INTRODUCTION TO REPLANTATION SURGERY
The successful replantation of amputated digits, hands, and upper extremities represents one of the most demanding challenges in operative orthopedics and microsurgery. Achieving not merely tissue survival, but meaningful functional recovery, requires a profound understanding of vascular anatomy, biomechanics, and meticulous surgical sequencing. The preparation phase—encompassing patient optimization, ex vivo dissection of the amputated part, and proximal stump management—dictates the trajectory of the entire procedure.
This comprehensive guide delineates the evidence-based protocols for replantation preparation, establishing a standardized yet adaptable order of repair designed to minimize ischemia time, prevent venous congestion, and ensure tension-free neurovascular anastomoses.
PREOPERATIVE PREPARATION AND ANESTHESIA
The physiological optimization of the patient and the surgical environment is paramount. Replantation is often a marathon procedure, necessitating rigorous attention to patient comfort, core temperature maintenance, and hemodynamic stability.
Anesthetic Considerations
The choice of anesthesia profoundly impacts both intraoperative hemodynamics and postoperative graft survival.
* Regional Anesthesia: For most adults and older children undergoing digital or hand replantation, an axillary brachial plexus block utilizing a long-acting local anesthetic (e.g., bupivacaine) is the gold standard. Beyond providing excellent intraoperative and postoperative analgesia, regional blocks induce a profound sympathetic blockade. This pharmacological sympathectomy results in peripheral vasodilation, maximizing arterial inflow and mitigating vasospasm at the anastomotic sites.
* General Anesthesia: General anesthesia is frequently preferable, and often mandatory, for proximal amputations (forearm and arm level), in younger or highly anxious children, or during prolonged surgeries involving multiple digits or bilateral amputations.
Patient Positioning and Environmental Control
- Thermoregulation: Hypothermia is a potent trigger for peripheral vasoconstriction, which can be catastrophic for microvascular anastomoses. The operating table must be heavily padded, and forced-air warming blankets should be applied to maintain normothermia throughout the prolonged surgical duration.
- Tourniquet Application: A pneumatic tourniquet is essential to provide a bloodless field during the initial dissection of the proximal stump and to control subsequent significant bleeding. The tourniquet should be padded and applied high on the arm.
- Stump Preparation: Once the patient is anesthetized and comfortable, the proximal stump is thoroughly cleansed with an antiseptic solution (typically povidone-iodine) and meticulously irrigated with normal saline to remove gross contaminants before formal surgical debridement begins.
Clinical Pearl: Never use chlorhexidine solutions near exposed peripheral nerves, as it is highly neurotoxic. Copious irrigation with normal saline remains the safest and most effective method for mechanical debridement of the stump.
MICROSURGICAL DISSECTION OF THE AMPUTATED PART
While the patient is being prepped and anesthetized, a second surgical team—led by a hand surgeon with advanced microsurgical training—simultaneously prepares the amputated part on a sterile back table. This ex vivo dissection is critical for identifying and tagging structures, thereby minimizing warm ischemia time once the part is brought to the surgical field.
Surgical Approaches and Exposure
The approach to the structures of the amputated part must allow for extensive, atraumatic exposure.
* Incisions: Mid-axial incisions on the radial and ulnar aspects of the digit are standard. These incisions allow for the reflection of full-thickness dorsal and palmar flaps, providing panoramic access to the neurovascular bundles, flexor tendon sheath, and extensor mechanism.
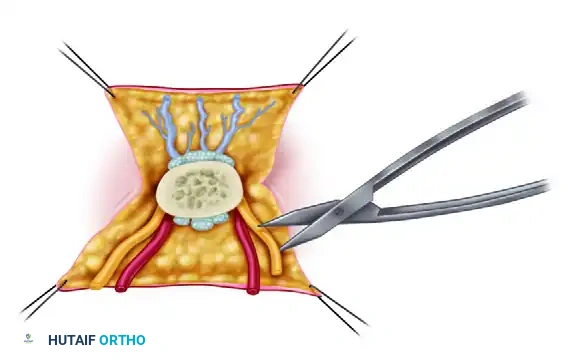
- Structure Identification: Using magnifying loupes or an operating microscope, the surgeon employs meticulous technique to identify the arteries, veins, and nerves.
