracts regenerating axons from the proximal stump.The cell body swells, Nissl granules in the cytoplasm diminish, and its dendritic processes retract. Several cells rupture and die, especially with more proximal nerve injuries (FIG 2).Regenerating axons sprout from the surviving axons and migrate toward the empty tubules in the degenerate distal stump at a rate of 1 to 3 mm per day.Proliferating Schwann cells myelinate the newly regenerated axons.In an unrepaired nerve, the random proliferation of axons from the proximal stump forms a tender mass of disorganized axons and fibrosis termed aneuroma.
PATIENT HISTORY AND PHYSICAL FINDINGS

FIG 3• Distribution of sensory loss with nerve injury.Yellow, median nerve;blue, ulnar nerve;pink, radial nerve.Perform the Froment sign test. The test is positive if paper is held by flexing the thumb interphalangeal (IP) joint, indicating recruitment of the flexor pollicis longus, which implies paralysis of the adductor pollicis from ulnar nerve injury.The thumb IP hyperextension test may indicate paralysis of the extensor pollicis longus due to posterior interosseous palsy.Perform the Tinel sign test. The test is positive if the patient notes a tingling sensation in the sensory distribution of the nerve. Serial progression of Tinel sign distally is useful to monitor axon progression after repair.When performing physical examinations, it is helpful to use motor function grading according to the Medical Research Council system. This grading allows for qualitative measurement of function and allows the clinician to chart recovery objectively:M0: no contractionM1: palpable contraction with only a flicker of motion M2: movement of the part with gravity eliminated M3: muscle contraction against gravityM4: ability to contract against moderate resistance M5: normal functionQuantitative measurements using grip and pinch strength dynamometers and comparing results to the contralateral normal side may also be useful.Sensory grading is also useful in evaluation. Sensory function is evaluated within the anatomic distribution of the nerve in question. Sensation is quantified using two complementary tests—(1) Semmes-Weinstein monofilaments, which measure innervation threshold, and (2) two-point discrimination, which measures innervation density. Vibratory, pain, and temperature sensation should also be evaluated. Semmes-Weinstein filaments demonstrate subtle and early sensory loss and are more useful in evaluation of compressive neuropathy. Two-point discrimination measurements help gauge the severity of nerve injury, with two-point discrimination of less than 12 mm indicating neurapraxic injury and readings greater than 15 mm suggesting complete disruption. Used together, the various sensory tests allow for qualitative measurement of function and allow for the clinician to objectively chart recovery:S0: lack of sensationS1: recovery of deep cutaneous pain sensibility within the autonomous area of the nerveS2: return of some degree of superficial cutaneous pain and tactile sensibility S3: return of function (S2) without evidence of hypersensibilityS3+: return of function (S3) with some return of two-point discrimination S4: normal functionSensory recovery classification on two-point discrimination alone:P.826Normal: less than 6 mm Fair: 6 to 10 mmPoor: 11 to 15 mm
IMAGING AND OTHER DIAGNOSTIC STUDIES
Diagnosis in acute injuries is usually based on history and clinical examination alone without need for additional investigations.Plain radiographs are of little use in evaluation of the nerves themselves but may be helpful in cases of injury from fracture or projectiles.Computed tomography (CT) myelography is useful for evaluation of injuries to the brachial plexus. Theformation of a pseudomeningocele is indicative of root avulsion.Magnetic resonance imaging (MRI) is useful for evaluation of peripheral injury but is not routinely indicated for peripheral nerve injuries.Short tau inversion recovery (STIR) MRI may show enhancement of the nerve near the site of injury or interruption of the nerve trunk on T1- and T2-weighted images.MRI provides visualization of pseudomeningoceles at the spinal cord levels in root avulsion injuries.Electrodiagnostic testingNerve conduction velocity (NCV) and electromyography (EMG) are useful in evaluation of closed nerve injuries, for example, after fracture or multiple nerve injuries such as brachial plexus injury.If stimulation distal to the suspected injury elicits a motor response about 3 days after injury, then the lesion is likely a conduction block. However, muscle action may be present in the case of complete transection for up to 9 days.Fibrillation potentials on EMG appear after 2 to 3 weeks and indicate muscle denervation and a severe grade nerve injury.Recovery is best evaluated with serial examination of compound muscle action potentials. Early recovery of only a few motor units may indicate reinnervation from adjacent intact nerves and should not be used as an indicator of recovery of the repaired nerve.
