INTRODUCTION TO PYOGENIC FLEXOR TENOSYNOVITIS
Pyogenic flexor tenosynovitis (PFT) represents a true orthopedic emergency, characterized by a rapidly progressive bacterial infection within the closed fibro-osseous space of the digital flexor tendon sheath. The accumulation of purulent exudate within this unyielding synovial space leads to a rapid increase in hydrostatic pressure. This pressure not only causes severe pain—classically described by Kanavel's four cardinal signs—but also compromises the delicate microvascular perfusion to the flexor tendons supplied by the vincula brevia and longa.
If left untreated, or if inadequately decompressed, the ensuing ischemia and enzymatic degradation from bacterial collagenases will result in irreversible tendon necrosis, catastrophic adhesion formation, and profound loss of hand function.
Postoperative closed irrigation, popularized and refined as the modified Neviaser technique, remains a cornerstone in the surgical management of acute PFT. By establishing a proximal-to-distal fluid gradient through the tendon sheath, the surgeon can mechanically wash out bacterial load, inflammatory cytokines, and destructive enzymes while preserving the critical biomechanical integrity of the annular pulley system.
INDICATIONS AND PATIENT SELECTION
The decision to utilize closed postoperative irrigation versus radical open debridement depends heavily on the chronicity of the infection and the intraoperative macroscopic appearance of the tendon and synovial fluid.
Favorable Indications for Closed Irrigation
Closed postoperative irrigation is highly appropriate and clinically effective for:
* Acute Infections: Presentations within 24 to 48 hours of symptom onset or penetrating trauma.
* Michon Stage I and II Infections:
* Stage I: The sheath contains cloudy, serous, or serosanguineous exudate, but the synovium is merely hyperemic.
* Stage II: The sheath contains frankly purulent fluid, but the flexor tendon remains viable, glistening, and structurally intact.
Contraindications (Indications for Open Drainage)
Closed catheter irrigation is contraindicated, and open drainage becomes mandatory, under the following conditions:
* Michon Stage III Infections: The flexor tendon is grossly necrotic, dull, fragmented, or the surrounding pulley system is destroyed.
* Chronic Infections: Delayed presentations where loculated abscesses or extensive fibrinous adhesions prevent the free flow of irrigant through the sheath.
* Atypical Pathogens: Mycobacterial or fungal tenosynovitis, which typically require extensive open synovectomy rather than simple irrigation.
💡 Clinical Pearl: The Lille et al. Controversy
While postoperative closed irrigation has been the gold standard for decades, modern literature presents a nuanced view. Lille et al. demonstrated no statistically significant differences in long-term functional outcomes between patients who received exhaustive intraoperative irrigation alone versus those who underwent continuous postoperative irrigation for 24 to 48 hours. However, for heavily contaminated sheaths or delayed presentations (without frank necrosis), leaving an irrigation system in place provides a reliable safety net against recurrent purulence.
SURGICAL ANATOMY AND BIOMECHANICS
A profound understanding of the synovial sheaths is required to successfully execute this procedure without causing iatrogenic injury.
The flexor tendon sheaths of the index, middle, and ring fingers typically extend from the neck of the metacarpal (just proximal to the A1 pulley) to the insertion of the flexor digitorum profundus (FDP) at the distal phalanx.
Conversely, the synovial sheath of the thumb (radial bursa) and the small finger (ulnar bursa) frequently communicate proximally at the level of the carpal tunnel (Parona's space). An infection in the small finger can rapidly track into the thumb, creating the dreaded "horseshoe abscess." In such cases, the irrigation system must be modified to address these proximal bursal extensions.
PREOPERATIVE PREPARATION
Anesthesia and Positioning
- Anesthesia: The procedure must be performed under suitable regional anesthesia (axillary or supraclavicular brachial plexus block) or general anesthesia. Local infiltration alone is strictly contraindicated due to the risk of spreading the infection and the inability to achieve adequate proximal exposure.
- Positioning: The patient is positioned supine with the affected arm extended on a radiolucent hand table.
The Tourniquet Rule
- Preparation: The hand and arm are appropriately prepped and draped using standard sterile orthopedic protocols.
- Tourniquet Inflation: A pneumatic tourniquet is applied to the proximal arm and inflated to 250 mm Hg (or 100 mm Hg above systolic pressure).