- Tagging: Small structures are highly susceptible to retraction and loss within the soft tissue planes. They must be carefully preserved and tagged with 8-0 or 9-0 nylon sutures. This ensures they can be rapidly located for nerve repair and vascular anastomoses later in the procedure. Tendons are dissected and secured with 4-0 nylon sutures.
Surgical Warning: Avoid grasping the intima or the cut ends of the vessels with forceps during dissection. Crush injury to the endothelium will inevitably lead to localized thrombosis and failure of the replant. Handle vessels only by their adventitia.
VASCULAR ASSESSMENT AND EX VIVO PERFUSION
The mechanism of injury—sharp laceration versus crush or avulsion—dictates the extent of vascular preparation required.
Sharp Amputations
If the amputation is clean and sharp (e.g., guillotine-type injury from a paper cutter or saw), the zone of injury is narrow. In these instances, ex vivo perfusion of the digital arteries prior to anastomosis is usually unnecessary and may risk iatrogenic intimal damage.
Crush and Avulsion Injuries
Crush and avulsion injuries present a much wider zone of trauma. Evidence of distal injury may manifest as ecchymoses along the neurovascular bundles, adventitial abrasions, or skip lacerations.
In these complex scenarios, the vascular tree must be interrogated and cleared:
1. Cannulation: Gently cannulate the digital artery using a small Silastic catheter.
2. Perfusion: Perfuse the vascular tree with a heparinized Ringer's lactate or normal saline solution (typically 100 units of heparin per mL).
3. Prognostic Assessment: Observe the venous outflow. If there is no return of the perfusate, or if the fluid extravasates from distally injured vessels, the microvascular bed is likely destroyed. In such cases, blood flow is highly unlikely to be maintained after anastomosis, and replantation may be contraindicated.
4. Metabolite Clearance: For major limb amputations (hands, forearms, arms), brief periods of perfusion are highly beneficial for flushing stagnant blood, microthrombi, and toxic anaerobic metabolites (lactic acid, potassium) from the vascular tree, thereby reducing the risk of systemic reperfusion injury.
THE STANDARDIZED ORDER OF REPAIR
After all structures in both the amputated part and the proximal stump have been thoroughly cleansed, aggressively debrided, and clearly identified, the formal repair begins. While certain clinical circumstances dictate variations, the following represents the universally accepted, biomechanically optimized order of repair.
1. Bone Shortening and Osteosynthesis
Bone shortening is the foundational step of replantation. It is an absolute prerequisite for achieving tension-free vascular and neural anastomoses.
* Shortening: Although multiple interpositional vein grafts can be utilized to bridge vascular gaps, it is standard practice to shorten the bone. Shortening is usually performed on the side of the amputation (proximal or distal) that has the most bone to spare. In digital replantations, this shortening rarely exceeds 1 cm to preserve intrinsic muscle balance and joint kinematics.
* Fixation Techniques: Rigid, low-profile internal fixation is required. We typically insert a longitudinal Kirschner wire (K-wire) combined with an obliquely crossing K-wire to provide rotational stability. Occasionally, intraosseous wiring (90-90 wiring) is utilized near metaphyseal regions or joints. Plates and screws are generally avoided in digital replantation due to their bulk, which can compromise soft tissue closure and impinge on the delicate vascular repairs.
* Arthrodesis: If the amputation has occurred directly through a joint, or if the extensor mechanism is deemed irreparable, primary arthrodesis should be prepared and executed at this stage.
2. Extensor Tendon Repair
Repairing the extensor tendons immediately after osteosynthesis provides additional stability to the skeletal fixation. It is performed using non-absorbable sutures (e.g., 4-0 or 5-0 core sutures) utilizing a figure-of-eight or modified Kessler technique. Repairing the dorsal structures first prevents the need to flip the hand later, which could jeopardize delicate volar vascular repairs.
3. Flexor Tendon Repair
Flexor tendon repair follows the extensor repair.
* Sequencing Note: Steps 2 and 3 may be reversed depending on the surgeon's preference and the exact level of injury.
* Delayed Repair: In cases of severe crush injury, massive contamination, or prolonged ischemia time where establishing blood flow is critical, flexor tendon repair may be intentionally delayed and performed as a secondary reconstructive procedure weeks later.
4. Arterial Anastomosis
Establishing arterial inflow is the most critical step for tissue survival.