DIFFERENTIAL DIAGNOSIS
Muscle or tendon injury in open lacerations Parsonage-Turner syndrome (brachial plexus neuritis) Peripheral nerve entrapmentPartial nerve injury (neuroma in continuity)Neurapraxic injury (axonal dysfunction without discontinuity)
NONOPERATIVE MANAGEMENT
Nonoperative management of a completely transected nerve after an open injury is doomed to failure because cut ends retract and scar tissue forms in the gap.Pending recovery of the nerve, splinting of the paralyzed joint maintains functional position and range-of-motion exercises prevent contractures.Serial clinical examination and electrodiagnostic testing are helpful to evaluate recovery.
SURGICAL MANAGEMENT
Nerves that have been completely interrupted require surgical measures to restore continuity. All open injuries with neurologic impairment must be explored expeditiously.With closed injuries or delayed presentation, consider the overall functional capacity of the injured limb.In a largely motor nerve, for example, the radial nerve, tendon transfers may restore function more reliably than nerve repair.
PREOPERATIVE PLANNING
The cause of the peripheral nerve injury must be identified. The repaired nerve must have a favorable local environment if the repair is to be successful.Underlying fractures must be stabilized.Adequate soft tissue coverage of the nerve repair must be planned.Repair should be delayed when multiple débridements are necessary until the bed for the repaired nerve is optimal and wound can be primarily closed. If delayed repair is considered, the distal and proximal ends should be identified and tagged with a suture in the epineurium.Intraoperative nerve stimulation of motor or mixed (motor and sensory) nerves may assist with identification of the proximal and distal nerve stumps within the first 72 hours after injury. During this interval, residual neurotransmitters are present in the distal nerve and stimulation is still possible.If segmental loss is suspected, as with a crushing injury, the patient must give informed consent for additional options such as conduit repair or nerve grafting.Injuries that present late should be evaluated with electrophysiologic studies to look for signs of recovery.If intraoperative nerve stimulation is to be used, muscle relaxants should be avoided at induction of general anesthesia.If associated muscle or tendon lacerations are present, muscle relaxation facilitates their repair.Regional anesthetics such as supraclavicular block provide excellent muscle relaxation, and a supraclavicular catheter will help in administering postoperative analgesia. However, the motor blockade from the block will prevent the use of intraoperative nerve stimulation.
POSITIONING
The patient is positioned supine, with the arm positioned on a hand table.Use of a tourniquet facilitates dissection but will interfere with intraoperative nerve stimulation because it results in ischemic conduction blocks after 15 minutes.Use of intraoperative magnification (eg, loupes) for the dissection and a surgical microscope during nerve repair is essential.Microinstrumentation is needed for nerve handling and repair. Precise atraumatic dissection technique is necessary for optimal results.Alcoholic solutions should be avoided for the preparation of open wounds to avoid chemical damage to nerve tissue.P.827
TECHNIQUES
APPROACH

TECH FIG 1 • A. Freshening of a lacerated nerve end. The nerve is stretched over a sterile, moistened tongue depressor and cut using a sharp no. 11 scalpel. B. Sprouting fascicles must be seen at the cut surface of each nerve end before the repair.
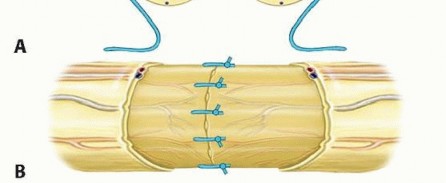
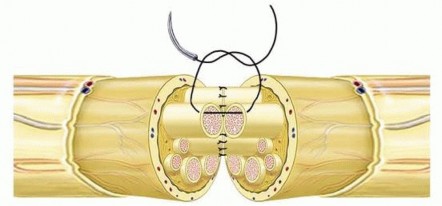
TECH FIG 2 • Steps of epineurial repair. A. The nerve ends are aligned, and two sutures are placed 180 degrees from each other. Tension across the repair is tested with two sutures. B. Additional sutures are placed in the epineurium.