🚨 Surgical Warning: Do Not Exsanguinate
To critically reduce the risk of mechanically disseminating the localized pyogenic infection into proximal, uninvolved fascial planes, do not wrap the limb with an Esmarch bandage. Instead, simply elevate the arm for 3 to 5 minutes to allow venous drainage via gravity before inflating the tourniquet.
SURGICAL TECHNIQUE: MODIFIED NEVIASER CLOSED IRRIGATION
Step 1: Proximal Exposure (The A1 Pulley)
The goal of the proximal incision is to access the membranous portion of the flexor sheath just proximal to the A1 pulley.
- Make a straight transverse incision parallel to the distal palmar crease, or alternatively, utilize a zigzag (Bruner) incision directly over the A1 pulley region.
- Carefully dissect through the subcutaneous tissue, identifying and protecting the digital neurovascular bundles, which lie volar and adjacent to the flexor sheath.
- Retract the neurovascular bundles to expose the proximal end of the flexor sheath.
- Upon visualization, expect to see the sheath bulging under tension. You will likely observe serosanguineous or purulent fluid visible through the translucent synovial membrane.
Step 2: Sheath Decompression and Culture
- Make a small transverse or V-shaped window in the membranous sheath immediately proximal to the A1 pulley.
- As the fluid is released, immediately swab the purulent or serous exudate and send it for urgent aerobic, anaerobic, and acid-fast bacilli (AFB) cultures, as well as Gram staining.
Step 3: Distal Exposure (The A4 Pulley)
To establish an outflow tract, the distal sheath must be opened.
- Make a second incision in the midaxial line on either side of the finger, located in the distal portion of the middle segment of the digit.
- Alternative Approach: Carefully make a transverse incision directly over the distal interphalangeal (DIP) flexion crease.
- Dissect down to the fibro-osseous canal and identify the A4 pulley.
- Open the flexor sheath immediately distal to the A4 pulley. Ensure the FDP tendon insertion is not compromised.
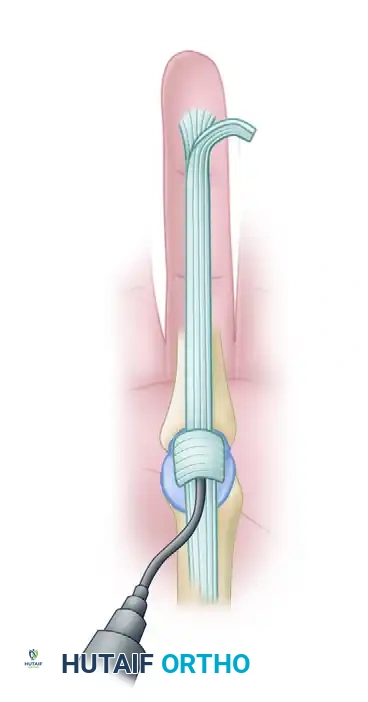
Step 4: Catheter Insertion and Routing
The irrigation system relies on a proximal-to-distal flow to flush debris out of the dependent distal wound.
- Using smooth forceps or a fine hemostat, carefully pass a 16-gauge or 18-gauge polyethylene catheter (a pediatric feeding tube or a dedicated epidural catheter may also be used) beneath the A1 pulley.
- Advance the catheter from proximal to distal within the flexor sheath for a distance of exactly 1.5 to 2 cm. Do not advance it further, as a catheter that is too long can cause mechanical pressure necrosis on the underlying tendon.

- Distally, place a small piece of a sterile rubber drain (e.g., a Penrose drain sliver) beneath the A4 pulley, bringing it out through the distal skin incision to maintain patency of the outflow tract.
- Using a syringe, forcefully irrigate the sheath from proximal to distal with sterile normal saline to clear immediate debris and verify that fluid flows freely out of the distal wound.
Step 5: Closure and System Testing
- Close the proximal palmar wound loosely around the inflow catheter using non-absorbable monofilament sutures (e.g., 4-0 Nylon).
- Suture the catheter securely to the palmar skin to prevent inadvertent dislodgment during postoperative mobilization.
- Close the distal wound around the rubber drain, ensuring it is left sufficiently loose to allow unimpeded fluid drainage. A tight distal closure will lead to iatrogenic compartment syndrome of the digit.