* Preparation: Before initiating reattachment, the proximal arterial stumps must be freed of any intraluminal clots. The tourniquet is temporarily deflated to assess pulsatile flow. The stumps are opened to allow free arterial bleeding, which flushes out microthrombi.
* Resection to Healthy Tissue: If satisfactory, brisk flow cannot be achieved, the vessel is likely suffering from intimal damage or severe vasospasm. Additional proximal dissection and aggressive vessel resection back to healthy, uninjured intima under the microscope is mandatory.
* Vein Grafting: If resection results in a gap that cannot be closed without tension, interpositional vein grafts (typically harvested from the volar forearm or dorsal foot) must be utilized. Never perform a microvascular anastomosis under tension.
5. Nerve Repair
Primary neurorrhaphy is performed using 8-0 or 9-0 nylon epineurial sutures.
* Timing Variation: If ischemia time permits, it is often technically easier to repair the digital nerves just before repairing the digital arteries. The nerves lie deep to the arteries in the volar surgical field; repairing them first prevents the surgeon from having to manipulate or retract the newly anastomosed, fragile artery to access the nerve.
6. Venous Anastomosis
Venous outflow must be established to prevent catastrophic venous congestion. A general rule is to repair two veins for every one artery anastomosed, if anatomically feasible.
* Timing Variation (The "Dorsal First" Approach): If ischemia time is well within safe limits, many microsurgeons prefer to repair the veins immediately after the extensor tendon repair (Step 2).
* Rationale: This allows all dorsal work (extensors and veins) to be completed in a bloodless field before the hand is supinated to address the volar structures. It minimizes repositioning of the hand, protects the venous anastomoses from disruption, and significantly reduces venous congestion once arterial inflow is established.
7. Soft Tissue Coverage and Wound Closure
The final step is meticulous, tension-free wound closure.
* Fasciotomy: In major limb replantations, or digits with significant crush components, prophylactic fasciotomies are highly recommended to prevent compartment syndrome secondary to reperfusion edema.
* Coverage: Skin must never be closed under tension over vascular repairs. If primary closure is not possible, split-thickness skin grafts or local rotational flaps should be employed immediately to cover exposed vessels and nerves.
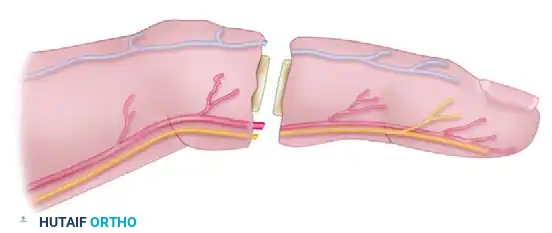
SPECIAL ANATOMIC CONSIDERATIONS: DISTAL THUMB AMPUTATIONS
Amputations of the distal thumb present unique anatomical challenges due to the arborization of the vascular tree.
* In these distal injuries, it is often technically advantageous to anastomose interpositional vein grafts to the terminal branch of the ulnar digital artery and the largest dorsal vein before performing osteosynthesis.
* Because the vessels at this level are exceptionally small, performing the proximal anastomoses of the vein grafts more proximally on the dorsum of the thumb—proximal to the zone of injury—can significantly improve patency rates. Careful, gentle, and meticulous dissection is required to locate these terminal branches.
POSTOPERATIVE PROTOCOLS AND MONITORING
The success of a replantation extends far beyond the operating room. Postoperative management is critical to prevent late thrombosis and ensure functional recovery.
- Monitoring: The replanted part must be monitored hourly for the first 48-72 hours. Clinical assessment includes skin color, capillary refill time, tissue turgor, and temperature monitoring (a drop of >2°C compared to an adjacent normal digit is highly indicative of vascular compromise).
- Anticoagulation: Protocols vary by institution, but typically include intravenous dextran, subcutaneous heparin, or oral aspirin to modulate thrombogenesis. Leeches (Hirudo medicinalis) may be employed for isolated venous congestion.
- Environment: The patient's room should be kept warm. Smoking, caffeine, and chocolate are strictly prohibited, as they induce severe peripheral vasoconstriction.
- Rehabilitation: Early, protected passive motion protocols, guided by a specialized hand therapist, are initiated once the vascular status is deemed stable (usually within 3 to 7 days) to prevent tendon adhesions and joint contractures.