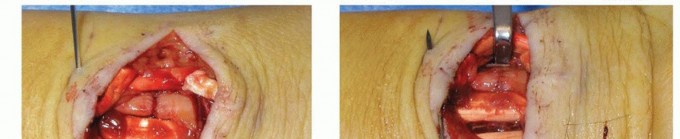

TECH FIG 3 • A. A laceration injury of the forearm, just proximal to the wrist. The palmaris longus tendon and the median nerve have been transected. B. Epineurial repair using interrupted, circumferential sutures.
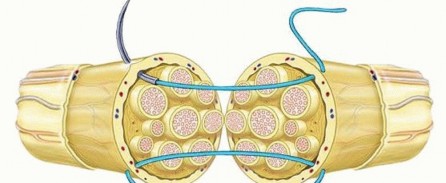
TECH FIG 4 • Technique of group fascicular repair. The epineurium is pulled back, and sutures are placed in the perineurium after fascicular groups have been aligned.
CABLE GRAFT REPAIR

TECH FIG 5 • Nerve grafting using “cables” of nerve graft. After aligning the nerve ends, similar fascicular groups are bridged with segments of nerve graft.
VASCULARIZED NERVE GRAFT REPAIR
CONDUIT REPAIR
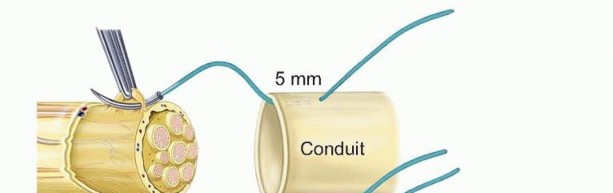
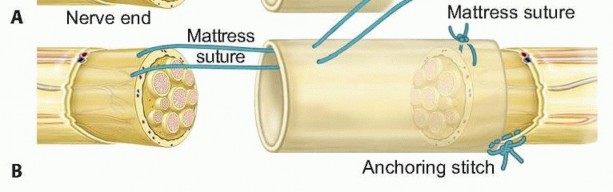
TECH FIG 6 • Technique of conduit repair. A. A horizontal mattress suture is placed between the conduit and the epineurium of the nerve. B. As the suture is tightened, the nerve is drawn into the conduit. A simple stitch is placed anchoring the epineurium to the tube opposite the location of the mattress suture.


TECH FIG 7 • A. Digital nerve injury with a 2-cm gap. The edges have been trimmed back to healthy fascicles. B. Nerve repair using a type I collagen conduit to bridge the gap between the nerve ends. Gently ease the nerve into the tube as the knot is tightened.Place a simple suture between the epineurium and the edge of the tube at a diametrically opposite point to anchor the tube and prevent rotation.Repeat the same steps for the distal stump and fill the tube with saline using a fine cannula (TECH FIG 7).6. Cadaver Allograft RepairAllograft repair is indicated in sensory, motor, and mixed nerve injuries with gaps up to 50 mm.Previous allografts required immunosuppression to prevent graft-versus-host disease and rejection. The immunosuppression was only necessary until adequate host Schwann cells migrated across the graft (usually approximately 24 months). Common immunosuppressants (tacrolimus) have been shown toaugment neuroregeneration.Modern allografts are acellular and must be repopulated with recipient Schwann cells from the proximal nerve stump. Autograft is already populated with autogenous Schwann cells, making autograft a superior graft material. Once the nerve ends are prepared, the nerve diameter at the proximal and distal stumps and the defect length are measured.Acellular allograft comes in varying diameters (1 to 5 mm) and various lengths (15 to 70 mm). As with nerve autograft, a graft slightly longer than the measured defect should be chosen to allow a tension-free repair.After the appropriately sized graft is chosen, the graft should be thawed using room temperature saline until it is soft and pliable (5 to 10 minutes).The allograft should be sutured into position using an epineurial suture technique as described earlier (see TECH FIG 2A,B). Cable grafting with allograft can also be used for larger nerves (see TECH FIG 4).P.8317. Nerve TransfersNerve transfers are indicated in devastating or chronic nerve injuries that are not amenable to primary reconstructive strategies. For example, in the cases of high (proximal) nerve injuries with complete axonal loss and wallerian degeneration, primary reconstructive strategies require the nerve to regenerate from the proximal stump, across the reconstructed gap, and distal to the motor endplates or sensory distribution of the nerve. This regeneration is slow (approximately 1 to 3 mm per day) and may not result in motor endplate reinnervation prior to muscle atrophy.With greater understanding of motor and sensory nerve topography, expendable donor nerves have been identified. Multiple donor nerves have been described and catalogued, offering several options for particularly troublesome nerve deficits.Keys to nerve transfer surgery include the following: Wide exposure.Precise understanding of the internal topography of the donor and recipient nerves. Transfer oftenrequires intrafascicular dissection of the donor and recipient nerve from the main trunk. Use of a nerve stimulator greatly assists in this technique so be mindful of muscle relaxants and tourniquet palsy during these procedures.Meticulous dissection technique.Use