- Test the system for patency one final time by irrigating freely with saline.
Step 6: Dressing Application
- Wrap the hand in a bulky, non-compressive soft dressing supported by a volar resting splint (wrist in 20° extension, MCP joints in 70° flexion, IP joints in full extension).
- Leave the tip of the distal rubber drain exposed through the dressing to allow nursing staff to observe the outflow.
- Bring the proximal inflow catheter out through the dressing, tape it securely to the outer bandage, and attach it to a sterile 30-mL syringe or a continuous gravity-drip IV tubing system.
MANAGEMENT OF BURSAL INVOLVEMENT (RADIAL AND ULNAR BURSAE)
When the infection involves the thumb or small finger, the surgeon must assume potential involvement of the radial or ulnar bursa, respectively.
- Palmar Catheter: Place a second catheter in the proximal palmar wound and pass it proximally into the sheath, securing it to the palmar skin with a suture.
- Forearm Decompression: Open the respective bursa proximally through a longitudinal incision on the radial or ulnar side of the distal forearm, just proximal to the wrist crease.
- Drain Placement: Place a piece of rubber drain into the opened bursa in the forearm and bring it out through the skin.
- Bidirectional Irrigation: For these combined digital and bursal infections, the surgeon must irrigate in both proximal and distal directions to ensure complete clearance of the horseshoe pathway.
OPEN DRAINAGE FOR ADVANCED INFECTION
If, upon opening the sheath, the flexor tendon is found to be grossly necrotic, fragmented, or if the infection is highly chronic with thick loculations, closed irrigation will fail.
In these Michon Stage III scenarios, open drainage is strictly necessary. The entire flexor sheath must be exposed, often requiring the sacrifice of non-essential pulleys, extensive tenosynovectomy, and potentially staged tendon reconstruction if the FDP is non-viable.
🔪 Surgical Pitfall: Missed Necrosis
Attempting closed irrigation on a necrotic tendon will result in persistent sepsis, delayed healing, and eventual rupture of the tendon. If the tendon lacks its normal pearly-white, glistening appearance, abandon the closed technique and proceed to open debridement.
POSTOPERATIVE CARE AND REHABILITATION PROTOCOL
The success of the modified Neviaser technique relies heavily on meticulous postoperative ward care.
Irrigation Schedule
- Volume and Frequency: The wounds are irrigated with 30 mL of sterile normal saline every 2 hours. Alternatively, a continuous gravity drip can be set at 10 to 15 mL per hour.
- Monitoring: During each flush, the wound at the distal end of the finger must be checked for catheter patency and the free flow of the irrigant. If resistance is met, the catheter may be kinked or blocked by fibrinous debris, requiring immediate attention.
48-Hour Evaluation
- After 48 hours of continuous or intermittent irrigation, the bulky dressing is removed in a sterile environment so that the fingers can be directly examined.
- Signs of Resolution: Decreased erythema, reduced swelling, and diminished pain on passive extension.
- Persistent Infection: If signs of persistent infection are present (ongoing purulent drainage, severe pain), irrigation is continued for another 24 hours.
Catheter Removal and Mobilization
- The dressings are removed again after the additional 24 hours (72 hours total) and the fingers are re-examined.
- If no residual signs of infection remain, the inflow catheter and the distal rubber drain are removed.
- A lighter dressing is applied that permits digital motion.
- Active Motion: Aggressive, early active motion exercises are begun immediately under the guidance of a specialized hand therapist. This is critical to prevent the formation of restrictive peritendinous adhesions.
- Prolonged Irrigation: If pain or purulent drainage persists beyond 72 hours, irrigation may be necessary for several more days, or the patient may require a return to the operating room for formal open debridement.
CONCLUSION
Postoperative closed irrigation remains a highly effective, tissue-sparing technique for the management of acute pyogenic flexor tenosynovitis. By meticulously placing the inflow and outflow tracts, avoiding excessive catheter insertion, and ensuring rigorous postoperative fluid management, the orthopedic surgeon can eradicate the infection while preserving the vital gliding mechanism of the hand. Careful patient selection is paramount; the surgeon must remain vigilant and ready to convert to an open drainage procedure if tendon necrosis or chronic loculations are encountered.