of a microscope and microsurgical instruments is recommended.Iatrogenic injury to the main trunk of the donor nerve may lead to significant morbidity.Tension-free transfer. When designing the transfer, remember “donor distal” and “recipient proximal.” The donor nerve should be dissected as distal as possible and the recipient nerve as proximal as possible to allow easy transposition and tension-free repair. If possible, the repair should be lax enough to allow passive range of motion of adjacent joints as well. Often, nerve transposition is required to allow free joint motion without compromising the repair.End-to-end repair. Although end-to-side transfers have been described, end-to-end repair is preferable.
PEARLS AND PITFALLS
Intraoperativeprecautions1. If contemplating intraoperative nerve stimulation, avoid muscle relaxants andtourniquets.2. Repair bones and tendons before undertaking fragile nerve repair.3. Proceed with nerve repair only if the wound bed is clean and healthy and primary closure is possible.4. If delayed repair is planned, place a marking suture in the epineurium to facilitate later identification.Nerveprecautions1. Limit handling of nerve and use microsurgical instruments.2. Use operating microscope to prepare nerve ends and for fascicular alignment.3. Always be prepared to use graft or conduit rather than suture nerve under tension or with joints excessively flexed.4. Keep nerves (including grafts) moist.5. Repair should be tension free.6. Soft tissue coverage is a must.Instrumentation1. Make certain that microinstrumentation is in good repair.2. Forceps should be free of spurs and should approximate correctly.3. Use 8-0 or 9-0 suture with atraumatic taper-point needles.
POSTOPERATIVE CARE
Consider use of a local anesthesia infusion pump for postoperative pain control. Immobilization is very important to prevent tension across the repair:The elbow should be held at 90 degrees of flexion.Wrist flexion greater than 20 degrees should be avoided.The metacarpophalangeal joints should be held at 70 degrees of flexion.Mobilization varies with associated tendon repair. After isolated nerve repair, gentle finger flexion and shoulder range of motion are started soon after surgery to promote nerve gliding and prevent finger stiffness.Remove skin sutures after 2 weeks and replace the splint.For nerve repairs around the elbow, allow motion in an extension-blocking splint. Full extension is permitted after 6 weeks.For repairs in the distal forearm and wrist level, immobilize the wrist at 20 degrees flexion and block metacarpophalangeal hyperextension for 4 weeks. Allow active finger motion within the splint. Bring the wrist to neutral at 4 weeks, and then allow mobilization out of the splint at 6 weeks.Nerve regeneration is followed at regular intervals with clinical examination of motor and sensory recovery and Tinel sign.The distal most point at which the Tinel sign is observed is recorded at each visit and its distance from the suture line noted.Expect distal progression of Tinel sign at the rate of about 1 mm per day, with a delay of 1 month after the date of repair.Failure of Tinel progression over serial visits may indicate repair failure: Consider reexploration and grafting.Sensory reeducation is initiated early in the postoperative phase with the goal of teaching recognition of new input in a useful manner.P.832Three stages to this process are introduced sequentially in the recovery period:Desensitization: The patient is presented with graded stimuli to decrease unpleasant sensations.Early-phase discrimination and localization: The patient works with static and moving touch, using visual reinforcement.Late-phase discrimination and tactile gnosis: The patient works with varying shaped objects.Until motor recovery has occurred, regular range-of-motion exercises should continue to prevent joint stiffness or contractures. Strengthening exercises are slowly added after return of voluntary motor function.After nerve transfer surgery, the patient must adapt to a new neural pathway from the cerebral cortex. Motor reeducation involves prescribed exercises using voluntary simultaneous contracture of the donor and recipient muscles.
OUTCOMES
The outcome after nerve repair is generally less favorable than that of repair of other tissues, such as bone or tendon injury.It is difficult to predict the outcome because of several variables, including type of nerve (pure sensory vs. mixed), age of patient, and type of injury—clean or crushed, associated soft tissue injuries.The single most important factor that correlates with outcome is patient age. The best results are seen in children younger than 10 years of age.Pure motor or pure sensory nerves fare better than mixed nerves.The outcome also correlates with level of injury. Injuries closer to the end organs fare better because there is less distance for the regenerating axons to cover.Peripheral factors that are determined by the injury and cannot be modified by the treating surgeon include axonal cell death, end organ atrophy, and extensive scarring from surrounding crush injury.The surgeon can control, to a limited extent, the scarring in and around the nerve repair.Central factors that account for poor results include cortical remapping and reorganization, with reduced and disorganized cortical representation of denervated areas.Children recover greater function than their adult counterparts with primarily repaired lesions at similar levels due to a combination of better axonal regeneration and cortical plasticity.Delayed repairs fare worse than those repaired acutely, with an estimated 1% decrease in performance for every 6 days of delay in the repair.The nature of the injury often determines the likelihood of recovery. Massive soft tissue injury or burns involving a peripheral nerve are less likely to regain function than injuries involving sharp or limited transection of a nerve.Median nerve outcome after high injuries usually is poor because of hand intrinsic atrophy. After low injuries, useful motor function is regained in 40% to 90% of repairs and useful sensation is restored in 53% to 100% of patients.Ulnar nerve injuries show similarly poor results for motor recovery, with functional restoration in 35% of cases and functional sensory recovery in 30% to 68% of cases.Because the radial nerve is largely a motor nerve, better results can be expected after acute radial nerve repairs, with functional return in 60% to 75% of patients. Poor results are noted with high injuries, however.After repair of digital nerves, about 50% of patients regain static two-point discrimination of less than 10mm. Younger children demonstrate near-normal sensory recovery due to their cortical adaptability.Conduit repair appears superior to primary end-to-side repair in digital nerve reconstruction with gaps less than 4 mm (excellent sensory recovery in 91% vs. 49%) and to standard nerve grafting in digital nerve gaps greater than 8 mm (excellent sensory recovery 42% vs. 0%).Lingering symptoms of hypersensitivity and cold intolerance are common with sensory nerve injury in the upper extremity, resolving in most patients after 2 to 3 years. The cause is unclear.Complex regional pain syndrome is more likely to be present after untreated nerve injuries. If it does occur, significant joint contractures and atrophic changes can result and the patient generally has a prolonged recovery period and a poor outcome.
COMPLICATIONS
Causes for failure of repair include the following: Tension on the initial repairAn unfavorable local tissue environment with excessive scarringNoncompliance with protective measures or therapy and consequent joint contracturesPainful neuromas usually form in unrepaired or poorly repaired nerves close to the surface. These usually are treated with desensitization, local padding, and so forth because surgical results are often disappointing.Altered sensation is a result of axonal misdirection and cortical misrepresentation and can present as loss of temperature sensation or cold intolerance, hyperesthesia, or neuropathic pain.Some amount of altered function is inevitable after all complete nerve injuries in the upper extremity except in young children. It is due to a combination of altered sensation and proprioception along with loss of motor strength.Complex regional pain syndrome type II can occur after nerve injury especially in untreated cases or after delayed treatment or failure to control pain. Typical features include dramatic changes in the color and temperature of the skin accompanied by intense burning pain, skin sensitivity, sweating, and swelling.Early recognition is the key with referral to a pain management specialist for stellate blocks along with steroids, antiepileptic drugs, and therapy.
SUGGESTED READINGS
- al-Ghazal SK, McKiernan M, Khan K, et al. Results of clinical assessment after primary digital nerve repair.J Hand Surg Br 1994;19:255-257.
- Birch R. Nerve repair. In: Green DP, Hotchkiss RN, Pederson WC, et al, eds. Green's Operative Hand Surgery, ed 5. Philadelphia: Elsevier Churchill Livingstone, 2005:1075-1112.
- Birch R, Bonney C, Wynn Parry CB. Surgical Disorders of the Peripheral Nerves. Edinburgh: Churchill Livingstone, 1998.
- Birch R, Raji AR. Repair of median and ulnar nerves. Primary suture is best. J Bone Joint Surg Br 1991;73(1):154-157.
- Brown JM, Mackinnon SE. Nerve transfers in the forearm and hand. Hand Clin 2008;24:319-340.P.833
- Chaise F, Friol JP, Gaisne E. Results of emergency repair of wounds of palmar collateral nerves of the fingers [in French]. Rev Chir Orthop Reparatrice Appar Mot 1993;79:393-397.
- Cho MS, Rinker BD, Weber RV, et al. Functional outcome following nerve repair in the upper extremity using processed nerve allograft. J Hand Surg Am 2012;37(11):2340-2349.
- Clark WL, Trumble TE, Swiontkowski MF, et al. Nerve tension and blood flow in a rat model of immediate and delayed repairs. J Hand Surg Am 1992;17:677-687.
- de Medinaceli L, Prayon M, Merle M. Percentage of nerve injuries in which primary repair can be achieved by end-to-end approximation: review of 2,181 nerve lesions. Microsurgery 1993;14: 244-246.
- Giddins GE, Wade PJ, Amis AA. Primary nerve repair: strength of repair with different gauges of nylon suture material. J Hand Surg Am 1989;14:301-302.
- Goldberg SH, Jobin CM, Hayes AG, et al. Biomechanics and histology of intact and repaired digital nerves: an in vitro study. J Hand Surg Am 2007;32:474-482.
- Goldie BS, Coates CJ, Birch R. The long term result of digital nerve repair in no-man's land. J Hand Surg Br 1992;17:75-77.
- Hudson DA, de Jager LT. The spaghetti wrist. Simultaneous laceration of the median and ulnar nerves with flexor tendons at the wrist. J Hand Surg Br 1993;18:171-173.
- McAllister RM, Gilbert SE, Calder JS, et al. The epidemiology and management of upper limb peripheral nerve injuries in modern practice. J Hand Surg Br 1996;21:4-13.
- Parry CB, Salter M. Sensory re-education after median nerve lesions. Hand 1976;8:250-257.
- Puckett CL, Meyer VH. Results of treatment of extensive volar wrist lacerations: the spaghetti wrist. Plast Reconstr Surg 1985;75:714-721.
- Shergill G, Bonney G, Munshi P, et al. The radial and posterior interosseous nerves. Results of 260 repairs. J Bone Joint Surg Br 2001;83:646-649.
- Sullivan DJ. Results of digital neurorrhaphy in adults. J Hand Surg Br 1985;10:41-44.
- Weber RA, Breidenbach WC, Brown RE, et al. A randomized prospective study of polyglycolic acid conduits for digital nerve reconstruction in humans. Plast Reconstr Surg 2000;106:1036-1045.
